
Abstract
BACKGROUND:
The knee is one of the most common injuries in sports. However, the incidence of knee injuries can be decreased by enhancing balance and neuromuscular control.
OBJECTIVE:
The aim of this systematic review and meta-analysis was to investigate how injury prevention programs (IPPs) that include balance training influence knee injury rates in athletes.
METHODS:
Data were obtained from different databases (1985–2021). Only randomised controlled trials that used IPPs that include balance training, were considered. Two investigators extracted data from the qualifying documents. The critical outcome data elements derived from the included studies were the number of ACL/knee injuries, ACL/knee injury rates, exposure hours, compliance rate, and follow-up duration.
RESULTS:
Compared to the control groups, those who participated in the IPP had a 54% lower risk of knee injuries per 1000 hours of exposure (IRR 0.457 (95% CI 0.346–0.603),
CONCLUSIONS:
IPPs that include balance training may reduce the risk of knee injuries.
Introduction
Severe knee injuries such as anterior cruciate ligament (ACL) tears and meniscus lesions are common in sports [1] and can lead to time loss with long absences [2]. Over the last two decades, many epidemiological studies have investigated the incidence and mechanism of injuries among amateur [3, 4] and professional athletes [5, 6, 7, 8, 9, 10]. Professional sports such as soccer are linked to a higher rate of ACL injuries than other sports [11, 12]. Generally, male players have a significantly lower risk of ACL injuries than female players [13]. Other risk factors for ACL injuries include match play, age [13], and previous knee injuries [5, 9, 14].
Moreover, increased physical impact on sports with rapid direction changes results in higher injury rates [15, 16]. IPPs designed to prevent knee injuries have been investigated and published several times [16, 17, 18]. These IPPs are used along with warm-up and training programs to prevent common musculoskeletal injuries [17, 19], Special programs have been published for knee injury prevention in different types of sports [20]. Moreover, specific risk factors and mechanisms of severe knee injuries have been recognized and led to the development of neuromuscular interventions and some specific IPPs programs [18].
ACL is one of the most injured ligaments of the knee joint worldwide [21]. Of these injuries, 88% have been shown to be non-contact in nature [22], without any direct physical contact to the athlete’s knee. In addition, 48% to 96% of ACL injuries occur in non-contact episodes in young athletes [23]. However, increasing medical treatment costs, especially in females, are significantly higher for knee injuries than in males [24].
Neuromuscular training (NMT) programs can significantly decrease the risk of knee injuries among male and female athletes [25, 26]. Balance training exercises included in injury prevention programs (alone or as part of the programs) reduced ankle injury rates among soccer players [27]. In particular, balance training has effectively reduced non-contact ACL injuries in soccer players, especially in female athletes [25]. Several randomised control trials have been conducted to evaluate the effectiveness of balance exercises on the severity and incidence of knee injuries in athletes [28, 39, 30, 31, 32, 33, 34, 35, 36, 37]. An investigation of a structured warm-up program that includes balance exercises to reduce knee injuries in young athletes revealed fewer knee injuries in the intervention group than in the control group [28]. In another study of 1892 female players aged 13 to 17 years, 837 athletes were in the control group and 1055 in the intervention group, showed that a comprehensive warm-up program that includes balance exercises reduced the risk of overuse, severe and overall injuries in the intervention group [29]. Similar results were obtained in a cluster randomised trial that included an intervention group (380 participants) and a control group (364 participants) of Canadian male and female athletes aged 12 to 17 years; the intervention group were instructed to apply a structured warm-up program that included balance exercises throughout the 2010 competitive season [30]. A key finding was that the program effectively decreased the rate of knee injury in the intervention group. Another study by Waldén et al. [31]was conducted to evaluate the effectiveness of the NMT program, including balance exercises, in decreasing the number of acute knee injuries in adolescent female athletes. They found that the NMT program reduced the rate of knee injuries in this group. A reduction in knee injury rates was also found in studies with different IPPs known as the FIFA 11
In contrast, no differences between the groups (the intervention and control group) were reported in other studies, and there was no reduction in the rate of knee injury across the players [32, 34, 37]. Given the inconclusive findings in the extant literature, there is a need to evaluate the role of IPPs that include balance training exercises in preventing or minimizing knee injury compared with balance training alone, using injury incidence rates to calculate its effectiveness. Moreover, balance exercises have been used widely in reducing injury rates and enhancing the NMT [31]. However, none of the previously mentioned studies assessed the effectiveness of balance training alone in reducing knee injuries in athletes. Hence, this systematic review and meta-analysis of randomized controlled trials (RCT) aimed to investigate how knee injury rates are influenced by IPPs that include balance training compared with the control group implemented balance training alone in athletes. This would provide evidence-based insights into whether balance training exercises should be included in IPPs for athletes to prevent or reduce such injuries or implemented alone. Moreover, this review will investigate Injury prevention programs including balance exercises with compliance and follow-up to reduce the incidence of knee injuries in athletes.
Materials and methods
Study design
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were used to conduct the systematic review and meta-analysis in the current literature [38]. A protocol was registered in the International Prospective Register of Systematic Reviews, PROSPERO (CRD42020186706) “retrospectively registered”.
Search strategy
Two investigators searched for relevant articles using electronic databases such as the Cochrane Library, PubMed, Web of Science, MEDLINE, and PEDro. The systematic search covered the data collection period from 1985 to 2021. To conduct electronic searches, the following keyword combination was used: (strengthening) OR (proprioceptive training) OR (neuromuscular training) OR (injury prevention programs) OR (FIFA 11
Eligibility criteria
Studies were eligible for inclusion if they (1) were cluster randomized controlled trials (CRCT) or individual randomized controlled trials (RCT) of sports IPPs that included balance training; (2) had a balance exercise intervention group and a control group for comparison; and (3) were conducted on athletes of any age, gender, or skill level; (4) studies in which at least two of the following were reported: number of knee/ACL injuries, knee/ACL injury rate, and exposure hours; and (5) studies that were conducted entirely in English.
The following studies were excluded: (1) Case studies or case series, retrospective evaluations, observational or cross-sectional studies; (2) Participants’ compliance was not reported; (2) only performance or physical measurements were reported but not knee/ACL injury rates or exposure hours; and (3) studies with missing data without a response from the corresponding to a request for missing data when contacted.
Data synthesis
Inclusion procedure
In the initial screening, two investigators independently evaluated the articles’ eligibility based on their titles and abstracts. The full text of qualifying studies was collected after duplicates were deleted, and publications that did not meet the inclusion requirements were omitted. If there were disagreements, a third reviewer was consulted to reach an agreement. Following the identification of an initial list of included studies, reference monitoring of such studies and previous reviews were screened for additional studies that may be included in this systematic review. The process for inclusion is summarized in (Fig. 1).
Flow diagram of the systematic steps in articles screening for inclusion.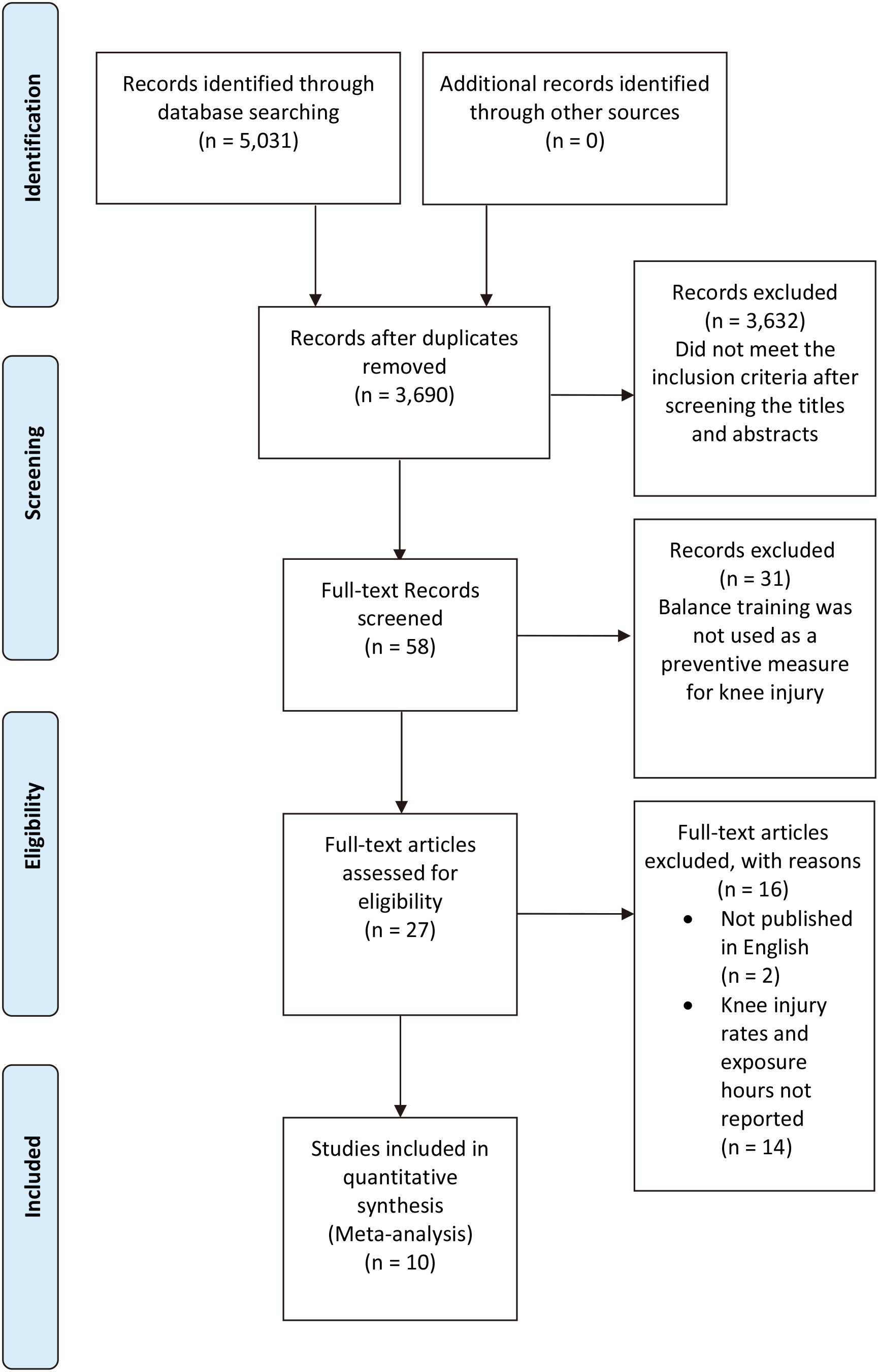
Endnote version X8 (Thomson Reuters, Philadelphia, PA, USA) was used for collecting studies, scanning, removing duplicates, and managing references. Before being analyzed by Comprehensive Meta-Analysis version 3 (CMA V3), the critical outcome results from each included study were extracted and collected in Microsoft Excel (Microsoft Corp) for Mac (Biostat, Inc., Englewood, NJ, USA).
Data extraction
Two investigators used a data extraction form to extract data from the full texts of the qualifying documents. The critical outcome data elements derived from the included studies were the number of ACL/knee injuries, ACL/knee injury rates, exposure hours, compliance rate, and follow-up duration.
Meta-analysis
The CMA V3 was used to enter and evaluate extracted data for the meta-analysis and subgroup analysis. The meta-analysis was based on the total number of exposure hours. Subsets of studies focused on the specificity of IPPs, and gender were subjected to subgroup meta-analysis for each main category. The random-effects model was used since the experiments involved a wide range of populations, contexts, and balance training doses and procedures. The injury rate was used to adjust the variations in athletes’ exposure hours from each included study [39] as it is preferred in sports science for estimating injury incidence. This injury rate is calculated by multiplying the number of injuries by the total risk period and then by 1000. The injury risk ratio (IRR) was calculated by dividing the intervention group’s injury rate by the control group’s injury rate. IRR less than one and confidence intervals (CIs) less than 1 indicate a positive intervention effect; for example, an IRR of 0.80 indicates a 20% reduction. The I
Publication bias
A funnel plot was developed to assess the risk of possible publication bias. The funnel plot asymmetry was evaluated using Egger’s test [41]. The Trim and Fill method [42] by Duval and Tweedie was used to see whether the overall IRR estimate needed to be adjusted for publication bias based on the filled studies.
Methodological quality scores of the included studies
Methodological quality scores of the included studies
1: eligibility criteria; 2: random allocation; 3: concealed allocation; 4: baseline comparability; 5: blinded participants, 6: blinded therapists; 7: blinded assessors; 8: adequate follow-up; 9: intention-to-treat analysis; 10: between-group comparisons; 11: point estimates and variability.
Each study’s methodological quality was assessed independently by two investigators. The 11 criteria of the Pedro scale recommended were used to assess the quality criteria and the risk of bias (Cashin & McAuley, 2020) [43]. When a criterion is clearly satisfied, each item is awarded a point. The total possible score is ten. A score of
Definitions of athlete workload and injury
Athlete workload
Athlete workload was defined as the number of active hours spent by athletes in training or competition during the study period [45].
Knee & ACL injury
Knee/ACL injuries are defined as ones that prevent a player from participating in the next game or training session. This was according to a statement issued by a group of sports epidemiologists [44].
Results
Study characteristics
All the articles included cluster randomized controlled trials in the following locations: Three in Norway [28, 29, 37]; and one of each in the Netherlands [32]; Sweden [31] Germany [34]; Nigeria [33]; the USA [35]; Australia [36]; and Canada [30]. Five studies included only male participants, 32–36 and four included female participants [28, 29, 31, 37], with just one study, including both male and female participants [30].
With regard to sporting level, two studies involved youth soccer players aged 13 to 17 years [29, 37], and there are one of each included as follows: collegiate soccer players aged 18 to 25 years [35], youth soccer players aged 13 to 18 years [30], adolescent soccer player age 12 to 17 [31], youth soccer players age 14 to 19 years [33], amateur soccer players age 14 to 35 years [36], adult soccer players age 24 to 25 years [32], adult soccer players age 43 to 45 years [34], and youth handball players age 15 to 17 years [28].
Two of the studies used the ‘11’ [32, 37], three used the 11
The programs ranged from six to twelve months, and the warm-up exercises differed Eight studies were based on their regular warm-up routine [28, 29, 31, 35, 37]; one had regular warm-up exercises including static and dynamic stretching, aerobic workouts, and stretches [30], and one had a pre-training from the FIFA 11
All studies conducted using IPPs that involve balance training exercises as a part of their programs were split into two subgroups. After evaluating the eligibility process, general IPPs studies that included balance training with other types of training exercises were determined to be in the FIFA 11
Characteristics and moderators of the included studies
Characteristics and moderators of the included studies
Abbreviations: M
Injury rates per 1000 hours of exposure in the included studies’ intervention and control groups
The primary articles found 5,031 studies, of which 5,021 were excluded due to duplication, criticism, and review. After applying our inclusion and exclusion criteria RCT/CRCT, balance exercises, compliance, and duration, ten additional studies remained. If more information was required, the corresponding authors of the studies were contacted. At least three corresponding authors double-checked all the studies before being included in our meta-analysis. References from the included studies were also checked to ensure that all articles that met the requirements for inclusion were found. Finally, the analysis included ten studies. Table 2 lists the characteristics of the included studies, while Table 3 displays injury rates per 1000 hours of exposure in the control and intervention groups of the included studies.
Pooled injury estimates
The ten studies covered data from 14,063 individuals and 344 knee injuries over 417,189 exposure hours. As shown in Table 3, the combined IRRs for the intervention and control groups are 5.84 and 8.56 injuries, respectively, per 1000 hours of exposure.
Meta-analysis results
Reduction in knee injuries
Compared to the control group, those who participated in the IPP had a 54% lower risk of knee injury soccer and handball per 1000 hours of exposure (IRR 0.457 (95% CI 0.346–0.603),
Forest plot illustrating the effect of IPPs that include balance training versus controls on knee (top) and ACL (bottom) injury risk ratio. IPPs 
In comparison to the control group, those who participated in the IPP had a 60% lower risk of ACL injury alone per 1000 hours of exposure (IRR 0.401 (95% CI 0.215–0.750),
In comparison to the control group, those who participated in the IPP had a 55% lower risk of knee injury in soccer per 1000 hours of exposure (IRR 0.446 (95% CI 0.321–0.619),
Forest plot illustrating the effect of IPPs that include balance training versus controls on knee injury risk ratio in soccer.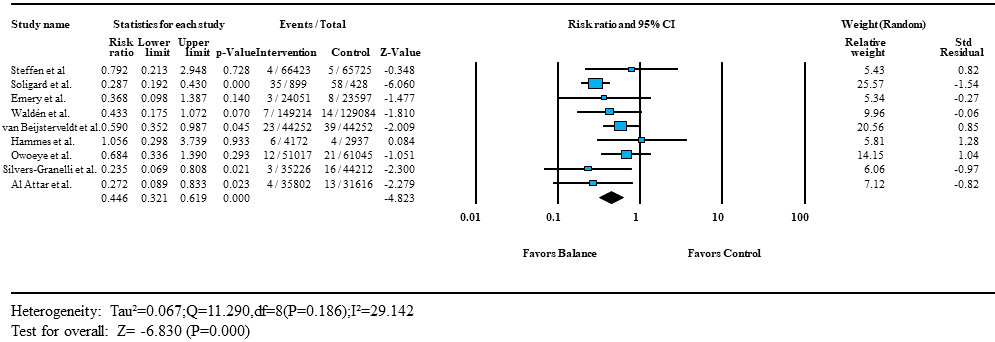
The IPPs display a reduction in knee injuries per 1000 hours of exposure, 49% of knee injury reduction among both males and females [IRR 0.507 (95% CI 0.320–0.804),
Forest plot illustrating the effect of IPPs that include balance training versus controls on knee injury risk ratio in: (top) males and females; (middle) males and (bottom) females.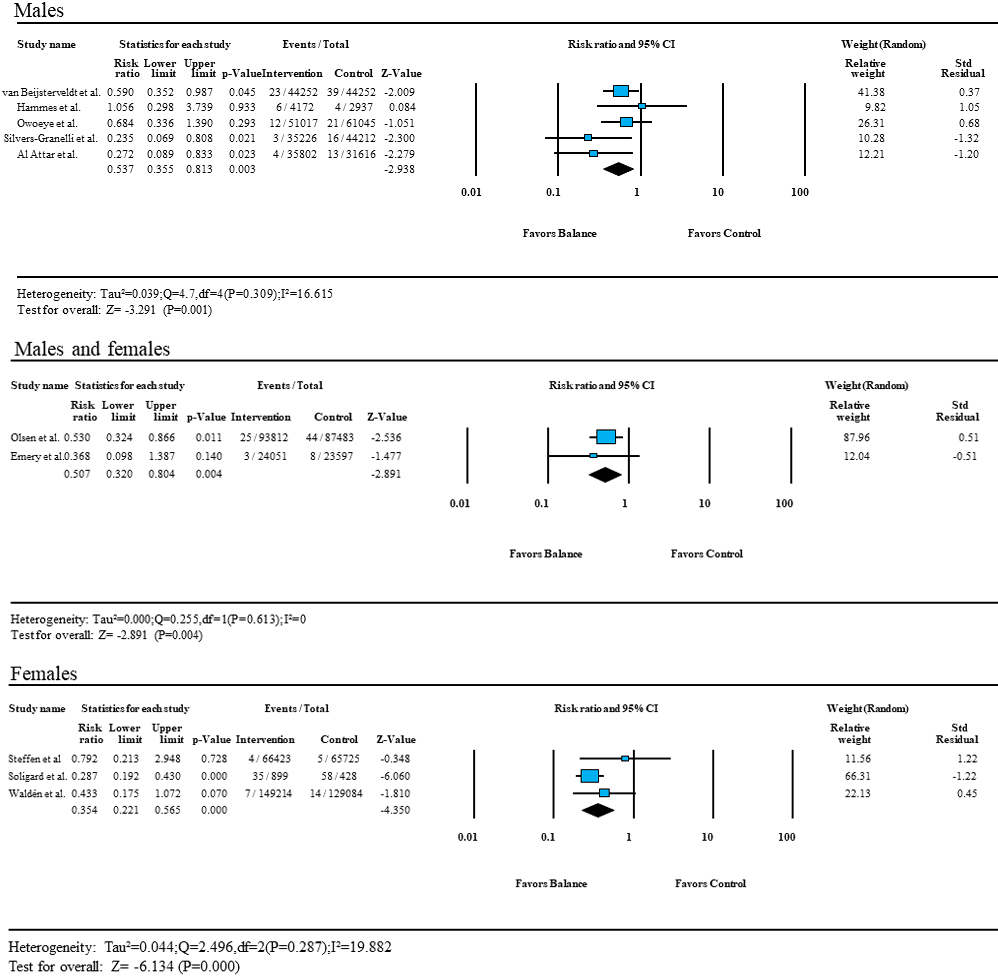
Funnel plot based on the study standard error and log risk ratio to assess publication bias. Circles indicate the study’s estimated point based on the procedure by Duval and Tweedie. The pooled estimate injury risk ratio (IRR) is presented as a diamond with the width corresponding to the CI, and the vertical line (centre of the diamond) is the overall effect.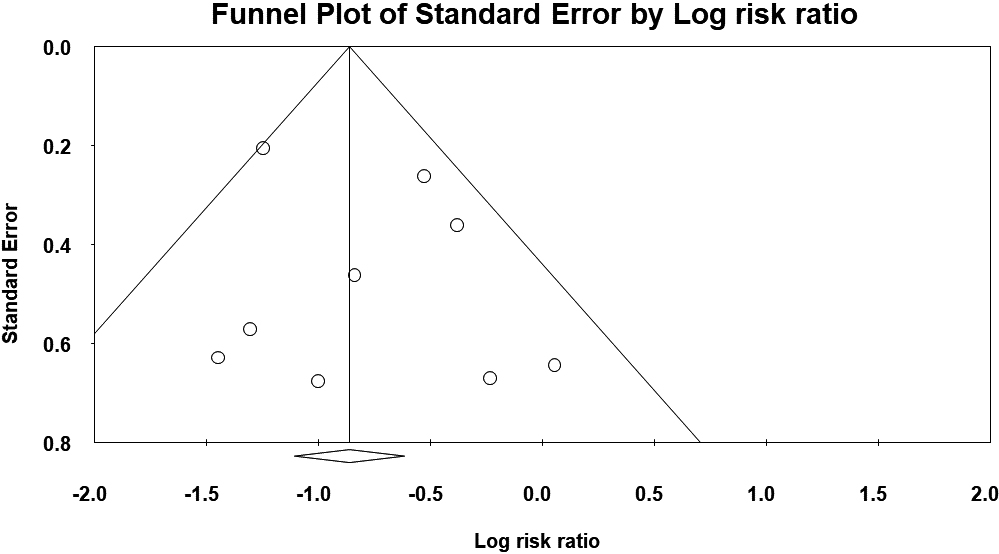
The bias is unlikely to exist because the asymmetry was small when looking at the funnel plots (Fig. 5). The Egger test confirms symmetry with a value of 0.73 (95% CI
Discussion
To date, this is the first systematic review and meta-analysis of the effectiveness of IPPs that include balance training exercises in reducing the incidence of knee injuries in athletes
Main findings
According to this systematic review and meta-analysis of ten randomized controlled trials, balance exercises alone or in conjunction with IPPs successfully reduce the risk of knee injuries in soccer players. The important objective of the current study was the exposure-based knee incidence rates. The analysis revealed that IPPs that involve balance exercises substantially decreased the risk of knee injuries in soccer players by 55% based on total exposure hours, IPPs that include balance exercises reduced the knee injury rates by 54% in soccer and handball, IPPs that include balance exercises reduced the ACL injury rates by 60%, IPPs that includes balance exercises reduced the knee injury rates by 49% in male-female combined. The IPP that includes balance exercises reduced the knee injury rates by 46% in males, and IPP that includes balance exercises reduced the knee injury rates by 65% in females.
Subgroup analysis
IPPs that include balance training exercise (FIFA 11
IPP versus specific balance training)
The FIFA 11
In sports research studies, the incidence rate is the preferred and more meaningful indicator of injury incidence because it can accommodate differences in athletes’ exposure period and estimate injury risk [39, 46]. Furthermore, it provides a valuable basis for studying the predictability of risk factors and the efficacy of preventive measures [39], as Soomro et al. [47] and Al Attar et al. [45] suggested in their meta-analyses that the athlete’s injury risk can be affected by the player’s exposure period. Indeed, it has been found that the athlete’s risk of injury was associated with increased exposure to sports [48, 49]. As a result, assessing the effectiveness of IPPs using athletes’ exposure-based incidence rate is more reliable and powerful.
Male versus female
The current review findings support the idea that IPPs that include balance training exercises can help female soccer players avoid knee injuries. When comparing studies with male subjects [32, 33, 34, 35, 36] to studies with females only [28, 29, 31, 37], IPPs that involve balance training exercises reduced the knee injury risk in females more than males. The combined findings involving males and females revealed a 50% reduction in knee injury risk in either case [30]. As a result, more research is needed to determine the effectiveness of IPPs, including balance training exercises in decreasing ACL injuries in male and female soccer players.
Balance training protocol and compliance
It was challenging to make a recommendation for the best balance training protocol because the duration, frequency, and exercise parameters differed between the included studies. As a result, more research is required to assess the dose-response relationship and the best approach for designing a balance training program to avoid knee injuries. However, when conducting training sessions 2–3 times a week for 6–12 months, it is believed that a valuable result is obtained [30, 33, 35, 36]. It has been hypothesized that in order to achieve a preventive effect, the training session must last at least 10 minutes [50], performed at least once a week for 3–12 months [50, 51], and a higher number of preventive sessions will result in additional benefits [45].
Injury rates are influenced by the degree of compliance with IPPs [52]. According to the results of the two studies, the risk of injury decreased as enforcement improved [53, 54]. Compliance has also been shown to influence the prevention program’s effectiveness [55]. The studies included in the current meta-analysis reported a moderate to excellent degree of compliance 60–100% to the preventive programs used [28, 29, 30, 31, 32, 33, 34, 35, 36], except for one study which reported low participants’ compliance 52% to the targeted prevention program [37]. Regardless of the prevention program used, all moderate to high compliance research showed that the intervention group experienced fewer injuries than the control group [28, 29, 30, 31, 32, 33, 34, 35, 36]. Just four research [30, 33, 35, 36] with moderate to high enforcement (60–85%) displayed a significant reduction in knee injuries among soccer players. Therefore, due to the differences between previous literature and our findings regarding the relationship between athletes’ compliance and the reduction of injury risk, further studies are needed to determine how compliance influences the efficacy of IPPs that include balance training exercises in reducing knee injury risk among soccer players.
History of prior knee injuries
Since most research did not differentiate whether participants had a history of knee injury or not, it was challenging to perform additional studies based on this information. More cluster-randomized controlled trials are needed to compare the prophylactic effect of balance training in soccer players with and without a history of a knee injury.
Directions for future research
According to this meta-analysis, balance exercises can potentially decrease knee injury rates in soccer players. As a result, teams that use balance activities in their preparation would have a significant advantage. A further study evaluating the implementation of balance training exercises as a preventive technique for knee injuries in soccer players with and without a knee injury history is recommended. Moreover, the same study would be recommended to be applied in the future comparing the use of balance training in sports other than soccer to see whether balance exercises successfully prevent knee injuries in other athletic populations.
Strengths and limitations
This study included subgroup categories such as sex (male versus female) to understand better the factors affecting knee injury risk. The high methodological standards used in this study, including the use of exposure-based incidence rates, made this meta-analysis special. In addition, all eligible studies with missing data were initially included, as their authors were contacted to provide specific data on soccer players if they only reported general results, such as knee injury rate for multiple sports. Furthermore, as the funnel plot appeared symmetrical and did not show deviation from the funnel shape, statistical analysis indicated no evidence of publication bias.
However, there are some limitations. The first limitation is that only studies published in English were considered. However, we did not find any non-English relevant studies, and language limits do not always affect or bias the findings of systematic reviews [56]. Second, there were no clear requirements to determine the level of competition, and the review included data from athletes of all ages, genders, and levels. Third, other training elements of the preventive programs may influence the reduction rate of knee injuries, possibly confounding the preventive effect of balance training exercises. Fourth, selection bias (missing multiple-sport context), confounding more broadly, generalizability, and lack of consideration of competition vs training/practice contexts. As a result, this analysis was created to provide research that looked at the preventive effects of balance exercises independently and as part of other preventive programs.
Conclusions
This is the first meta-analysis to show that balance exercises, alone or in conjunction with IPPs, significantly reduced knee injuries in soccer players. The results showed that performing IPPs that include balance training exercises can reduce knee injury rates by 56% compared to teams that did not apply. Our findings can help policymakers implement balance training as a preventive measure for knee injuries for soccer players.
Author contributions
CONCEPTION: Wesam Saleh A. Al Attar.
PERFORMANCE OF WORK: Wesam Saleh A. Al Attar.
INTERPRETATION OR ANALYSIS OF DATA: Wesam Saleh A. Al Attar.
PREPARATION OF THE MANUSCRIPT: Wesam Saleh A. Al Attar, Hussain S. Ghulam, Saud Al Arifi, Saad Alhosaini, Sami Alharbi, Yasser Alraddadi, Ahmed I. Alomar and Ross H. Sanders.
REVISION FOR IMPORTANT INTELLECTUAL: Wesam Saleh A. Al Attar, Hussain S. Ghulam, Saud Al Arifi and Ross H. Sanders.
CONTENT: Wesam Saleh A. Al Attar, Hussain S. Ghulam, Saud Al Arifi, Saad Alhosaini, Sami Alharbi, Yasser Alraddadi, Ahmed I. Alomar and Ross H. Sanders.
SUPERVISION: Ross H. Sanders.
Ethical considerations
This study, as a systematic review and meta-analysis, is exempt from Institutional Review Board approval.
Funding
The authors extend their appreciation to the Deanship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project number: IFP22UQU4350385DSR011.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project number IFP22UQU4350385DSR011.
Conflict of interest
The authors have no conflicts of interest to report.