
Abstract
BACKGROUND:
Intrinsic foot muscle (IFM) dysfunction and poor foot arch are associated with various foot conditions. Toe flexor exercise (TFE) has been used to improve it; however, the immediate effects of TFE on each IFM and how it relates to changes in navicular bone height (NH) are unclear.
OBJECTIVE:
This study aimed to investigate acute muscle swelling in the IFM after TFE and the association between changes in NH and IFM size.
METHODS:
Fourteen adults participated in this study. NH and cross-sectional area (CSA) of the IFM were acquired pre and post- TFE. The CSA of the IFM, including the abductor hallucis (AbH), flexor hallucis brevis, flexor digitorum brevis, and quadratus plantae, was acquired with ultrasonography. In the TFE, each participant completed five sets of eight repetitions with maximum strength.
RESULTS:
The NH and CSA of all IFM significantly increased significantly post-TFE (
CONCLUSION:
This study suggests that the acute swelling of AbH after TFE is associated with an immediate increase in NH, supporting the important role of AbH in the formation of foot arch.
Keywords
Introduction
The medial longitudinal arch (MLA) is an essential component involved in shock absorption and attenuation of force transmission from ground reaction forces during standing and walking [1, 2]. As the MLA is a variable structure [3], it is commonly known that changes in MLA height can lead to changes in plantar pressure distribution [4] and affect muscle activity [5, 6] and postural stability [7]. The MLA is formed and maintained by the bony structures, ligaments, and muscles. Intrinsic foot muscles (IFM) become more active with loading and contribute to stabilizing the MLA [8]. Moreover, IFM dysfunction relates to the decrease in the MLA. The lower MLA, that is, pes planus, is associated with foot deformities or injuries, including hallux valgus, excessive subtalar pronation, plantar fasciitis, and Achilles tendinosis [1, 9, 10, 11]. For this reason, maintaining or improving the function of the IFM is required and toe flexor exercise (TFE) for IFM activation is widely used in clinical practice to improve foot conditions.
To assess the effect of training on muscles, morphological changes in the muscles have recently been the focus of attention. Some studies based on ultrasonography or MRI have shown an increase in muscle cross-sectional area (CSA) immediately after resistance training [12, 13]. The acute increase in muscle morphology is considered to be caused by muscle swelling and alterations of intra- and extracellular water balance due to increased vascular permeability [14, 15]. Resistance exercise leads to the accumulation of lactate and hydrogen ions through the degradation of muscle glycogen [16]. After exercise, lactate and hydrogen ion concentrations are high [17], facilitating water uptake into muscle cells based on permeability [18, 19]. Increased pressure on the cell membrane is linked to the activation of anabolic protein kinase transduction pathways, which facilitates muscle hypertrophy [20, 21, 22]. Thus, acute effects on muscle morphology are considered to be important factors leading to muscle hypertrophy [23, 24]. In addition, it provides evidence of muscle activation during exercise. However, to our knowledge, no studies have investigated muscle swelling in the IFM after TFE. As the IFM is anatomically complex with four layers of small muscle located on the plantar, evaluating acute swelling of the muscle by reflecting muscle activation, is a useful method for assessing the effects of exercise on the muscle.
There are various methods of assessing MLA height; the simplest and most commonly used method is to directly palpate and mark the navicular bone and measure the navicular bone height (NH) above the ground [25]. Several studies have shown that TFE can increase NH [26, 27]. Most IFM are involved in toe flexion. Among them, the abductor hallucis (AbH) is known to be the key muscle for maintaining and elevating the MLA [26]. In a previous study, TFE with high AbH activity showed a higher MLA [26], and an attempt was made to elevate MLA by electrical stimulation of AbH [27]. Although the activity of AbH by TFE causes an increase in NH, that is, MLA, it is natural that IFM other than AbH are also trained by TFE, since toe flexion is a movement accomplished by multiple IFM. However, it has been difficult to examine the relationship between the MLA and the exercise effect on each muscle individually because muscles other than the AbH are at the plantar foot or overlapped by some muscles. Hence, by evaluating acute muscle swelling for each IFM and examining the relationship with the MLA, it may be possible to ascertain whether the muscles that increase in size with exercise are related to the increase in NH. The acute muscle swelling of IFM may suggest immediate changes and a relationship with NH. However, this immediate response may link it to changes associated with long-term intervention [23, 24].
The purpose of this study was to assess IFM muscle swelling immediately by ultrasonography after TFE and to investigate the relationship between the increase in CSA of the IFM and NH. We hypothesized that acute muscle swelling can be confirmed on all IFM acting in toe flexion and that the increase in AbH is related to the change in the amount of NH because of its role in forming and maintaining the MLA.
Methods
Participants
This study was conducted in the laboratory from April 1, 2022 to May 28, 2022, following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Fourteen adults (28 feet), including six males, participated in the study (Table 1). None of the participants had acute foot or ankle injuries within 1 year and a history of foot and ankle surgery. The inclusion criteria for this study were as follows: (i) without any pain on their foot and ankle, (ii) score 6 or less with foot posture Index (FPI). A normal foot was scored 0–6 and a pronated foot was scored 7 or more on the FPI [28]. The study protocols conform to the principles of the Declaration of Helsinki and were approved by the Ethical Committee for Epidemiology of Hiroshima University (approval number: E-2266). All participants provided their written informed consent to participate in the study.
Participants’ baseline characteristics
Participants’ baseline characteristics
Data are presented as the mean and standard deviation. BMI, body mass index; FPI, foot posture index.
Schematic for the present study. NH, navicular bone height; CSA, cross-sectional area; IFM, intrinsic foot muscles; TFE, toe flexor exercise.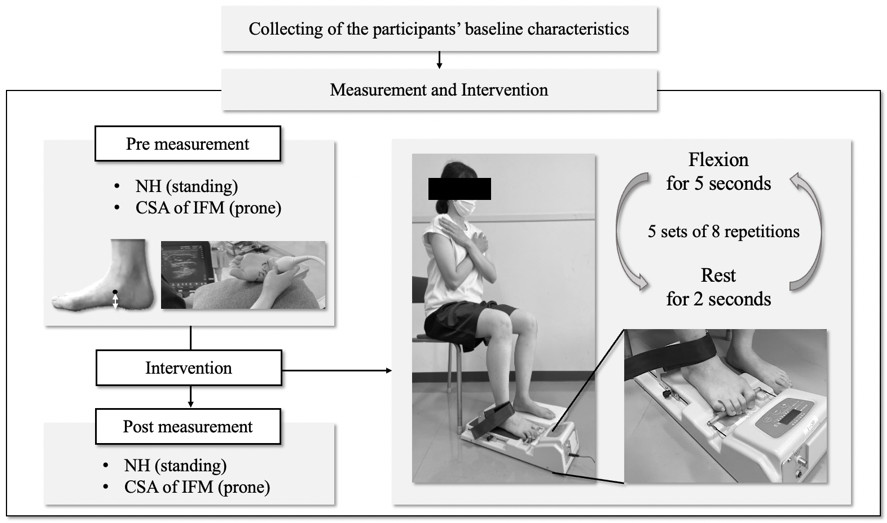
The participants’ sociodemographic data were measured the day before the TEF intervention, including the FPI and maximum toe flexor strength. The experimental protocol is illustrated in Fig. 1. In the present study, NH in a standing position with 50% weight bearing and morphology of IFM were acquired in two conditions: pre- and post-TFE. NH was measured from the ground to the anterior-inferior portion of the navicular using a ruler [25]. An image of IFM morphology was obtained using ultrasonography.
The TFE task using a toe grip dynamometer (T.K.K. 3361, Takei Scientific Instruments Co., Niigata, Japan) was conducted in a sitting posture with the hip and knee joints secured at 90
The CSA of four IFM including AbH, flexor hallucis brevis (FHB), flexor digitorum brevis (FDB), and quadratus plantae (QP) were evaluated using ultrasonography (SONIMAGE MX1, Konica Minolta, Inc., Tokyo, Japan). Participants were placed in the prone position with the knee flexed at 90
Details of the probe position and orientation were in accordance with previous studies that also reported the reliability of the protocol [31, 32, 33]. The CSA of the FDB and QP were acquired by placing the probe at 50% of the length in line with the medial tubercle of the calcaneus to the third metatarsal head. To obtain the CSA of the AbH, the probe was placed along a line perpendicular to the long axis of the foot, at the anterior aspect of the medial malleolus. The CSA of the FHB was measured perpendicular to the shaft of the first metatarsal, at the thickest portion of the muscle. Gain was adjusted for each foot to ensure that the fascial muscle borders were identifiable. Once the probe was placed, fine adjustments were necessary to visualize each muscle properly and accommodate anatomical variations. In addition, testers marked with a pen to place the probe so that measurements could be taken at the same location before and after TFE. While three testers participated in the measurement, all procedures for each participant were conducted by one tester. CSA was measured using ImageJ software (National Institutes of Health, Bethesda, Maryland, USA), and the region of interest was calculated along the muscle fascial borders. Three images of each muscle were obtained for each participant and were used to calculate the mean value of each CSA Intra-class correlation coefficients (ICC) were calculated to assess the repeatability of the measurements CSA of each IFM.
Statistical analysis
Comparison of the navicular bone height and cross-sectional area of intrinsic foot muscles between pre and post TFE
Comparison of the navicular bone height and cross-sectional area of intrinsic foot muscles between pre and post TFE
Data are presented as the mean and standard deviation. NH, navicular bone height; CSA, cross-sectional area; IFM, intrinsic foot muscles; FDB, flexor digitorum brevis; QP, quadratus plantae; AbH, abductor hallucis; FHB, flexor hallucis brevis.
Correlation coefficients between the change in NH and CSA of each IFM. NH; navicular bone height, CSA; cross-sectional area, IFM; intrinsic foot muscles, FDB; flexor digitorum brevis, QP; quadratus plantae, AbH; abductor hallucis, FHB; flexor hallucis brevis. 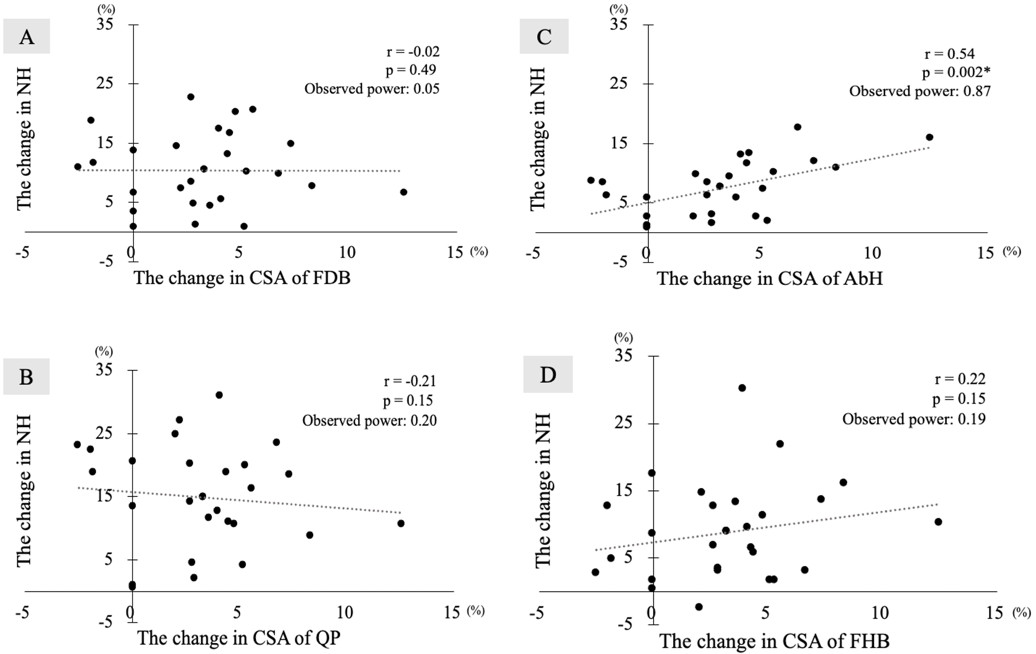
Statistical analyses were performed with the IBM SPSS Statistics software version 28.0 (IBM Japan Co Ltd, Tokyo, Japan). Prior to the analysis, the normal distribution of the data was confirmed using the Shapiro-Wilk test. All variables had normal distributions and are represented as means and standard deviations. The NH and CSA of each muscle were compared pre- and post-task using a paired
The ICC (1, 3) values for the FDB, QP, AbH and FHB showed excellent reliability (ICC
Table 2 shows the results of the NH and CSA of the IFM pre- and post-TFE. When comparing NH pre- and post-TFE, there was a significant increase in post-TFE (
Figure 2 shows the correlation coefficients between changes in the NH and CSA of each IFM. Only the amount of change in the CSA of the AbH was moderately positively correlated with the amount of change in the NH (
Discussion
The present study assessed muscle swelling in the IFM immediately after TFE and investigated the relationship between the increase in the NH and CSA of the IFM. To the best of our knowledge, this is the first study to show an increase in the CSA of the IFM as an acute muscle swelling after TFE using ultrasonography. The positive correlation between the increase in AbH and the amount of change in NH indicates the important role of AbH in the formation of the foot arch. Thus, this immediate association could suggest that AbH is a key muscle for increasing NH and we can expect that exercising AbH is important for improving NH. The findings from this study are a crucial and relevant clue for clinicians involved in the treatment and improvement of foot conditions or dysfunction of the IFM that are related to the prevention of injuries.
In this study, the CSA of all IFM increased immediately after TFE. This morphological change in muscles is termed swelling and has been recognized as a response to metabolic stress by resistance training [35, 36]. This acute morphological change in muscles itself does not indicate muscle development, but only an immediate effect of exercise, however, this acute muscle swelling is known to have a positive correlation with the long-term effect of muscle hypertrophy [30]. Toe flexion is a movement attributable to several IFM. The activation in the IFM, which is attached to each toe and has parallel anatomical orientations to the longitudinal arches, has been reported in previous studies using surface electromyography (sEMG) [26, 37, 38, 39, 40]. However, the small sizes and proximity of these muscles made it difficult to evaluate the effects on each muscle individually. Although a method to record sEMG for AbH has been established [26, 27], the deeply located IFM cannot be recorded with sEMG. In the present study, muscle swelling was evaluated using ultrasonography.
We identified a noticeable relationship between the change in the NH and CSA of the AbH by TFE. Previous studies have shown that AbH is important in supporting the MLA and controlling foot pronation during static stance [38, 40]. In support of this, the present study showed that muscle swelling in AbH after TFE was related to NH, which is located on the medial side of the foot and is used to evaluate MLA. This could be a result of the anatomical characteristics of the AbH which has parallel orientations with the MLA. AbH is the largest IFM and most medial muscle among the first layers of the IFM, which is the primary muscle involved in hallux abduction and acts during flexion of the first metatarsophalangeal joint [41]. The anatomical course of AbH arises from the posteromedial calcaneus and inserts into the sesamoid and inferior medial side of the proximal phalanx of the hallux [42]. Additionally, the AbH tendon has a conjoined tendon with FHB [42, 43]. These anatomical connections of AbH can explain why AbH acts in TFE. The results obtained from this study suggest that exercising AbH is crucial for NH elevation. Toe flexion is achieved by several IFM; however clinicians have to pay attention to whether there is a reliance on IFM other than AbH if their rehabilitation or exercise is for improving the foot arch. For example, it may be important to maintain the abduction position of the hallux during exercise. This means that the focus should be on AbH contraction.
This study has several limitations. Participants in this study had healthy feet. Foot deformities such as pes planus and hallux valgus may be caused by dysfunction of the IFM, and conversely, deformities may further impair IFM function. TFE is used to improve such foot conditions, and we will investigate whether the same results can be obtained with training for deformed feet as for healthy feet. In addition, the duration of the TFE effect, that is, muscle swelling or NH elevation is unclear. Based on the immediate relationship between AbH and NH changes obtained in this study, future work should proceed to examine the effects of long-term interventions. We believe that investigating how long the effect lasts and how muscle swelling and foot posture change differ with various types of exercise, including towel gathers and short foot exercises, will provide important clues that can be applied to clinical practice.
Conclusions
Acute muscle swelling on the IFM immediately after TFE can be assessed briefly using ultrasonography. Furthermore, the increase in AbH is related to a change in NH. This study showed that exercising AbH is of key importance in elevating NH and maintaining the MLA.
Author contributions
CONCEPTION: Honoka Ishihara, Hinata Esaki, Koki Tsuchida and Makoto Komiya.
PERFORMANCE OF WORK: Honoka Ishihara, Hinata Esaki, Koki Tsuchida and Ayano Ishida.
INTERPRETATION OR ANALYSIS OF DATA: Honoka Ishihara, Hinata Esaki, Koki Tsuchida, Ayano Ishida and Makoto Komiya.
PREPARATION OF THE MANUSCRIPT: Honoka Ishihara.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Shogo Tsutsumi, Tsubasa Tashiro, Makoto Komiya and Noriaki Maeda.
SUPERVISION: Yukio Urabe.
Ethical considerations
The study protocol met the requirements of the Declaration of Helsinki and was approved by the Ethical Committee for Epidemiology of Hiroshima University (approval number: E-2266). All participants provided their written informed consent to participate in the study.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.