
Abstract
BACKGROUND:
Pelvic-drop exercise (PD) is unilateral weight-bearing exercise that is frequently performed in rehabilitation sessions because its easy application can trigger moderate-to-high gluteus medius (Gmed) activity. Hip rotation has been applied to effectively facilitate Gmed activity during exercise.
OBJECTIVE:
To determine the effects of PD with three different hip rotations on Gmed, tensor fasciae latae (TFL), gluteus maximus (Gmax) activity, and Gmed:TFL activity ratio in patients with Gmed weakness.
METHODS:
Eighteen subjects with Gmed weakness participated. Subjects performed three different forms of PD with neutral hip, hip internal rotation, and hip external rotation position. Surface electromyography was performed to quantify the activity of Gmed, TFL, and Gmax.
RESULTS:
PD with hip internal rotation showed significantly greater Gmed activity than with neutral hip and hip external rotation (
CONCLUSIONS:
PD with hip internal rotation is recommended to stimulate greater Gmed activity while preserving Gmed:TFL muscle activity ratio.
Keywords
Introduction
The gluteus medius muscle (Gmed) is a primary hip abductor muscle that attaches proximally to the external surface of the ilium and distally to the greater trochanter [1]. Through concentric, isometric, and eccentric contractions, the Gmed abducts the hip, stabilizes the pelvis, and controls hip adduction and internal rotation, respectively [2]. Gmed weakness is associated with impairment of functional activities such as balance, gait, and running as well as with pathologies of the hip, knee, and ankle joints, including femoroacetabular impingement, patellofemoral pain syndrome, iliotibial band syndrome, and chronic ankle instability [3]. Therefore, many previous studies investigated the effects of weight-bearing (WB) or non-WB exercises for strengthening the Gmed and previous review article reported that WB exercises generally showed a higher level of muscle activity than non-WB experience, except for side-lying hip abduction [4].
Unilateral WB exercises, which closely replicate functional activities of daily living, are prescribed by clinicians to stimulate functional muscle recruitment patterns [5, 6]. The hip abductor muscles must produce adequate internal torque to counter the external torque generated by the mass of the head, arms, and trunk during WB exercises for hip muscle strengthening [7]. Pelvic-drop exercise (PD), a unilateral WB exercise, is frequently performed in rehabilitation sessions because its easy application can trigger moderate-to-high Gmed activity [8, 9] and hip abductor activation is required to control pelvic orientation [7].
Hip rotation has been applied to effectively facilitate Gmed activity during exercise [8, 10, 11, 12, 13]. In particular, hip internal rotation during side-lying hip abduction and side-sling plank provoked significantly higher Gmed activity than a neutral or externally rotated hip position [10, 11, 13] because Gmed reached a favorable position with the internally rotated hip joint. However, the relative activity of the synergistic muscles should be considered when prescribing these exercises to patients with Gmed weakness [10]. Synergist muscles act together and affect each other during movement [14, 15]. Based on these findings, hip rotation during PD exercise can increase Gmed activity, which could reduce tensor fasciae latae (TFL) and superior portions of the gluteus maximus (Gmax) activity [1].
This study aimed to determine the effects of PD with three different hip rotations (neutral, internal, and external rotation) on Gmed, TFL, and Gmax activity and the Gmed:TFL activity ratio in patients with Gmed weakness. We hypothesized that internal or external hip rotation would change muscle activity during PD.
Methods
Participants
Sample size was calculated using the G Power software version 3.1 (Heinrich-Heine-Universität Düsseldorf, Germany). The necessary sample size of 6 patients was calculated from the data obtained from a pilot study of 6 patients to achieve a power of 0.80, an effect size of 0.69 (calculated with the partial
Inclusion criteria were Gmed weakness (grade 3 or less on manual muscle testing), absence of past or current lower extremity injuries such as sprains or fractures, and ability to maintain three PD exercise positions for 5-s [13, 16]. The weaker leg, defined as the leg with less hip abduction strength on a handheld dynamometer test (mobile MT-100, SAKAI Medical Co., Ltd.), was selected for investigation [16]. The exclusion criteria were previous musculoskeletal, neurological, and cardiopulmonary disease, involvement in lower limb sports during the past 3 months [7], and shortness of TFL (hip adduction
Instrumentation
Surface EMG (TeleMyo DTS; Noraxon Inc., Scottsdale, AZ, USA) was used to measure the activity of the Gmed, TFL, and Gmax in three different PD conditions. The Noraxon MyoResearch Master Edition software package ver. 3.16 (Noraxon Inc.) was used to analyze the EMG data. The EMG signals were sampled at 1500 Hz with the first order high-pass filters at 10 Hz
The range of motion of hip abduction or hip rotation was measured using a MyoMotion 3-dimensional (3D) motion analysis system (Noraxon Inc.) with a small inertial measurement unit sensor placed on a body segment. The 3D angular orientation was tracked. Two inertial measurement unit sensors were also placed in the anterior region of the thigh and the pelvis, between the posterior-superior iliac spines. The sampling rate was 200 Hz. The MyoResearch Master Edition software package ver. 3.16 was used to analyze the 3D motion data.
Procedures
First, the principal investigator (SMB) explained the overall experimental procedure to the selected patients, from whom informed consent was obtained for participation in the present study before the start of the experiment. Second, manual muscle testing was performed to confirm Gmed weakness. For the test, the patients were instructed to adopt a side-lying position on the treatment table with the bottom leg flexed for comfort and stability. The test leg was aligned to the rest of the trunk. The hip joint of the test leg was abducted to 50% of the total range of motion. The investigator provided hip abduction resistance by placing the hand 10 cm proximal to the lateral femoral epicondyle. An isometric hold for 5-s against resistance was then performed [18]. Because TFL recruitment or hip hiking provoked by the quadratus lumborum could interfere with the test, the patients were requested to avoid any medial rotation or flexion of the hip with verbal encouragement to facilitating maximal performance [19]. A three-minute rest was given between 2 trials of isometric hold. Muscle grading, described by Kendall [20], expressed as 0, 1, 2, 3, 4, 5 and 3 or less was considered weak. The reliability of the manual muscle test for the individual muscle groups was 0.63–0.93 [20]. Third, to determine the general characteristics of the participants, their heights and weights were measured before the experiment. Before participating in the investigation, patients jogged at a submaximal speed for 5 minutes to warm up and reduce discomfort or pain while performing the exercises [11]. Patients were familiarized with the exercises and were tested only after they had demonstrated exercise precision. To avoid the influence of fatigue and learning effects, the sequence of three different forms of PD was randomized using a random number generator in Excel software (Microsoft Corp., Redmond, WA, USA). Each PD condition was performed 3 times at a comfortable speed, with a 3-minute rest between them [16]. The exercise positions were maintained for 5-s with a 10-s rest between trials. The mean values for data analysis were calculated from the middle 3-s of each exercise to reduce any starting or ending effects on the skin-electrode connecting element.
Pelvic drop with neutral hip. For PD-N, the patients stood on the test leg on a 15-cm step with both knees in full extension. The contralateral pelvis was lowered toward the floor with the feet flat in the absence of trunk’s compensatory motion (Fig. 1). The pelvis was lowered on 3 beats with a metronome set at 60 beats per minute and raised on the next in a continuous manner. The test leg was positioned neutrally, and the non-test leg had no support [7, 8].
Pelvic-drop exercise with neutral hip.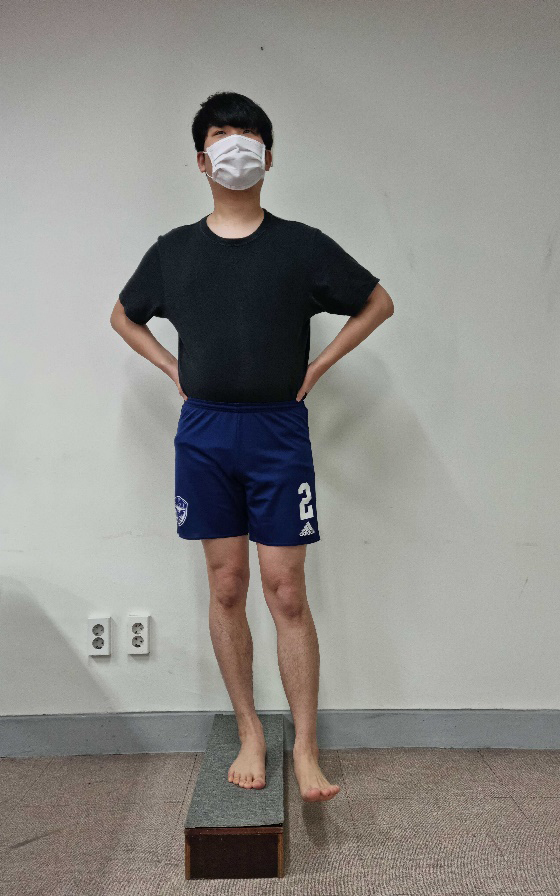
Pelvic-drop exercise with hip internal rotation.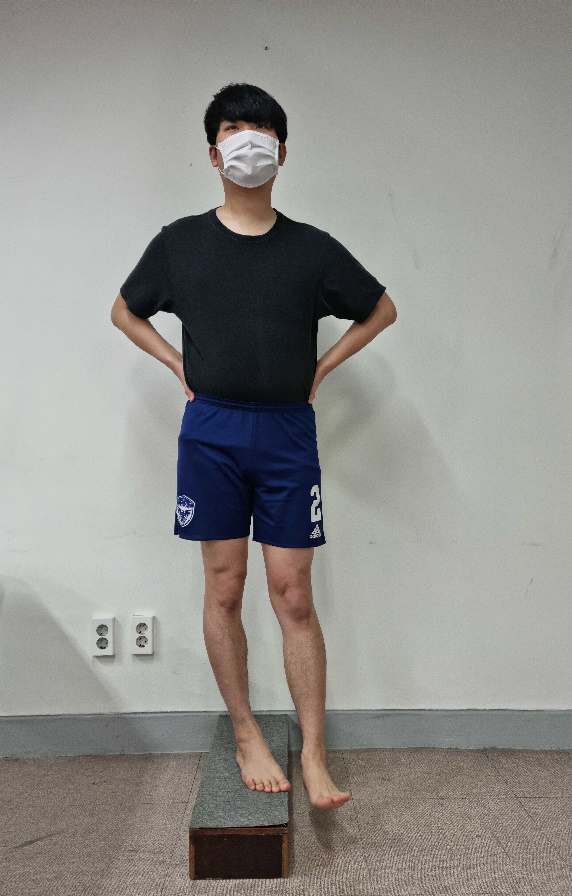
Pelvic-drop exercise with hip external rotation.
Pelvic drop with hip internal rotation and external rotation. PD-IR and PD-ER were performed in the same way as PD-N except for hip rotations of the test leg to about 50% of the maximal range of motion (Figs 2 and 3).
EMG data collection. Disposable Ag/AgCl surface electrodes were placed approximately 2 cm apart in the direction of the muscle fibers. The electrodes were placed over the midsection of the muscle bellies following the description by Criswell (2010) [21]. For Gmed, the electrodes were placed approximately one-third of the distance between the iliac crest and the greater trochanter. For TFL, electrodes were placed approximately 2 cm below the anterior superior iliac spine. For Gmax, electrodes were placed at half the distance between the second sacral spinous process and the greater trochanter.
Maximal voluntary isometric contraction (MVIC) in the standard manual muscle test position was used to normalize the EMG signals of Gmed, TFL, and Gmax [20]. To obtain MVIC for Gmed, patients were positioned on their sides with the test leg up at approximately 50% of hip abduction with slight extension and external rotation of the hip joint against maximum resistance applied to the ankle. The bottom hip and knee remained flexed. To obtain the MVIC for TFL, patients were positioned supine with the test leg flexed, the knee extended, and maximal hip joint internal rotation while performing hip flexion against the maximum resistance on the ankle. To obtain the MVIC for the Gmax, the patients adopted a prone position with the test leg flexed at 90
The Statistical Package for the Social Science (SPSS) version 25.0 software (IBM Inc., Armonk, NY, USA) was used for the data analyses. The one-sample Kolmogorov-Smirnov test was used to test for data normality. A one-way repeated-measures analysis of variance was used to compare Gmed, TFL, and Gmax activity during PD-N, PD-IR, and PD-ER. Statistical significance was set at 0.05. If a significant difference was found, Bonferroni adjustment was performed (
Results
Significant differences in muscle activity were observed among the three different PD conditions for Gmed (
Comparison of muscle activity (% maximum voluntary isometric contraction) in the gluteus medius, the tensor fasciae latae, and the gluteus maximus among various hip rotation positions during pelvic-drop exercise
Comparison of muscle activity (% maximum voluntary isometric contraction) in the gluteus medius, the tensor fasciae latae, and the gluteus maximus among various hip rotation positions during pelvic-drop exercise
Abbreviations: SD, standard deviation; CI, confidence intervals; PD-N, pelvic drop with neutral hip; PD-IR, pelvic drop with hip internal rotation; PD-ER, pelvic drop with hip external rotation.
Gmed was significantly greater during PD-IR than during PD-N (
Comparison of muscle activity in the gluteus medius, tensor fasciae latae, and gluteus maximus among different hip rotations during pelvic drip exercises (PD). Abbreviations: PD-N, PD with neutral hip; PD-IR, PD with hip internal rotation; PD-ER, PD with hip external rotation. 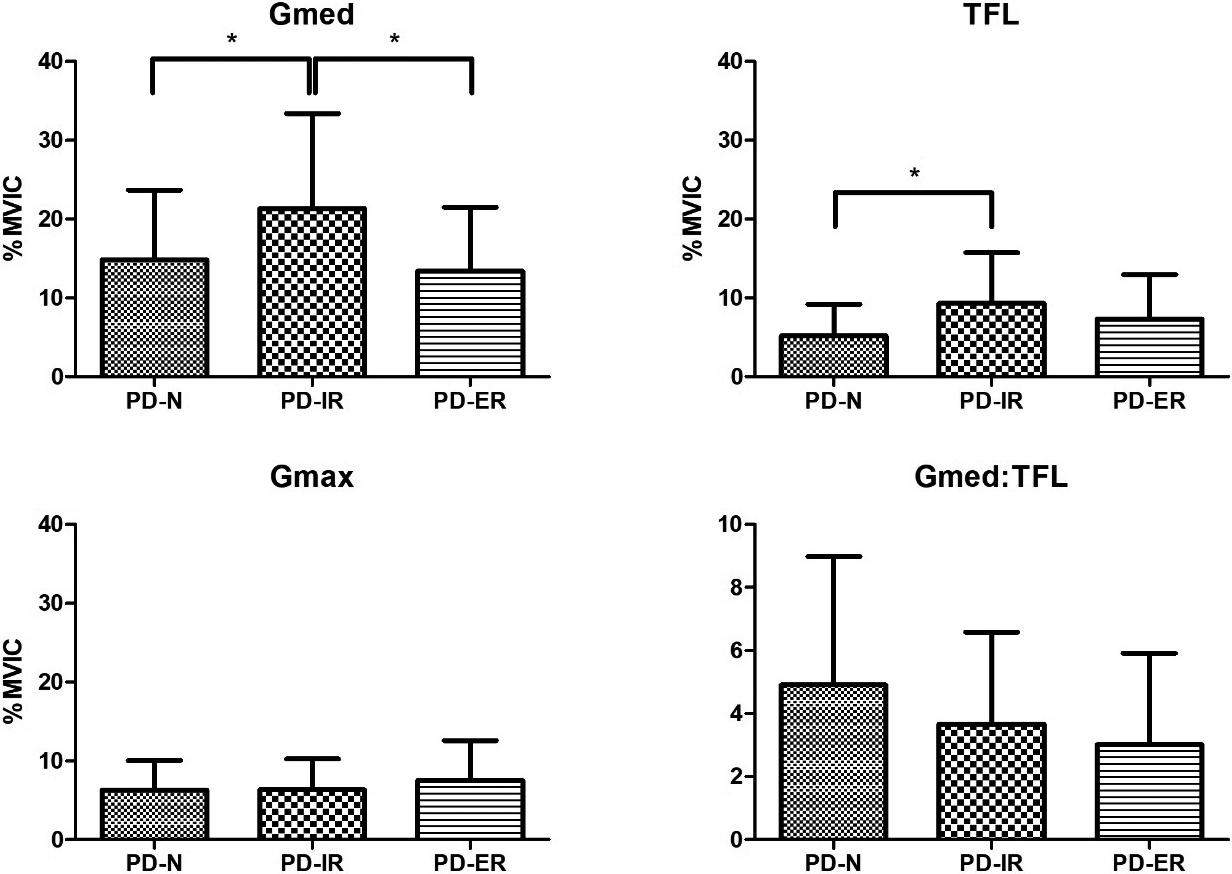
This study aimed to compare Gmed, TFL, and Gmax activities during three different PD conditions (PD-N, PD-IR, and PD-ER) in patients with Gmed weakness. The PD-IR group showed significantly greater Gmed activity than the PD-N and PD-ER groups as well as greater TFL activity than the PD-N group. These results partially support our hypothesis.
The Gmed muscle activity was significantly greater in PD-IR than in PD-N (by 6.521%) and PD-ER (by 7.975%). These results are consistent with those of previous studies [8, 24]. Moneteiro et al. reported that PD-IR showed significantly greater Gmed activity than PD-ER in healthy participants. Letafatkar et al. also demonstrated that healthy participants or those with genu varum showed significantly greater Gmed activity in PD-IR than in PD-ER [8, 24]. There were two possible mechanisms. First, the hip joint position change might have resulted in a change in the length-tension curve. In the neutral hip position, Gmed may have been isometrically contracted without a change in length. The internal rotation of the hip joint slightly lengthened the Gmed. The length of the Gmed could be increased, which can produce more muscle activity by sarcomeric changes in the muscle during PD-IR. Thus, Gmed was placed at a preferable position for optimal activation [10, 11, 13, 16, 24]. Second, the patients were required to maintain isometric hip IR in the PD-IR position. Increased external rotation forces enhanced Gmed activity [25]. Specifically, the anterior and middle fibers of Gmed play an important role in hip internal rotation [25, 26]. The results indicate that PD-IR is very effective at targeting Gmed weakness and preferentially activating the Gmed. These findings may be of clinical relevance.
PD-IR also elicited significantly greater TFL activity than PD-N (by 4.077%). In contrast, previous studies demonstrated that hip internal rotation produced significantly less or no significant difference in TFL activity compared to neutral hip or hip external rotation during side-lying hip abduction, side-sling plank, and PD [8, 11, 13]. In performing this task, TFL induces hip abduction and provides pelvic stabilization. The hip internal rotation position had a narrower base of support than the neutral hip position. Therefore, many muscles may be required to maintain pelvic alignment in this position. Fortunately, TFL activity during three different forms of PD showed lower level of activation (
Gmax activity showed no significant difference among the three PD conditions and elicited low-level activation (
Although Gmed activity was significantly increased in PD-IR group, the Gmed:TFL activity ratio showed no significant changes among exercises. This unexpected result may be due to the level of activation of muscles. As discussed previously, TFL activity during the three PD conditions showed relatively lower activation. Therefore, although there were several significant absolute differences in muscle activities among the exercises, the ratio that was affected relatively showed no significant difference. Nevertheless, because synergistic muscles act simultaneously and affect each other throughout the movement, determining both relative and absolute muscle activity would be meaningful [13, 15]. Based on these results, clinicians may be able to selectively prescribe PD with hip rotation for individuals with Gmed weakness.
This study has several limitations. First, the long-term effects of PD with three different hip rotations on hip abductor muscle activity could not be determined due to the cross-sectional nature of this study. Second, only participants 24–29 years of age were studied. Third, surface EMG signals of the middle fiber of the Gmed are vulnerable to cross-talk from the surrounding muscles [28].
Conclusions
This study investigated the effects of hip rotation on Gmed, TFL, and Gmax activity and Gmed:TFL activity ratio in patients with Gmed weakness. The Gmed activity was significantly greater in the PD-IR group than in the PD-N and PD-ER groups. TFL activity was also significantly greater in the PD-IR group than in the PD-N group. Thus, PD-IR is recommended to achieve greater Gmed activation and concurrently, preserve the Gmed:TFL activity ratio. Further studies are needed to determine the long-term effects of the three PD conditions on Gmed, TFL, and Gmax activity in patients of all ages with Gmed weakness.
Author contributions
All authors contributed equally.
Ethical considerations
This study was approved by the Institutional Review Board of Baekseok University (BUIRB-202202-HR-039). Written informed consent was obtained from all participants.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.