
Abstract
BACKGROUND:
A passive-control foot press trainer (PFPT) based on spring resistance aims to strengthen the ankle joint, similar to heel raise exercise (HRE).
OBJECTIVE:
To compare the muscle activity of the tibialis anterior, gastrocnemius medialis, gastrocnemius lateralis, rectus femoris, and biceps femoris between PFPT and HRE.
METHODS:
Eight healthy women performed four exercise conditions: PFPT forefoot (PFPT FF), PFPT rearfoot (PFPT RF), HRE at the floor level (HRE F), and HRE on the block (HRE B). During exercise, muscle activity was measured using surface electromyography and subsequently converted to percentages of maximum voluntary isometric contraction.
RESULTS:
Tibialis anterior showed the highest activity in PFPT FF, with significant difference from other conditions. Gastrocnemius medialis and lateralis demonstrated the highest activity in HRE B; Rectus femoris showed the highest activity in PFPT RF, showing significant differences from other conditions (
CONCLUSIONS:
Lower leg and thigh muscle activity between PFPT and HRE had similarities and differences. Future studies should analyze the long-term effects of PFPT, including on patients with musculoskeletal and nervous system injuries.
Keywords
Introduction
Stroke, one of the most prevalent cerebrovascular diseases, is the third leading cause of death in the member countries of the Organisation for Economic Co-operation and Development. It is characterized by the onset of chronic neurological disorders resulting from brain tissue damage [1, 2, 3]. The location and size of the affected area determine the extent to which a stroke can impair physical and mental abilities [4], significantly restricting various bodily functions particularly those of the upper and lower extremities. These limitations in daily activities can markedly reduce the overall quality of life. Owing to medical advancements, the survival rate of patients with stroke has increased; currently, 70%-75% of survivors experience persistent disabilities [5, 6]. Physical capacity reportedly decreases by approximately 40% in stroke survivors compared to healthy individuals, mainly owing to the loss of muscle strength and excessive activation, leading to functional deficits [7].
Repetitive concentric and eccentric actions of the distal lower extremity muscles are crucial for optimizing the performance of everyday activities [8]. However, stroke survivors often face challenges in walking because of various factors, including sensory impairment, muscle weakness, and stiffness [9, 10, 11]. Approximately 20% of stroke survivors experience foot drop, which impacts walking and other daily activities [4]. Consequently, improving walking and lower extremity motor functions is critical for predicting stroke-related disability and is considered a priority in stroke rehabilitation [12, 13, 14].
The strength of ankle dorsiflexion on the paretic side plays a key role in determining timed up-and-go performance in patients with spastic hemiparesis [15]. Overactivity of the tibialis anterior (TA) during electromyography (EMG) assessments causes forefoot varus during the stance phase of walking [16]. Conversely, the ankle plantarflexors generate most of the propulsive force needed for forward progression during walking [17]. Cooper et al. reported a significant correlation between ankle plantarflexor weakness and knee hyperextension during the mid-stance phase [18].
Traditional rehabilitation training to recover the motor function of the lower extremities of patients with hemiplegia due to stroke involves intensive exercise programs in the form of passive, active assistance, and active and resistance exercises in stages according to the motor function status of the patient’s lower extremities [19, 20, 21, 22, 23]. Among the various strengthening exercises, resistance training with eccentric contraction promotes neuromuscular activation after stroke [24, 25]. Eccentric training uses muscle contractions to increase length, stimulate collagen synthesis in muscles and tendon systems, and promote muscle cell growth and production [26]. According to Eng et al., eccentric strength is better preserved than concentric strength following a stroke [25]. This suggests that strength training using eccentric contractions provides stronger training stimuli. Heel raise exercises (HRE) in a standing position are performed clinically by repeatedly strengthening the eccentric and concentric phases of the ankle plantarflexors [27, 28].
The frequency and duration of exercises directly impact the recovery of the patient’s normal abilities; therefore, providing repetitive training is important. However, considerable physical effort from the therapist is necessary to perform manual therapy techniques and repetitive motions, which can lead to significant musculoskeletal strain [29]. Training equipment and robots are being developed and used to complement and restore various lower-extremity motor functions. Kubota et al. introduced a robot for eccentric contraction training of the TA [30]. The robot allows users to perform exercises while seated, with one foot secured to the footplate of the robot. Force sensors embedded in the footplate capture data on the force exerted at the toe tip, which is visualized through computer graphics. This setup enables the trainee to adjust the exerted force by referencing this visual data. When resistance was applied in the dorsiflexion direction on the footplate where the user’s feet were secured, the TA underwent eccentric contraction training based on the displayed target force. Simultaneously, plantarflexors also engaged in concentric contraction to counter this resistance. The possibility of improving walking ability by applying robot-assisted eccentric contraction training in older people has been reported, and a study on chronic stroke with hemiplegia reported a decrease in the Timed Up and Go and Co-Contraction Index Score of the TA and gastrocnemius (GCM) [31]. The Eccentron device by BTE Technologies Inc. (Hanover, MD, USA) allows for eccentric strength exercises of the lower extremities in a sitting position using a footrest for resistance and is currently utilized in clinical settings [32]. However, owing to the inherent design limitations of stepper-type exercise devices, this method primarily involves repetitive pushing motions while seated, which predominantly targets specific muscles. This restricts the individual’s ability to engage in weight-bearing exercises that simulate standing or walking, which are crucial for comprehensive lower extremity training. Additionally, these limitations prevent the device from providing a holistic approach to muscle strengthening across the entire lower extremity. A Motorized Ankle Stretcher (MAS) was introduced to improve ankle dorsiflexion joint range of motion (ROM) and maximize recovery of lower extremity motor function by gradually stretching the calf muscles of the lower leg in a standing position. A comparison of the existing stretching board for stroke showed that the MAS group had significant improvements in ankle ROM, balance control, and gait performance [33]. However, although MAS has the advantage of providing stretching by supporting gravity in the standing position, there are limitations in applying active muscle strengthening.
Various interventions are being implemented to effectively rehabilitate gait disorders and lower extremity dysfunction in patients with stroke and hemiplegia. However, few exercise devices can learn gait patterns by strengthening muscles through concentric and eccentric resistance exercises of the ankle joint and by providing resistance exercises to the ankle for each gait cycle. In the context of current ankle exercise robotic devices and gait training robots, accessibility is hindered by their limited ease of use and convenience.
Previously, we developed the passive-control foot press trainer (PFPT) to enhance lower-limb muscle function and facilitate gait improvement through targeted ankle exercises [34]. The PFPT employs forefoot and rearfoot pressing exercises using a spring-based resistance pedal and is designed for use in a standing position to take advantage of gravity. This setup also allows for repetitive training of walking patterns while standing. The current study primarily aimed to evaluate the effectiveness of the newly developed PFPT in strengthening lower-limb muscles by comparing its performance with that of the commonly used HRE, which is traditionally employed in clinical settings to enhance ankle muscle strength. Before extending this intervention to patients with stroke, we conducted a preliminary study involving healthy adult women to establish a baseline for its effectiveness and applicability.
Materials and methods
Participants
The Institutional Review Board of the Korea National Rehabilitation Center approved the study protocol, which conformed to the tenets of the Declaration of Helsinki (No: NRC-2022-03-025; date of approval: April 26, 2022). The purpose and procedures of the study were fully explained to the participants, and all participants provided informed consent. In this study, eight healthy adult women were selected based on the following inclusion criteria: no history of injury to the right leg within the past 6 months, no surgical treatments on the legs within the previous year, and no diagnosed neurological disorders that could influence motor function. Exclusion criteria were strictly defined to maintain the integrity of the study results. Individuals with any current or recent musculoskeletal, neurological, cardiovascular, or degenerative pathologies that could interfere with exercise performance were excluded. Additionally, potential patients with medical contraindications that would prevent safe participation in the study were also excluded. Furthermore, all participants were screened to ensure they had no prior injury history that might confound the outcomes in the four exercise conditions tested.
PFPT
The PFPT is designed to support a person’s body weight in a standing position and to repeat self-initiated dorsi-plantar flexion of the ankle. The equipment has a plate on which the user can stand and perform exercises, and a spring-replaceable pedal is attached to the center of the plate. It is designed in the form of a spring-based pedal for eccentric contraction of the muscles around the ankle, and the spring strength is divided into three levels and can be selectively applied according to the strength condition. A handle was attached to the side of the plate to maintain a stable posture during exercise, and an elastic band was added when necessary to enable a combination of exercises of various strengths.
Passive-control foot press trainer (PFPT).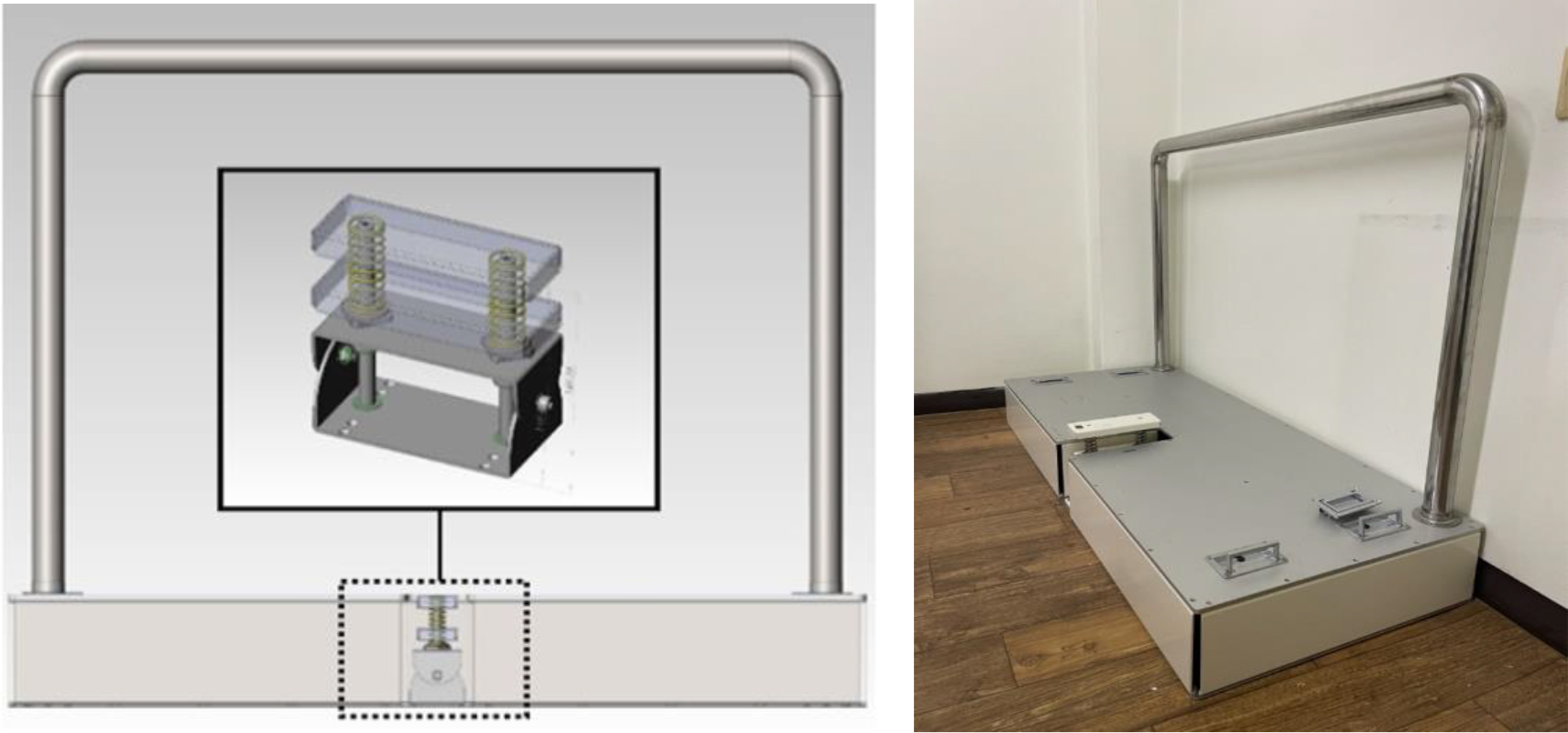
Ankle exercises using the PFPT included two types of movements. The “forefoot pressing movement” involves pressing the front part of the foot while standing, targeting ankle-centric muscle contractions. This movement induces concentric contractions of the plantarflexors and eccentric contractions of the dorsiflexors to enhance ankle stability and strength. The “rearfoot pressing movement” involves pressing the heel of the foot and targets comprehensive lower limb muscle contractions. This movement induces concentric contractions of the hip and knee extensors and dorsiflexors and eccentric contractions of the hip and knee flexors and plantarflexors. Such extensive muscle activity is expected to enhance lower body balance and overall mobility. Furthermore, by utilizing the longitudinal space around the pedal, the foot pressing movements are specifically designed to train partial motions of the stance phase in one foot while the opposite foot performs swing phase movements. This arrangement facilitates the learning of specific segments of the walking pattern (Fig. 1). However, in this study, walking pattern training was not conducted, and only ankle exercises in a standing position using the PFPT were performed.
Each participant attended two sessions, during which they engaged in ankle exercises under two conditions each using the PFPT and for HRE. After the first visit, a rest period of at least 24 h was allowed before the next exercise condition to prevent fatigue, and the order of the exercise conditions was randomly applied. The number of exercises was set to a 40-repetition maximum under all conditions, and a metronome (36 BPM comfortable speed) was used to perform the exercises at a constant speed.
Exercises using PFPT (A), HRE at floor level (B), and forefoot on the block (C). A. PFPT ankle exercises (left: PFPT FF, right: PFPT RF); B. HRE on the floor level (HRE F); C. HRE with forefoot on the block (HRE B). Abbreviation: PFPT 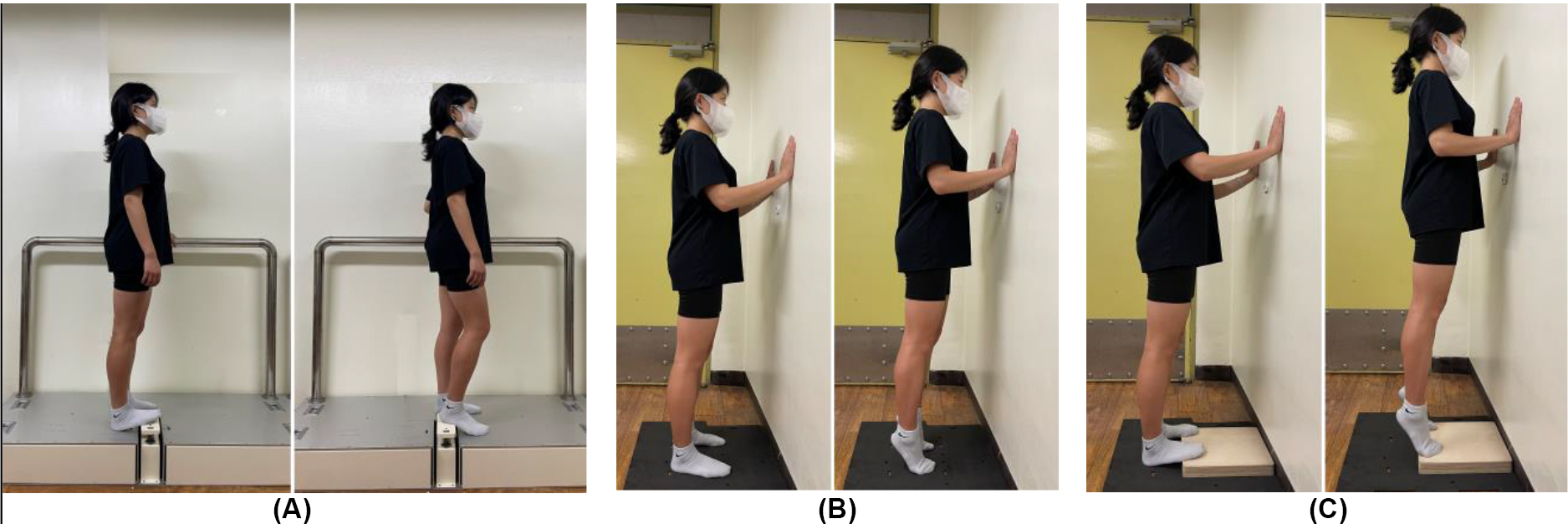
PFPT ankle exercises were divided into forefoot (PFPT FF) and rearfoot (PFPT RF) conditions depending on the area where the pedal device was pressed (Fig. 2A). For the PFPT FF exercise, participants were instructed to stand with the pedals in front of them, feet shoulder-width apart, and to look forward. The forefoot should be placed on the pedal and the rearfoot on the floor. The parallel bar located on the side should be lightly grasped. The pedal should be slowly pressed and held with the forefoot in accordance with the metronome signal and then slowly returned to the initial position. For the PFPT RF exercise, participants were instructed to stand with the pedals behind them, place the rearfoot on the pedal, and place the forefoot on the floor. In the initial position, with the hips and knees flexed naturally, the pedal should be pressed with the rearfoot in accordance with the metronome signal and maintained at knee extension and then slowly returned to the initial position. After randomly performing either PFPT FF or PFPT RF, a 20-min rest period was provided, and the remaining condition was performed. To prevent compensation and maintain postural alignment during the PFPT exercises, a physical therapist stood nearby and provided verbal comments.
HRE was divided into heel raise exercises at the floor lever (HRE F) and heel raise exercises on the block (HRE B). In HRE F, participants were instructed to raise their heels as high as possible and then drop them in time with the metronome signal until they touched the floor (Fig. 2B). In HRE B, participants were instructed to raise both heels as high as possible with the forefoot on a 5 cm block. After a slight pause at the top position, participants were instructed to slowly drop their heels onto the floor (Fig. 2C) [35, 36]. To maintain balance during the exercise, both HRE F and HRE B were performed while standing in front of a wall and lightly touching it.
To acquire EMG signals, surface EMG data were recorded using a Trigno wireless EMG system (Delsys, Inc., Boston, MA, USA). EMG data were collected from the TA, GM, gastrocnemius lateralis (GL), rectus femoris (RF), and biceps femoris (BF) on the dominant side (the preferred leg for kicking a ball). Electrodes were placed over the bellies of the muscles under investigation. To reduce the impedance interface between the skin and electrodes, the tested areas were shaved and cleaned using abrasive pads for skin preparation and alcohol wipes. The surface EMG electrode attachment site was determined according to the SENIAM guidelines, which is the gold standard for surface electrode placement [37]. Participants performed maximal voluntary contraction (MVC) three times for each muscle before exercise. The MVC trials for each muscle were based on muscle testing using an anatomical guide for EMG [38]. The sampling rate for the EMG signal was set at 2,000 Hz, and the bandpass filter was set between 20 and 450 Hz. Raw data from the TA, GM, GL, RF, and BF during the PFPT and HRE were transformed into root mean square (RMS) data. The mean RMS of the maximum voluntary isometric contraction (MVIC) was calculated for each muscle. All EMG data are expressed as percentages of MVIC (%MVIC). Excluding 5 times each from the start and end of the exercise, 30 times were analyzed and expressed as the mean normalized EMG peak (%) [39].
Data analysis
We used SPSS (version 21.0; IBM Corp., Chicago, IL, USA) to determine the statistical significance of the lower limb muscle %MVIC across different exercise conditions. Before conducting further analyses, we verified the normality of the data using the Shapiro-Wilk test [40]. One-way analysis of variance (ANOVA) was used, and the factor was set to four (PFPT FF, PFPT RF, HRE F, and HRE B). The Bonferroni post-hoc test was performed, and significance was set at
%MVIC of the lower-limb muscles during PFPT and HRE (Unit: %MVIC)
%MVIC of the lower-limb muscles during PFPT and HRE (Unit: %MVIC)
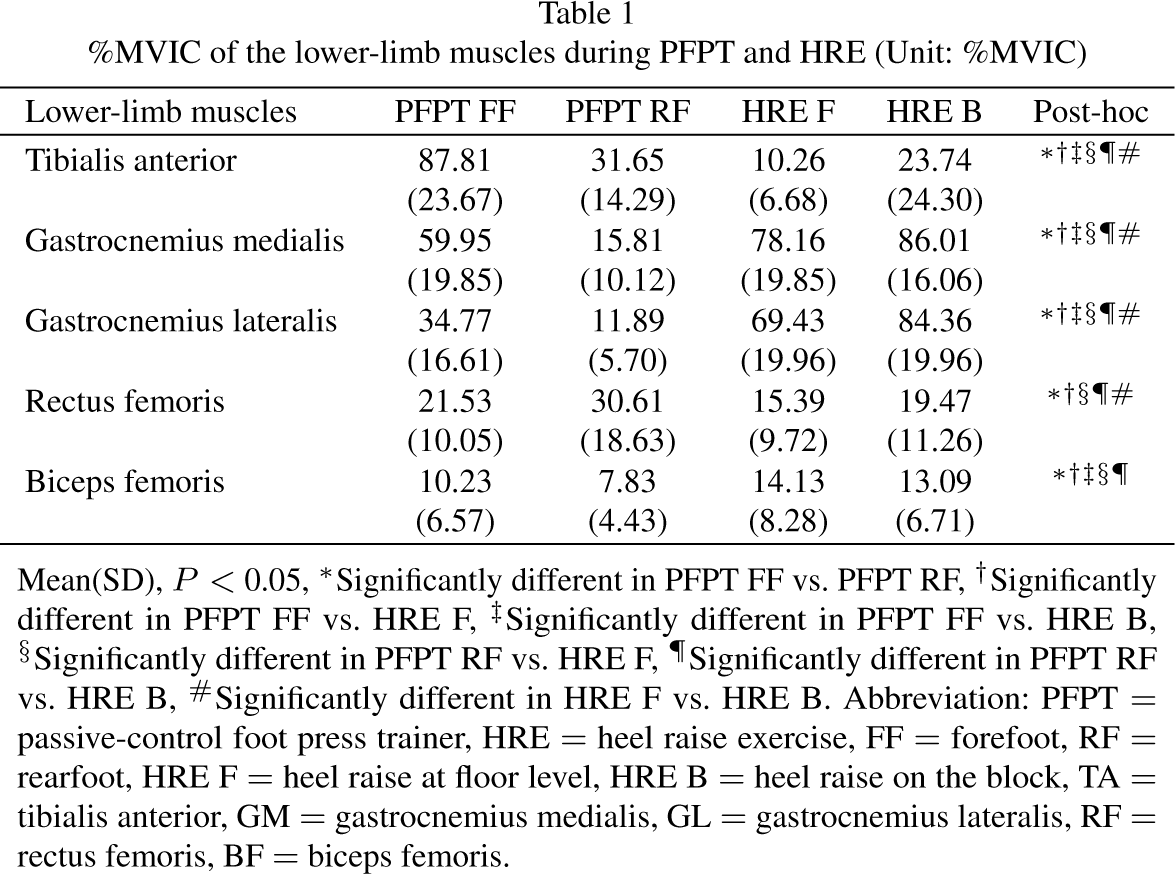
Mean(SD),
Mean of EMG peak (%) of the calf muscles. 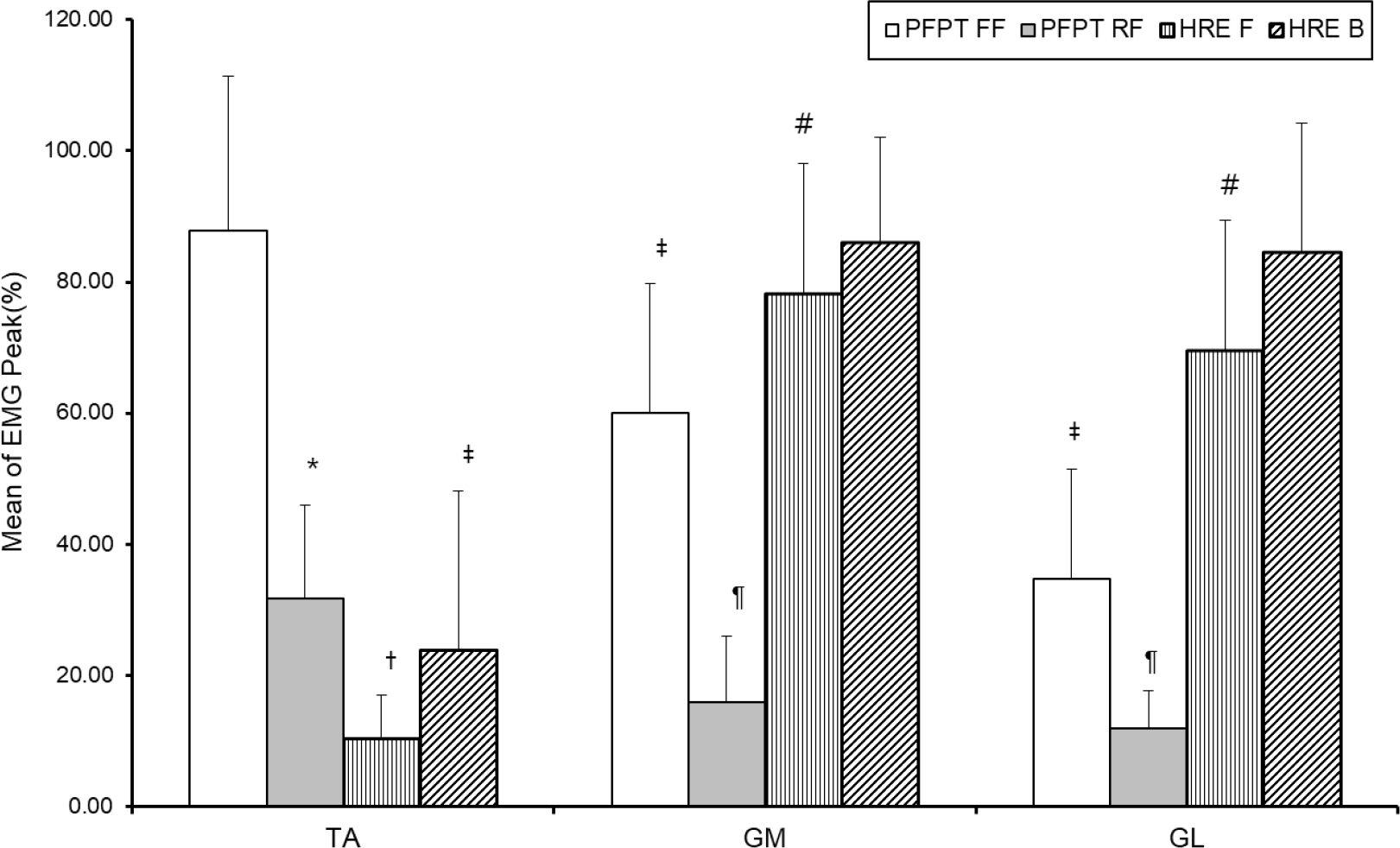
Mean of EMG peak (%) of the thigh muscles. ∗Significantly different in PFPT FF vs. PFPT RF, †Significantly different in PFPT FF vs. HRE F, ‡Significantly different in PFPT FF vs. HRE B, §Significantly different in PFPT RF vs. HRE F, ¶Significantly different in PFPT RF vs. HRE B, # Significantly different in HRE F vs. HRE B. Abbreviation: PFPT 
The characteristics of the participants were as follows: age, 22.3
We previously developed the PFPT to improve lower-limb muscle function and gait through ankle exercises [34]. The PFPT allows forefoot and rearfoot pressing exercises after placing the sole of the foot on a spring-based resistance pedal device in a standing position exposed to gravity. Therefore, in this study, before applying the developed PFPT to stroke patients, four ankle exercises, including two ankle resistance exercises and two HRE ankle exercises using the PFPT, were performed on young adult women. This preliminary study confirmed the effectiveness of the equipment by comparing muscle activity between conditions.
The %MVIC of the TA was highest in PFPT FF. The initial position during PFPT FF was a dorsiflexed ankle with the forefoot raised on the pedal. The pedal was then gradually pressed against the forefoot and returned to its initial position through concentric dorsiflexion. During this process, the muscle activity of TA, an ankle dorsiflexor, appeared to be greatly activated, which may indicate enhanced muscle strength and improved ankle stability, both essential for efficient gait performance and fall prevention. During HRE, the %MVIC of the TA was higher in HRE B than in HRE F. As HRE B was performed with the forefoot raised on a 5-cm-high block, muscle activity of the TA appears to have increased from the initial ankle dorsiflexed position to the full ROM.
The %MVIC of the GM and GL generally showed high activity in HRE. HRE has been widely used clinically to strengthen the GCM, which is a strong plantarflexor. In a study by Lee et al., patients with stroke were divided into two groups (HRE B and HRE F), and the same amount of training was performed. Significant increases in plantarflexor power, walking speed, and cadence were reported during HRE B [35]. These results were explained by the fact that the use of the blocks enabled concentric and eccentric contractions of plantarflexors throughout the entire ankle ROM. In this study, a higher %MVIC was confirmed in all muscles, except the BF, during HRE B exercise than during HRE F; the %MVIC of the GM was higher than that of the GL under all exercise conditions. According to Fiebert et al., the GM showed higher muscle activation than the GL during plantar flexion in a weight-bearing state; however, as the load increased, the gap in muscle activation between the GM and GL decreased [41]. In this study, the difference in muscle activation between the GM and GL during HRE B was smaller than that during HRE F, which suggests that HRE on the block is more intensive owing to increased ankle ROM. Therefore, a significant improvement may have been observed in patients with stroke in previous studies that employed HRE B.
The %MVIC of the RF was significantly higher in PFPT RF than in the other three conditions (
The %MVIC of the BF was highest in HRE F and lowest in PFPT RF. Excluding PFPT RF, PFPT FF, HRE F, and HRE B were all performed in a standing position; therefore, knee extension had to be maintained. However, in PFPT RF, the main movement started from a flexed knee position and concentric contraction of the knee extensor. Therefore, the BF, which is a knee flexor, would have contributed to maintaining knee extension through co-contraction with the knee extensor. Additionally, it is believed that a relatively low %MVIC activity occurred owing to spring elasticity during knee flexion when returning to the initial posture.
Most muscles of the lower extremities undergo repeated phasic activation during the gait cycle. The TA slows ankle plantar flexion through eccentric contraction upon heel contact and prevents foot drag during the swing phase. Plantarflexors, including the GCM, eccentrically control the forward movement of the tibia relative to the foot during the stance phase and provide propulsion for forward advancement during heel-off. The quadriceps femoris absorbs shock through eccentric contraction immediately after heel contact and prevents excessive knee joint flexion; the knee flexors assist in hip extension in the early stance phase and contribute to knee joint stability through simultaneous activity with the knee extensors [42]. In this study, we confirmed the activation of overall lower limb muscles, including the TA and RF, in exercises using the PFPT compared to HRE. HRE particularly increased activity in the GCM. Consequently, exercises using the PFPT have demonstrated potential in enhancing the stability of ankle and knee joints, thereby contributing positively to gait dynamics. Our findings suggest that the PFPT effectively targets specific muscles such as the TA and RF for strengthening, whereas the HRE predominantly activates the GCM muscles. For a comprehensive approach to strengthening all ankle muscles, combining PFPT with HRE might be beneficial. This integrated approach could offer a more inclusive muscle strengthening regimen for the ankle, enhancing joint stability and improving overall gait.
Our study has several limitations. First, it included only a small number of healthy women volunteers. Future research should include a larger number of participants and encompass patients with neuromuscular injuries who require lower limb strengthening. Second, given the challenges of dorsiflexion in patients with stroke and plantarflexor spasticity, it is critical to conduct further studies to verify the significance and identify appropriate target groups for forefoot and rearfoot exercises using the PFPT. Third, this study did not evaluate whether ankle exercises using the PFPT lead to significant improvements in gait patterns. This should be address by developing a customized exercise program that integrates ankle exercises and gait pattern training with the PFPT. After implementing this program, analyzing balance and gait-related variables will be crucial to evaluate the effectiveness of the intervention. Employing surface EMG, a noninvasive technique, enhances our understanding of muscle activity and is widely used in muscle physiology research [43]. Moreover, research could benefit from integrating EMG with 3D motion capture systems and IMU-based motion analysis to evaluate limb function under various conditions.
In future developments, the advancement plan for the PFPT includes integrating electronically controlled motors to provide adjustable resistance and continuous passive movement modes. Additionally, the system will offer various training programs and real-time feedback through pressure sensors, enhancing the engagement and effectiveness of repetitive exercises.
Conclusion
During the forefoot and rearfoot pressing ankle exercises using the PFPT, significant changes in the activity of the lower leg and thigh muscles were observed compared to those during HRE. These findings demonstrate that the PFPT can be effectively used for targeted strengthening of specific muscles. Additionally, for a more comprehensive strengthening of all ankle muscles, integrating PFPT with HRE may be beneficial. This combined approach could provide a more inclusive muscle-strengthening regimen for the ankle.
Future research should focus on validating the effectiveness and applicability of the PFPT for improving gait and posture correction in the lower extremities, particularly in patients with various neuromuscular system injuries. Moreover, there is a need to enhance the convenience of using the PFPT, develop training protocols that leverage its unique features, and offer diverse content to alleviate monotony and foster engagement during repetitive exercises.
Funding
This study was supported by a grand (#NRCTR-IN-23006) of the Translational Research Center for Rehabilitation Robots, Korea National Rehabilitation Center, Mi nistry of Health & Welfare, Korea.
Ethical considerations
All study participants provided informed consent, and the study design was approved by the appropriate ethics review board at the National Rehabilitation Center (#NRC-2022-03-025).
Author contributions
CONCEPTION: Young-Hyeon Bae, BumChul Yoon, and Byung-Woo Ko.
PERFORMANCE OF WORK: Byung-Woo Ko, Young-Hyeon Bae, and BumChul Yoon.
INTERPRETATION OR ANALYSIS OF DATA: Byung-Woo Ko, Young-Hyeon Bae, BumChul Yoon, and Joon-Ho Shin.
PREPARATION OF THE MANUSCRIPT: Young-Hyeon Bae, BumChul Yoon, Byung-Woo Ko, and Joon-Ho Shin.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Young-Hyeon Bae, BumChul Yoon, and Byung-Woo Ko.
SUPERVISION: Young-Hyeon Bae and BumChul Yoon.
Footnotes
Acknowledgments
We would like to thank Ms. Ji-Hyun Lim for her assistance with data collection.
Conflict of interest
The authors have no conflicts of interest to declare.