
Abstract
BACKGROUND:
The return to activities and sports after the anterior cruciate ligament (ACL) reconstruction is a critical decision.
OBJECTIVE:
To verify the most used elements during the isokinetic evaluation for discharge after ACL reconstruction.
METHODS:
Systematic review (PROSPERO CRD42021224433). Research in the literature: PubMed, Medline, SciELO, Lilacs, CENTRAL, PEDro, Web of Science and Embase, in February 2022. Studies that performed isokinetic evaluation during the discharge period in male patients aged 18 to 59 years after ACL reconstruction. Descriptive synthesis on the most used parameters during isokinetic evaluation as a discharge criteria after ACL reconstruction.
RESULT:
Twenty-three studies involving 1,792 participants were included. Medium and high quality evidence identified that most isokinetic evaluations targeted only muscle strength after rehabilitation of the ACL (peak moment).
CONCLUSION:
The most used elements during the isokinetic evaluation were: angular velocity of 60∘/s, 1 set of 5 repetitions, concentric mode and peak moment.
Introduction
The knee joint is constantly subject to injury, since its stability depends on the complex anatomy of muscles and ligaments [1, 2, 3]. The anterior cruciate ligament is responsible for preventing anterior sliding of the tibia in relation to the femur, knee hyperextension and rotational movements [4, 5, 6]. After anterior cruciate ligament injury, surgical reconstruction is often recommended to restore anterior knee stability [7, 8]. The return to activities and sports after the anterior cruciate ligament reconstruction is a critical decision, because the criteria used for discharge are fundamental to prevent injury recurrences, to ensure patient’s best performance, and even to reduce the costs with health treatments [9].
The isokinetic dynamometer is considered the gold standard method for strength evaluation, being fundamental to measure muscle rebalance and joint function [4, 10]. The device imposes resistance with constant velocity that adapts to the patient’s strength, measuring parameters such as moment (Newton meter), angular velocity, total muscle work (Joules) and muscle power (Watts), providing numerical results and graphs [11]. The isokinetic dynamometer performs a quantitative evaluation of muscle function, its measurements are safe, objective and reproducible, besides being able to identify the patient’s deficiencies, establishing a criterion for discharge and return to sport [12].
Undheim et al. [13]. conducted a systematic review to report isokinetic evaluation protocols to assess muscle strength of patients undergoing anterior cruciate ligament reconstruction [13]. However, the study was conducted with low methodological quality, because the data were extracted only by the main author, causing a high risk of bias to the results. Moreover, the non-characterization of the sample studied regarding sex may interfere with the results due to the variation of strength between sexes [14]. The literature searches were carried out in 2013. Currently, new studies have been published, which may change the results presented.
Roe et al. [15] investigated the criteria for returning to sport and muscle strength was present in 50 studies. Of these studies, 33.3% evaluated isokinetic strength at 60∘/s. However, the study was developed to examine similarities and differences in tests for return to sport, i.e., the isokinetic criteria and parameters used were not specifically investigated, which are fundamental to measure muscle stability so that patients return to daily and sports activities more safely and with lower risk of injury recurrences. Thus, a systematic review investigating isokinetic parameters is necessary, to verify in detail which isokinetic parameters are being used for discharge and return to sport. Therefore, the aim of this study was to verify which are the most used parameters in the isokinetic evaluation for discharge after anterior cruciate ligament reconstruction.
Methods
This systematic review is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [16] guidelines. The review protocol was prospectively recorded in the PROSPERO database (CRD42021224433).
Search strategy
Systematic searches were performed in the electronic databases: PubMed (MEDLINE), SciELO, LILACS, CENTRAL (Cochrane Central Register of Controlled Trials), PEDro, Web of Science and EMBASE, from the oldest records until February 24, 2022, without restrictions regarding language and year of publication.
For the search strategy, terms and words related to the subject were used, in addition to the descriptors present in the DeCS (Descriptors in Health Sciences) and meSH (Medical Subject Headings) PubMed: “Anterior cruciate ligament” AND “isokinetic dynamometer”. The detailed search strategies used in each database are described in Appendix 1.
Inclusion and exclusion criteria
The studies were considered for inclusion if they met the following criteria: (1) any study design except: reviews of any nature, experience report, in vivo studies, in vitro studies, animal studies and case reports, (2) male participants aged between 18 and 59 years, (3) and perform isokinetic evaluation during discharge in patients submitted to or after anterior cruciate ligament reconstruction. Studies (1) unavailable full text and if there was no response from the authors were excluded (2) there was no specification in the sample sex (3) no full text was found and there was no response from the authors.
Studies selection
The studies selection process included: (1) analysis and selection by screening of titles, (2) analysis and selection by reading abstracts and (3) analysis and selection by reading the full texts, taking into account the inclusion criteria established. Potentially eligible studies were also researched by reading the reference lists. Three independent reviewers extracted the data (ACJC, LZRS and LGF) and, in case of disagreement, reviewers discussed to reach consensus.
Data extraction
Studies selection process and inclusion process.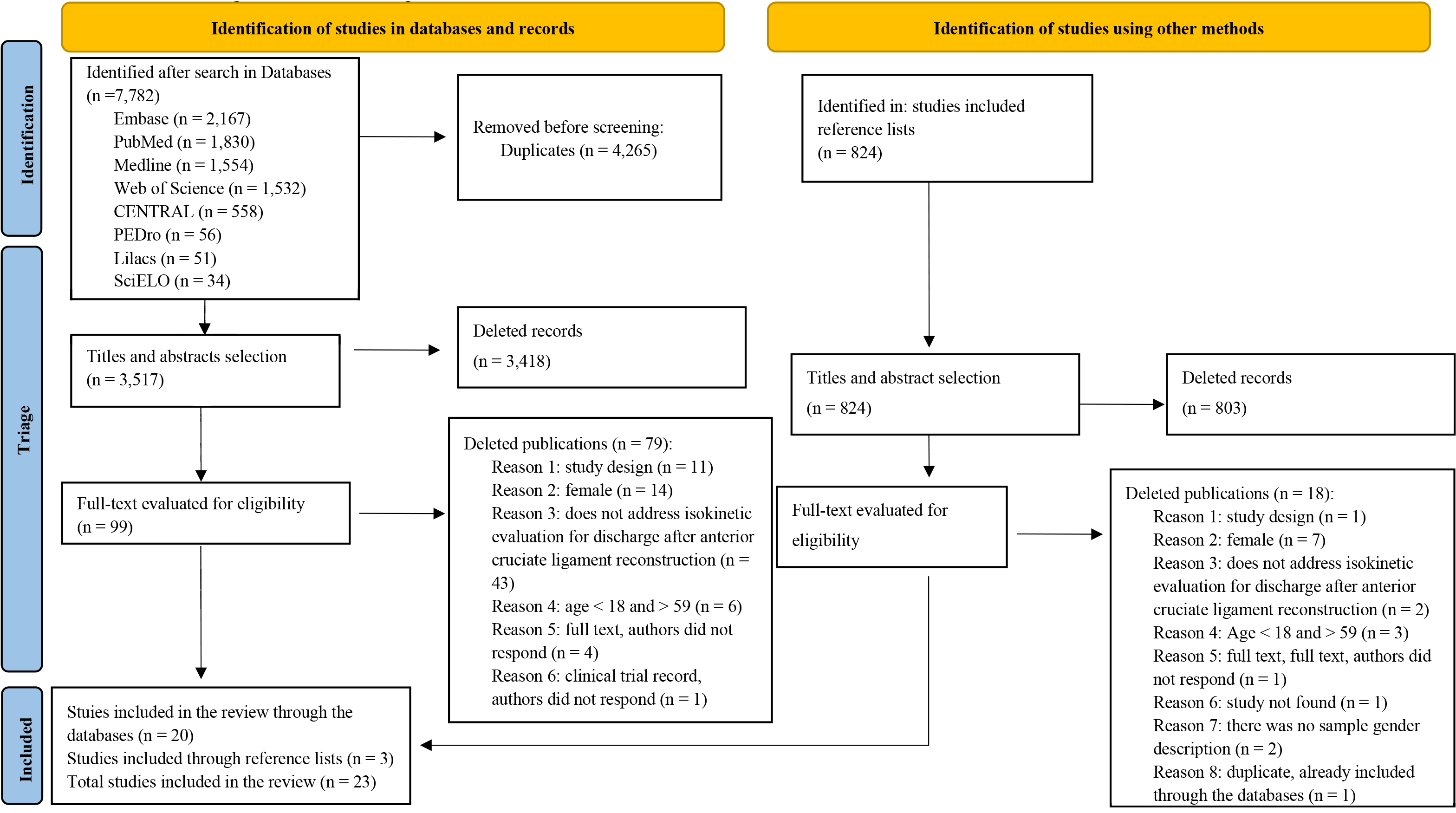
A study-based data extraction form [17] was elaborated to record information on: (1) year of publication, (2) study design, (3) characteristics of participants, and (4) isokinetic evaluation protocol. Three independent reviewers extracted the data (ACJC, LZRS and LGF) and, in case of divergence; reviewers discussed to reach consensus.
The quality assessment was performed through a personalized checklist [18]. adapted to the isokinetic instrument, because no standardized quality assessment guidelines applicable to the the purpose of this study were identified, in addition to the included studies design heterogeneity. The quality checklist consisted of 20 items, each item was evaluated with 0 (not described), 1 (limited description) and 2 (described appropriately), Appendix 2. Items 10 to 15 were adapted to the isokinetic dynamometer instrument, without prejudice to the total score. According to the scale score, the studies are classified as low quality (score
Due to some items adaptation in the personalized checklist, relative reliability was performed to observe the reliability among the study evaluators. Reliability was calculated by the Intraclass Correlation Coefficient (ICC), with a 95% confidence interval (95% CI), using the two-way mixed effects model, absolute agreement, a single evaluator model. The ICC is interpreted according to the following guidelines: values lower than 0.5 indicate low reliability, values between 0.5 and 0.75 indicate moderate reliability, values between 0.75 and 0.9 indicate good reliability, and values higher than 0.90 indicate excellent reliability as suggested by Koo and Lee [19].
Data analysis
The variables measured in the study were described through qualitative analysis and narrative synthesis of the findings.
Results
Studies inclusion
The databases search resulted in 7,782 studies, of which 3,418 were excluded after reading the titles and abstracts, and 3,517 were considered potentially eligible. In addition, a total of 79 studies were excluded after reading the full text and 5 studies were not found, although contact was made with the authors by e-mail, requesting the full text. An abstract was considered potentially eligible but was not included in the analysis because the full text could not be assessed [20].
Twenty studies were included through the databases and three studies were included through the reference lists of the included studies. Thus, 23 studies met the inclusion criteria and were included in the review [21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43]. Furthermore, f [21,22,23,24, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] our additional potentially eligible studies were found [44, 45, 46, 47] in the selected studies reference lists, but were not included, since the full text was not found [44] even after being requested; the study was not found [47] there was no specification of the sample gender [45, 46]. and the authors’ contact was not available. The entire eligibility assessment process is described in Fig. 1.
Studies characteristics
Twenty-three studies were included in the analysis (
Description of the studies included in the analysis
Description of the studies included in the analysis
N – Total sample number; ∘/s – Degrees per second; (Nm) – Newton / meters ; Nm/kg – Newton meter/kg; H/Q ratio – hamstring/quadriceps ratio; MI – Member involved; MNI – Member not involved; IL – Injured limb; UL – Uninjured limb; ILS – Index of limb symmetry; PM- Peak moment; PO – Power; TW – Total work; ROM – Range of motion; km/h – Kilometer/ hour; Kg – Kg; kg/m2 – Kilogram / square meter; cm – Centimeters; m – Meters; ACL – Anterior cruciate ligament; ACLR – Anterior cruciate ligament reconstruction; Hz – Hertz; BMI – Body mass index; PBTB – patellar bone-tendon-bone graft; STG – semitendinosus and gracilis tendon graft.
Table 1 presents the characteristics of the studies.
Nineteen studies performed warm-up [21, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 35, 36, 37, 38, 39, 40, 42, 43] and fourteen performed familiarization with the device [21, 22, 25, 26, 27, 28, 29, 30, 31, 32, 35, 38, 42, 43]. before evaluation. The warm-up was performed using an exercise bike or cycle ergometer for 5 to 12 minutes [21, 24, 26, 27, 28, 29, 31, 32, 33, 35, 36, 40, 42, 43]. Lustosa, Fonseca e Andrade (2007) [35]. Thiele et al. [42]. Kadija et al. [32] and Milutinovic et al. [36] in addition to cycling, used stretching for the evaluated muscles. Cardone et al. [24]. O’ Malley et al. [39] and Milutinovic et al. [36] used repetitions using the device as warm-up. O’ Connor et al. [38]. performed running, squats and jumps. Other studies performed warm-up for 5 minutes, without specifying the way of execution [23, 25, 37] and 4 studies did not perform warm-up [22, 30, 34, 41].
Familiarization consisted of repetitions with submaximal force, between 2 and 5 repetitions [28, 29, 31, 32, 43]. Dagnoni et al. [28] and Dauty et al. [29] in addition to the repetitions with submaximal force, performed repetitions with maximum force. Abellaneda et al. [21] and Lustosa et al. [35]. performed repetitions at each velocity evaluated as a form of familiarization. In the study by Cvjetkovic et al. [26] all participants had at least 2 previous tests using the Biodex System. Other studies performed some repetitions using the device [22, 25, 27, 30, 38, 42] and 9 studies did not perform familiarization [23, 24, 33, 34, 36, 37, 39, 40, 41].
Contraction mode
During the isokinetic evaluation 16 studies used concentric mode [21, 22, 24, 25, 26, 28, 30, 31, 34, 35, 37, 39, 40, 41, 42, 43]. 4 studies used concentric and eccentric mode [21, 30, 31, 42]. 2 studies used the isometric mode [30, 32] and the remaining did not specify the contraction mode used [23, 27, 29, 33, 36, 38].
Angular velocities
The most used angular velocities were 60∘/s, evaluated in 21 studies [21, 22, 23, 24, 26, 27, 28, 29, 30, 31, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42]. and 180∘/s, evaluated in 13 studies [22, 23, 24, 26, 27, 29, 31, 33, 34, 36, 37, 42, 43]. Other angular velocities such as 30∘/s [21]. 120∘/s [40, 42, 43]. 240∘/s [21, 24] and 300∘/s [34, 35, 40, 43]were also observed [21, 24, 34, 35, 40, 42, 43].
Isokinetic variables
In this review, 20 studies used peak moment to measure muscle strength [21, 22, 23, 24, 25, 26, 27, 29, 30, 31, 33, 34, 36, 37, 38, 39, 40, 41, 42, 43] 5 studies investigated power [26, 34, 38, 39, 42] and 6 studies investigated the total work [24, 27, 28, 34, 35, 42]. The H/Q ratio (Hamstring/quadriceps) was analyzed by 10 studies [22, 26, 27, 28, 31, 32, 33, 34, 36, 41] and limb symmetry index was calculated by 9 studies [25, 30, 32, 33, 36, 38, 39, 41, 43].
Sets and repetitions
Regarding the set and repetitions during the isokinetic evaluation, 10 studies performed 1 set of 5 repetitions [22, 23, 25, 26, 30, 33, 34, 35, 42, 43]. Baltaci et al. [23]. Cvjetkovic et al. [26]. Czaplicki et al. [27]. Kyritsis et al. [34]. Akinci et al. [22]. Krzemińska et al. [33] used 1 set of 5 repetitions at 60∘/s and 1 set of 10 repetitions at 180∘/s, with the exception of Kyritsis et al. [34] who followed these repetitions and added 1 set of 20 repetitions at 300∘/s and Krzemińska et al. [33] which used 1 set of 8 repetitions at 180∘/s. Milutinovic et al. [36] performed 5 knee flexion repetitions and 5 knee extension repetitions.
Dauty et al. [29] and Jamshidi et al. [31] performed 3 repetitions at 60∘/s and 5 repetitions at 180∘/s. Dagnoni et al. [28] and Abellaneda et al. [21] evaluated with 1 set of 3 repetitions. O’ Malley et al. [39] and Seo et al. [41] used 2 sets of 5 repetitions. Cardone et al. [24] performed 1 set of 4 repetitions and O’Connor et al. [38] 3 sets of 5 repetitions. Kadija et al. [32] evaluated isometrically and used 2 maximum isometric contractions sustained for 6 seconds. Other studies did not specify the repetitions performed [37, 40].
Included protocols quality assessment
The quality assessment of the included studies consisted of 14 high-quality studies and 9 medium-quality studies. Thus, 61% of the studies included in this review are of high quality and 39% are classified as medium quality.
Quality assessment scale adapted to the isokinetic evaluation
Quality assessment scale adapted to the isokinetic evaluation
As 1: Assessor 1; As 2: Assessor 2; T: total score; T%: Total score in percentage; AT%: Average total score in percentage.
The reliability values for the evaluation instrument adapted by the authors were calculated by means of each question of the form as follow: assessor 1 with assessor 2
Additional information about included studies
ACL: anterior cruciate ligament; IKDC: International Knee Documentation Committee; ACL-RSI: Anterior Cruciate Ligament-Return to Sport After Injury Scale; SLDJ: Single leg drop jump; SLCMJ: Single leg countermovement jump; ACL-QoL: Anterior Cruciate Ligament Quality of Life Questionnaire; BPTB: bone- patellar tendon-bone; HS: gracilis/semitendinous double bundle; KOOS: Knee and Osteoarthritis Outcome Score; QT: quadriceps; P-ACLR: Primary anterior cruciate ligament reconstruction; R-ACLR: Revision of anterior cruciate ligament reconstruction.
Additional information about the included studies, such as the type of surgical procedure, postoperative time, whether there was fatigue during the isokinetic evaluation, use of functional tests and recurrence of injuries, are shown in Table 3.
Discussion
The aim of this study was to verify the most used parameters during isokinetic evaluation for discharge after anterior cruciate ligament reconstruction. According to Fonseca et al. [48] isokinetic parameters have been used in research and clinical practice, providing accurate data on muscle performance and information on joint rebalance. The main results of this study indicate that the most used parameters correspond to the angular velocity of 60∘/s, 1 set of 5 repetitions, concentric mode and variable peak moment. In addition, most studies performed warm-up and familiarization with the device before the evaluation.
Main findings interpretation
According to Dvir [49] isokinetic dynamometry is considered the gold standard due to the reliability in quantifying the variables related to muscle performance generated by muscle contraction. The most used contraction mode in the studies [21, 22, 24, 25, 26, 28, 30, 31, 34, 35, 37, 39, 40, 41, 42, 43]was the concentric mode. This choice can be justified by the fact of easy-to-understand execution, making muscle contraction more effective for evaluation. On the other hand, the eccentric mode is more complex, requiring greater motor control compared to the concentric mode and consequently more familiarization with the device. Thus, it can decrease the reliability and reproducibility of isokinetic evaluation [23].
The peak moment, measured in 21 studies [21, 22, 23, 24, 25, 26, 27, 29, 30, 31, 33, 34, 36, 37, 38, 39, 40, 41, 42, 43]is the maximum force produced during the range of motion and the lower the dynamometer velocity, the higher the peak moment [12, 50, 51]. Thus, it is understood that it is preferable that the peak moment be evaluated at slow angular velocities, such as 60∘/s, to potentiate muscle strength ability, which is in accordance with the results of the study in which the angular velocity of 60∘/s was the most used. Roe et al. [15] evaluated muscle strength as a criterion for returning to sport in 82.5% of the studies, the isokinetic strength at 60∘/s is the most used angular velocity, which corresponds to 33.3% of the included studies. Quadriceps weakness correlates with greater movement asymmetries, being predictive of failure in the criteria for returning to sport [15].
In the review by Burgi et al. [52] from the 209 studies included, 41% included strength as a criterion for returning to sport and 40% of the 50 studies that used isokinetic force as part of the return to sport criteria required a limb symmetry index with at least 85% [52]. This corroborates this study results, because the limb symmetry index was analyzed in 39% of the included studies. Bilateral deficit, i.e., strength deficit greater than 10%, may be a risk factor in knee injuries [15, 53, 54]. The isokinetic evaluation indicates muscle asymmetry and these values are fundamental due to the maintenance of symmetry between limbs [48] because the asymmetric strength of the quadriceps is directly proportional to the risk of new rupture of the anterior cruciate ligament [55, 56]. Thus, the bilateral deficit is an important variable to be considered as one of the discharge and return to sport criteria.
Although peak moment is the most commonly measured variable, H/Q ratio is a fundamental element to observe muscle movement efficiency and joint stability after anterior cruciate ligament reconstruction [57]. The H/Q ratio is calculated by the hamstring peak moment divided by the quadriceps peak moment [12, 51, 58]. This ratio is important as it will show the muscle imbalance resulting from the injury. At slow velocities, the H/Q ratio is around 60% for healthy individuals, values below 50% indicate severe muscle imbalance and may predispose to new injuries [58]. According to Dingenen and Gokeler [56] for every 10% reduction in the H/Q there is a greater risk of 10.6 times of a new rupture of the anterior cruciate ligament [56]. Thus, the H/Q ratio is a necessary and objective parameter for discharge and return to sport, establishing a more assertive decision in order to prevent injury recurrences.
Regarding the set and repetitions used during isokinetic evaluations, 10 studies performed 1 set of 5 repetitions [22, 23, 25, 26, 30, 33, 34, 35, 42, 43]. Baltaci et al. [23]. Cvjetkovic et al. [26] and Czaplicki et al. [27] used 1 set of 5 repetitions at 60∘/s and 1 set of 10 repetitions at 180∘/s. For the velocity of 60∘/s, a few repetitions were performed, while for 180∘/s a higher volume of repetitions was performed. It is recommended to perform fewer repetitions for peak moment evaluation at lower angular velocities, because peak moment presents an inverse relationship to the angular velocity applied to the test, in other words, the lower the velocity in the dynamometer, the higher the peak moment [12]. However, for power, a higher volume of repetitions is performed at higher velocities, because the power is higher in the velocity of movement in the shortest fraction of time [59]. Thus, it is essential to perform the evaluation at both velocities, because muscle strength (peak moment) and muscle velocity or explosion (power) are important components of muscle function, since power is widely used in sports gestures [60] and its evaluation for discharge and return to sport is fundamental.
Limitations
The major limitation of this study is that the criterion for selecting the final recommendations to perform knee isokinetic assessment after ACL reconstruction and rehabilitation to return to physical activities is based only on the frequency of findings. There are no evaluation quality criteria, nor comparison with other parameters such as functional tests, new ACL injury or fatigue during the test. Future studies with the purpose of comparing other parameters with isokinetic evaluation are suggested. It would also be informative and beneficial if there were descriptions of isokinetic assessment protocol modifications according to time since surgery.
There was difficulty in including all eligible studies, although the authors were contacted [44, 45, 46, 47]. In addition, it was not possible to perform a meta-analysis of the studies included in the review, due to the descriptive characteristic of the parameters used during the isokinetic evaluation at discharge after anterior cruciate ligament reconstruction. Another possible limitation, regarding the sample analyzed, the level of physical activity was not stratified, which may differ the isokinetic evaluation among active, sedentary or athletes. In addition, only male participants were included. Thus, the results of this study cannot be extrapolated to the general population.
Another limitation of the study was that only Jamshidi et al. [31] cited the Dynamic Control Ratio (Hecc/Qcon), described for the first time by Dvir et al. [61]. This ratio, which reflects the hamstring capacity to eccentrically the restrain forward movements of the tibia due to strong quadriceps concentric contraction was significantly higher in the ACL-deficient knee than in the healthy knee. Further studies are needed to investigate the relationship to high-level sports performance and return to sports after anterior cruciate ligament reconstruction.
Clinical implications
This systematic review presents the main conducts and evaluations for discharge and return to sport through the isokinetic dynamometer, what has been used and which variables are prioritized. The parameters identification during isokinetic evaluation will help to support clinical practice and scientific research, improving clinical accuracy on the method used for patients evaluation for physical therapy discharge.
The results show that the studies are focused on the evaluation of muscle strength as a criterion for discharge and return to sport. Other criteria should still be taken into account during evaluation, such as the evaluation of power, total work, H/Q ratio and bilateral deficit analysis. Changes in isokinetic parameters are related to injuries and to deficits evaluated [4]. There is little evidence in the literature on the muscular deficiency index (MDI) [62] which could be useful to establish functional progression and discharge criteria, through minimum values of symmetry between the limbs. Thus, primary studies are necessary to investigate its repercussions. In addition, other criteria such as the complementary use of other tests, for instance functional tests, are essential to complement the decision on discharge and return to sport, to investigate functionality in conjunction with muscle strength.
Future studies are needed to verify which are the most used isokinetic parameters during discharge for more specific population such as women, since the population may present differences, especially during muscle strength evaluation. Furthermore, to investigate in the literature whether there are differences in the isokinetic parameters used during the evaluation of patients after anterior cruciate ligament reconstruction and healthy population. It is suggested that future primary studies describe in detail the protocols used, and may be based according to Appendix 2 used in this study. It is recommended that the H/Q ratio and limb symmetry index be approached more intensely in clinical practice, as they are fundamental to observe the efficiency of muscle rebalance after anterior cruciate ligament reconstruction for discharge and return to sport.
Conclusion
The results of the present study indicate that the most used parameters during the isokinetic evaluation for discharge after anterior cruciate ligament reconstruction were: angular velocity of 60∘/s, 1 set of 5 repetitions, concentric mode and variable peak moment. It is important to emphasize that the recommendations of this study are based only on the frequency of findings, and not on the frequency of new injuries or other qualitative criteria.
Author contributions
All authors contributed to the conception, design, analysis and results interpretation. All authors contributed to the manuscript writing and critical review.
Data sharing
All data relevant to the study are included in the manuscript or appendices.
Ethical considerations
There was no patient or public involvement in this study.
PROSPERO register
Isokinetic parameters used during discharge in patients after ACL reconstruction rehabilitation: a systematic review. ID: CRD42021224433.
Footnotes
Acknowledgments
To the Araucaria Foundation for Scientific and Technological Support and Development. Ana Carolina de Jacomo Claudio was a fellow of the Institutional Program of Scientific Initiation Scholarships (PIBIC), having financial support from the Araucaria Foundation for Scientific and Technological Support and Development.
Conflict of interest
The authors declare that there are no conflicts of interest.
Appendix 1. Search strategies description in each database
Appendix 2. Customized checklist adapted for the Isokinetic Dynamometer
Have the research objectives or goals been clearly stated? Has the study design been clearly described? Has the study population been adequately described? Have the eligibility criteria been specified? Has the sampling methodology been adequately described? Was the sample size used justified? Has the description of the method allowed precise replication of measurement procedures? Has the participants evaluator been described (e.g., experience)? Has a system been reported to standardize motion instructions? (yes) Has the isokinetic been calibrated? Was there a gravity correction? Was warm-up performed? Have the angular velocities analyzed been clearly described? Has familiarization been performed? Have the measured variables been clearly described? Has the system been compared to a recognized gold standard? (yes) Have reliability/accuracy measurements of the equipment used been reported? (yes) Have the main findings of the study been declared? Were the statistical tests appropriate? Have the limitations of the study been clearly described?
Each item was evaluated with 0 points when not described, 1 point when considered limited description and 2 points when adequately described.
The total score was calculated and the studies were classified as low quality (score