
Abstract
BACKGROUND:
Obesity is thought to be a risk factor for cardiopulmonary diseases due to changed pulmonary mechanics. It also drastically lowers functional capability in both males and females. A routine physiotherapy program has been shown to be effective in the prevention and treatment of cardiopulmonary diseases. It also significantly increases functional capacity following coronary artery bypass grafting. However, the effect of a structured physiotherapy program in obese and non-obese patients has not been well explored. As such, the objective of this study is to determine the effect of a standardized physiotherapy program on pulmonary function and walking capacity in obese and non-obese patients undergoing coronary artery bypass grafting.
METHODS:
A prospective study was conducted on 50 obese (age 57.2
RESULTS:
At baseline, obese individuals had significantly lower pulmonary and physical functioning. On postoperative day 4, both groups deteriorated, although the obese group deterioration was worse, in most of the pulmonary parameters. On postoperative day 7, both groups improved, though the non-obese group improved at a faster rate. In contrary, it was observed that the obese group improved more rapidly in terms of functional capacity.
CONCLUSIONS:
The study indicated that the outcomes of a structured physiotherapy program following coronary artery bypass grafting were different for persons who were obese compared to those who were not. Adipose tissue variations surrounding the rib cage, diaphragm, and visceral cavity may account for the observed rate of change between the two groups. Therefore, it is apparent that a new strategy for managing obese individuals who have undergone CABG is required.
Introduction
Obesity is becoming increasingly prevalent in both emerging and developed countries [1]. According to the World Health Organization, excess body weight is the sixth most important risk factor determining global disease burden [2]. Over the last two decades, obesity has risen in emerging countries that have adopted a modern lifestyle characterized by decreased physical activity and excessive eating of inexpensive, energy-dense foods [3]. The number of obese people in Asia is increasing, and the rate of increase does not appear to be slowing [4].
Obesity rates among patients undergoing heart surgeries such as coronary artery bypass grafting (CABG) appear to follow those in the overall adult population and have risen dramatically in most industrialized countries over the last decade [5]. It is important to optimize strategies to offer quality and efficient care because CABG outcomes vary depending on patient characteristics such as age and gender, as well as the presence and existence of co-morbid conditions. In addition, pulmonary function declines significantly following CABG surgery. The surgical procedure may play a role in the development of restrictive pulmonary impairment [6, 7, 8, 9, 10]. Jenkin et al. [11] observed that even patients with modest obesity who are awaiting CABG have dramatically reduced lung capacities. Obese individuals frequently complain of exertional dyspnea and exercise intolerance [12]. Thus, obese patients undergoing CABG are at a greater risk of developing postoperative pulmonary dysfunction, posing significant challenges for the physician and rehabilitation practitioner during the postoperative period [13]. Obesity appears to increase the risk of perioperative problems in all organ systems, not only the heart [5]. Additionally, studies have shown that obese people have lower levels of physical function than non-obese people [14, 15]. Body mass index (BMI) has been shown to be inversely related to functional ability in a variety of individuals of diverse ages [16]. Obesity has a substantial impact on daily activities like walking, bending, and climbing stairs [17]. The symptoms of coronary heart disease, such as angina and exertional dyspnea, limit their physical activity [18]. Another factor that contributes to inactivity and deconditioning is fear of the repercussions [19, 20]. As a result, people who are obese are at greater risk of developing functional impairment as well as smaller lung capacities.
Postoperative pulmonary dysfunction can be prevented and treated with a standard physiotherapy program. It has been shown to significantly improve functional capacity and overall quality of life following CABG [21, 22, 23]. Despite the well-established additional deleterious effects of obesity, there is a dearth of research regarding the comparative response of obese and non-obese patients to a structured physiotherapy program following CABG, particularly in the inpatient phase. Therefore, the purpose of this prospective study is to assess the effects of a structured physiotherapy program on ventilatory mechanics and exercise tolerance in obese and non-obese patients who have CABG.
Methods
Study participants and data collection
The Research Ethics Committee of Jazan University gave its approval to this study (Ref No: 05/JUREC/14PT.2020). Prior to participation, each participant signed an informed consent form. All experiments were carried out in line with the Helsinki Declaration. The TIDieR (Template for Intervention Description and Replication) Checklist is included as Appendix 1. A prospective study was conducted on 50 consecutive individuals (26 obese, 24 non-obese). People aged 70 years or older, or who had any orthopedic or neurological difficulties were excluded from the trial. People were informed about the trial and consented in writing. Following enrollment, participants were placed into two groups according to their BMI. Participants in Group A were obese, defined as having a BMI of
Subjective ratings and spirometry data were taken at baseline. All spirometry tests were performed in the sitting position using the Vitilograph 2120 in accordance with established guidelines [24, 25]. The best of three trials was recorded, and there was a one-minute break between each trial. A posttest spirometry was performed on day 4 and 7 postoperatively. A six-minute walk (6-MWT) test was conducted at baseline and on day 7 postoperatively [26]. Patients were advised to walk back and forth on the walking path of 30 m indoor corridor, at their own pace for 6-MWT. Patients were recorded performing a 6-minute timed walking using a stopwatch on a smartphone. When 4 and 2 minutes remained in the test, prompts were offered. We utilized the following standardized prompt: “You’re down to the final two (or four) minutes. You are doing an excellent job. You may accelerate or decelerate at any time, maintain the same pace, or take a break if necessary. Simply attempt to travel as much distance as possible in the remaining time. You are doing an excellent job.” After six minutes, the participant’s total distance traveled was recorded, along with a Borg dyspnea scale rating. The total distance that was walked was recorded after being measured to the nearest meter. The 6MWT is widely regarded as the gold standard for objectively measuring submaximal exercise capacity [27]. It also has great repeatability for cardiac populations (ICCs of 0.97, 0.91, and 0.90, respectively) [28, 29, 30].
A structured physiotherapy programs
A structured physiotherapy programs
After completing the 6MWT, we also assessed any exertional dyspnea with a modified Borg scale [31]. We informed patients that a score of 0 on the modified Borg scale shows no dyspnea, 1 indicates very faint dyspnea, 2 indicates weak, 3 indicates moderate, 4 indicates relatively strong, 5 indicates strong, and 10 reflects the worst dyspnea the patient could envision or had ever experienced. As soon as 6MWT was complete, we asked the patients how they felt about it.
All patients were put to general anesthesia for surgery, which was carried out under moderate hypothermia (28
Inpatient physiotherapy program
A qualified physical therapist expertise in cardiopulmonary rehabilitation administered a structured physiotherapy program from day 1 to day 7 in both groups. All the interventions were given at University Hospital, Jazan, Saudi Arabia. Active-assistive to active range of motion movements to major muscle groups, active ankle movement, and scapular elevation/depression are all part of the inpatient physiotherapy program. In addition to that, other exercises involving deep breathing were introduced. In addition to that, the patient was given the task of walking a distance of 100 feet while being monitored by a physiotherapist. These exercises were performed in a seated position at first, and later progressed to being performed in a standing position. At first, each exercise was performed between five and ten times, and subsequently the number of repetitions increased to between ten and fifteen. Details of exercise protocol is presented in Table 1. The component of these exercises has been used previously in patients with post-CABG [32].
Statistical analysis
The descriptive variables are expressed as mean
Results
Demographic statistics
Demographic statistics
Note: BMI, Body mass index;
Fifty subjects were analyzed for the study, with 26 people in group A (obese adults, the mean BMI: 33.64
Changes in outcomes from Pre- to Post- operative stages in each group
Note: VC: Vital capacity; FVC: Forced vital capacity; FEV1: Forced expiratory volume in one second; PEF: Peak expiratory flow; 6-MWT: 6-minute walk test;
Percentage changes in outcomes in each group
Note: VC: Vital capacity; FVC: Forced vital capacity; FEV1: Forced expiratory volume in one second; PEF: Peak expiratory flow; 6-MWT: 6-minute walk test;
Table 3 depicts changes in outcomes in each group from baseline- to posttest. An independent t-test found that numerous spirometry measures (VC, FVC, FEV1, and PEF) were substantially lower in the obese adults than in the non-obesity adults at baseline. Additionally, obese individuals covered much less distance throughout the 6-MWT than non-obese individuals. On posttest data, numerous spirometry values (VC, FVC, FEV1, and PEF) were considerably lower in obese individuals than in non-obese individuals. Additionally, on posttest data, the obese sample covered significantly less distance during the 6-MWT than the non-obese population.
Changes (%) in forced vital capacity (FVC) from baseline to postoperative day 4 and 7.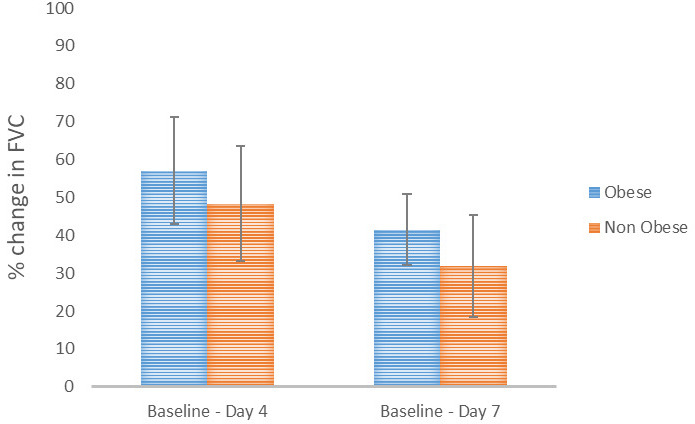
Changes (%) in peak expiratory flow (PEF) from baseline to postoperative day 4 and 7.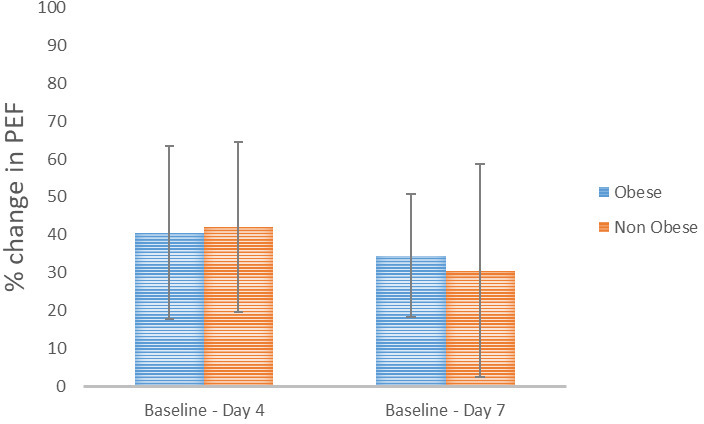
Changes (%) in 6-minute walk test distance from baseline to postoperative day 7.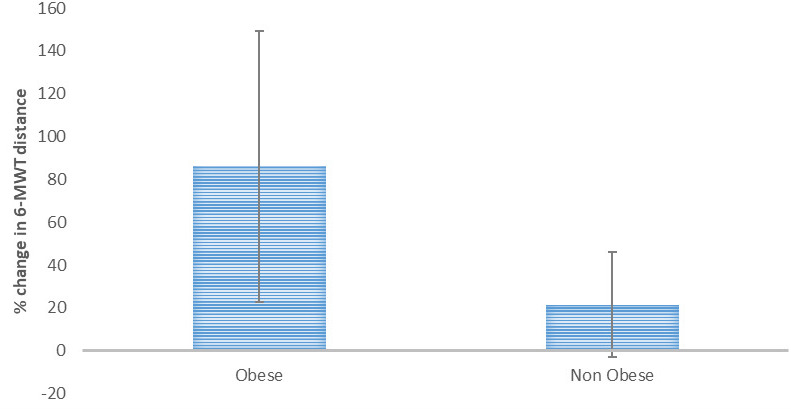
The current investigation discovered that various spirometry measurements and the 6-MWT were significantly different across the groups at baseline. Thus, a percentage difference between all variables was determined to rule out decrement or increment in any result relative to baseline values (Table 4). While both groups experienced a drop in most spirometry data on the post-operative day 4, the obese sample experienced a significantly greater reduction in FVC (Fig. 1) and PEF (Fig. 2). Spirometry data continued to decline in both groups on postoperative day 7, but the obese sample showed a considerably higher decline in FVC (Fig. 2). On postoperative day 7, both groups demonstrated an increase in walk distance covered during the 6-MWT. In obese subjects, the percentage improvement on the 6-MWT was much greater (Fig. 3).
Obese individuals are believed to be at an increased risk of developing cardiovascular disease. Obesity is a risk factor for coronary artery disease because it is related with an increased prevalence of metabolic syndrome, dyslipidemias, and a sedentary lifestyle. Standardized physiotherapy programs significantly reduce cardiovascular death by improving body weight and functional capacity [33, 34, 35, 36]. The purpose of this study was to determine the effect of a structured physiotherapy program on the ventilatory mechanics and exercise tolerance of obese and normal-weight individuals having CABG. The demographic variables (age and height) of obese and non-obese patients were found to be statistically insignificant, indicating that both groups were comparable in terms of change in lung volumes in relation to demographic parameters.
In the current study, preoperative mean values for VC, FVC, FEV1, and PEF were significantly lower in obese patients than in non-obese patients, while mean values for FEV1/FVC and FEV1-25 were not significantly different between the two groups. Jenkins et al. [11] observed a similar finding when they examined the impact of modest obesity on lung volumes in individuals after CABG. They discovered that patients with mild to moderate obesity had lower VC and FRC levels. Akdur et al. [13] also examined pulmonary volumes in obese female patients following CABG and discovered comparable results. These alterations in lung volume have been ascribed to increased intra-abdominal adipose tissue mass loading and splinting of the diaphragm. This impairs the chest wall’s mechanical qualities, resulting in a decrease in chest compliance and prevents the diaphragm from fully extending. The BMI range of obese people in this study was 30–35 kg/m
Lung volumes were measured on postoperative day 4 and day 7 to compare the benefits of a structured physiotherapy program between obese and non-obese samples. On postoperative day four, VC, FVC, FEV1, and PEF significantly decreased in the obese group compared to the non-obese group. While the FEV1/FVC ratio increased in both groups, there was no statistically significant difference between them. On the fourth postoperative day, lung volumes were lowered by a mean of 56% in obese patients and 48% in non-obese patients, respectively, compared to preoperative values. Following that, on day 7, it improved slightly but remained below preoperative values. Lung volumes remained much lower in the obese than in the non-obese, by a mean difference of 41% in the obese and 32% in the non-obesity, compared to their respective preoperative values. Vergas et al. [37] corroborated these findings. They reported a significant decline in pulmonary function following CABG. Immediately following surgery, lung volumes dropped and then improved, but on the tenth postoperative day, lung volumes were 30% below preoperative values. Shenkman et al. [38] also discovered similar results. They concluded that for at least 3.5 months following heart surgery, lung function deteriorates considerably. They stated that the mechanism underlying the impairment of pulmonary function is unknown, but that bronchoconstrictive effects of medication, postoperative surgical pain, phrenic nerve cold injury, dissection of the internal mammary artery, and mechanical effects of median sternotomy could all be contributing factors [6, 10, 38, 39, 40, 41].
The mean difference in FVC deterioration on day 4 and day 7 was substantially greater in the obese group than in the non-obese group in the current study. These findings indicate that, while both groups experienced a significant decrease in lung volume, the non-obese group experienced a greater increase in post-operative PFT values. Initially, it was observed that obese patients had a greater reduction in lung volumes on postoperative day 4 when compared to their preoperative values. On postoperative day 7, both groups gradually improved their lung volumes. The obese group improved less than the non-obese group. These findings were corroborated by research conducted by Akdur et al. [13]. Additionally, they concluded that the obese group experienced a greater decline in post-operative PFT values than the non-obese group. It has been suggested that respiratory muscle weakening may play a role in the initial postoperative loss of restricted lung function. Obese patients’ respiratory muscle strength and endurance are diminished, resulting in early respiratory muscle exhaustion. This could explain why obese people experience a greater drop in lung volume throughout the postoperative period [12]. Additionally, obese patients have decreased pulmonary volumes preoperatively, which contributed to a greater drop in lung volumes in the postoperative period compared to non-obese patients.
Additionally, the obese group’s functional ability was shown to be much lower than that of the non-obese group. At the baseline, the mean distance traveled during a 6-MWT was significantly different between obese and non-obese participants in the current study. Larsson and Reynisdottir [42] shown that obese individuals walked significantly less than non-obese individuals during the 6-MWT. Similarly, Bautista et al. [43] found that obese individuals had considerably shorter 6-MWT distances than non-obese individuals. As a result, it seems as though the obese patients travelled less distance due to their higher body mass.
Postoperative data of the 6-MWT indicated that obese patients had significantly shorter mean 6-MWT distances than non-obese patients. The obese group had a substantially larger mean percentage difference in 6-MWT distances between preoperative and postoperative day 7. While obese individuals advanced more functionally than non-obese patients in the postoperative days following CABG, their mean distance traveled during the 6-MWT was statistically smaller. The detrimental effect of obesity on exercise physiology is widely recognized. It should be emphasized that being overweight might impair walking and increase workload [44]. Obesity increases the exertion required to perform a given quantity of exercise, resulting in a lower 6-MWT distances in patients with a greater body mass index or body weight [45].
Limitations and clinical implications
Our study has certain possible limitations, including the fact that the pulmonary function and 6-MWT assessments did not contain other variables such as a description of the patient’s physical activity level before to surgery, which may influence the patient’s functional status. Additionally, it was a single-center study without a control group. Furthermore, gas exchange measurements were not taken during exercise. Therefore, the findings of this study should be interpreted considering the common factors and barriers that affect all physiotherapy program, such as the inability to objectively monitor patient compliance with educational and lifestyle counseling, as well as the potential confounding effects of concurrent medication use. Previous studies have discovered that the decreased lung volume in the obese adults could be attributed to both the accumulation of fat throughout the body and the increase in BMI [46, 47, 48]. When it comes to adiposity markers, abdominal adiposity is more relevant than weight and BMI, as mentioned by Ochs-Balcom et al. [49] and their findings on how it impairs lung function. Some researchers have confirmed that the gender difference in the distribution of body fat has an effect on pulmonary function [48, 49]. Women tend to have their fat distributed more peripherally, whereas males tend to have theirs concentrated more centrally [48, 49]. Since participants of both genders were included in the current study, it is possible that their differences could have affected the results. Therefore, future studies are warranted to determine if the gender plays a role in the results of this study.
Conclusions
The results of this study show that recovery of pulmonary function and functional ability following CABG is not comparable in obese and non-obese individuals undertaking the same standardized physiotherapy program. At baseline and follow-up, obese individuals had lower spirometry and 6 MWT scores than non-obese individuals. Possibly, the mass burden of adipose tissue surrounding the ribcage, the diaphragm, and the visceral cavity contributes to the disparities in the change in outcomes between the two groups. As a result, a novel strategy for the treatment of obese patients who have undergone CABG is required.
Ethical considerations
The Research and Ethics Committee, Department of Physical Therapy, Jazan University, Saudi Arabia gave its approval to this study (Ref No: 05/JUREC/14PT.2020 dated 21
Trial Registry Number: NCT05357937; https://cli nicaltrials.gov/ct2/show/NCT05357937.
Funding
No funding received for this paper.
Supplementary data
The corresponding author can provide access to the patient data that supported the study’s conclusions upon request.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors have declared that they do not have any competing interests.
Appendix 1
The TIDieR (Template for Intervention Description and Replication) checklist
Item
Item
Where located
number
Primary paper (page or appendix number)
Other
BRIEF NAME
1.
Provide the name or a phrase that describes the intervention.
1
WHY
2.
Describe any rationale, theory, or goal of the elements essential to the intervention.
3–4
WHAT
3.
Materials: Describe any physical or informational materials used in the intervention, including those provided to participants or used in intervention delivery or in training of intervention providers. Provide information on where the materials can be accessed (e.g. online appendix, URL).
4–5
4.
Procedures: Describe each of the procedures, activities, and/or processes used in the intervention, including any enabling or support activities.
4–5
WHO PROVIDED
5.
For each category of intervention provider (e.g. psychologist, nursing assistant), describe their expertise, background and any specific training given.
5
HOW
6.
Describe the modes of delivery (e.g. face-to-face or by some other mechanism, such as internet or telephone) of the intervention and whether it was provided individually or in a group.
5
Table 1
WHERE
7.
Describe the type(s) of location(s) where the intervention occurred, including any necessary infrastructure or relevant features.
5
WHEN and HOW MUCH
8.
Describe the number of times the intervention was delivered and over what period of time including the number of sessions, their schedule, and their duration, intensity or dose.
Table 1
TAILORING
9.
If the intervention was planned to be personalised, titrated or adapted, then describe what, why, when, and how.
N/A
MODIFICATIONS
10.
If the intervention was modified during the course of the study, describe the changes (what, why, when, and how).
N/A
HOW WELL
11.
Planned: If intervention adherence or fidelity was assessed, describe how and by whom, and if any strategies were used to maintain or improve fidelity, describe them.
N/A
12.
If intervention adherence or fidelity was assessed, describe the extent to which the intervention was delivered as planned.
N/A