
Abstract
BACKGROUND:
Trunk muscle thickness and brightness are associated with injuries.
OBJECTIVE:
This study compared trunk muscle thickness and brightness between female college athletes with and without history of low back pain.
METHODS:
15 sprinters, 22 volleyball-, and 18 basketball players, all females, were included. The participants were grouped based on the presence of low back pain. Short-axis ultrasound images of the rectus abdominis, external oblique, internal oblique, transverse abdominis, and lumbar multifidus were obtained. The muscle brightness was calculated after selecting the region of interest for each muscle. Muscle thickness and brightness in both groups were compared.
RESULTS:
In sprinters, the right lumbar multifidus thickness was significantly thinner in the low back pain group (24.66
CONCLUSIONS:
Low back pain in female college athletes may not be related to trunk muscle thickness and brightness.
Participant characteristics based on the sport engaged
Participant characteristics based on the sport engaged
Group characteristics are expressed as mean
Athletes have a higher frequency of history of low back pain (LBP) than non-athletes [1]. The frequency of lumbar injuries caused by sports was investigated, and in sprinters, the frequency of lumbar injuries was the highest compared with all other injury sites [2]. Approximately 40% of female college volleyball players have experienced LBP in the past year [3], indicating a high frequency of LBP in various sports. Those engaged in volleyball and basketball have 3.8 and 2.5 times higher instances of developing LBP compared with those who did not exercise regularly [1]. Thus, the prevention of low back disorders is necessary owing to the high frequency of LBP in athletes, regardless of the sport.
Quantitative factors such as trunk muscle thickness are involved in LBP [4, 5]. In middle-aged individuals with LBP, the cross-sectional area of the multifidus ipsilateral to the side of pain decreases [4]. In a study of young athletes, it has been established that the cross-sectional area of the lumbar MF and TrA thickness is significantly lower in cyclists with LBP than in healthy participants [6]. Additionally, in young soccer players, oblique abdominal muscle thickness is decreased in players with a history of LBP compared with healthy players [5].
In recent years, not only quantitative factors but also qualitative factors have been considered. Muscle brightness has gained popularity as an index that may be used to estimate the degree of adipose tissue and intramuscular fibrous within skeletal muscles. Muscle brightness is the degree of black and white (echo intensity) of the muscle on ultrasound images and is considered to be an estimation of muscle quality. High muscle brightness indicates a high degree of adipose tissue and intramuscular fibrous within skeletal muscle. A significant correlation between muscle composition calculated using muscle brightness, and that calculated by muscle biopsy has been reported [7], indicating the validity of evaluating muscle brightness.
Muscle brightness has also been reported to be related to muscle strength and injury. For example, reports indicate that muscle brightness is correlated with muscle strength in the elderly [8], suggesting the importance of muscle luminance assessment. In addition, the brightness of the peroneus longus muscle in individuals with chronic ankle instability (CAI) was higher on the CAI side than on the non-CAI side in their twenties [9]. Thus, it has been reported that muscle brightness is associated with the presence or absence of ankle joint injury, even in young adults. LBP and trunk muscle brightness in athletes may also be related, but the relationship between LBP and muscle brightness is unknown.
Since athletes have a high frequency of LBP, investigating whether muscle quality and thickness are related to LBP may help prevent LBP. Most investigations on muscle thickness and brightness in athletes have been conducted on male athletes [5, 6, 7, 8, 9]. Investigating whether muscle brightness and thickness are related to LBP in female athletes may aid in preventing LBP. Therefore, in this study, we aimed to clarify the relationship between the history of LBP, trunk muscle thickness, and muscle brightness in female athletes.
Methods
Participants
Fifty-five collegiate female athletes were included in this study (Table 1). Athletes from 3 sports were included: 15 sprinters in track and field, 22 in volleyball, and 18 players in basketball. Those with at least 5 years of athletic history were included. Eleven sprinters (73.3%) were at the national competition level, and four (26.7%) were at the regional competition level. Eighteen volleyball players (81.8%) were at the national competition level, and four (18.2%) were at the regional competition level. All basketball players (100%) were at the national competition level. All participants were members of the same university athletic team. Participants decided to participate in the study of their own free will after the teams in each sport were asked to participate in the study. To eliminate the influence of recent physical activity on muscle brightness, measurements were taken at least 12 h after the end of the exercise. Those with a history of spinal surgery were excluded.
The inclusion criteria for the LBP group were as follows: at least 5 episodes of LBP in the lifetime, at least 3 episodes in the past 3 years, and at least 1 episode within 6 months [10]. LBP was defined as pain between the 12th rib and the inferior end of the gluteal fold lasting more than 1 day. The participants were informed of the study in writing, and their consent was obtained before the study was conducted. This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the affiliated institution (Approval number: 1858-210218, Approval date: 2/18/2021).
Method for measuring muscle thickness. Ultrasound short-axis images of the right rectus abdominis muscle (A), right oblique muscle group (B), and right lumbar multifidus muscle (C).
Ultrasound imaging was performed using an ultrasound imaging system (Aplio 500, Toshiba Medical Systems) with a 10 MHz linear probe. The instrument settings were B mode, focus point of 2 cm, and gain of 100 dB, which were kept consistent during the measurements. The target muscles included the rectus abdominis, external oblique, internal oblique, transverse abdominis, and lumbar multifidus. Measurements were obtained from the sprinters on the right side, while volleyball and basketball players were measured on both sides. Because volleyball and basketball involve many asymmetrical movements, bilateral imaging was performed. The abdominal muscles were measured in the supine position, the lumbar multifidus was measured in the prone position, and the upper limbs were positioned on the side of the body. Additionally, the participants were instructed to breathe quietly while resting during the measurements [11]. One image was taken for each exhalation, and all measurements were performed by the same examiner (C.S.). The rectus abdominis (RA) was measured 3 cm lateral to the umbilicus [11]. The transversus abdominis (TrA) internal oblique (IO), and external oblique (EO) muscles were measured 2.5 cm anterior to the mid-axillary line at the midpoint between the inferior rib and iliac crest [11]. Furthermore, the lumbar multifidus (MF) was measured 2 cm lateral to the L4 spinous process [11]. The probe was applied perpendicular to the skin with minimal pressure, and two short-axis ultrasound images were obtained for each muscle [12].
Measurement of muscle thickness (Fig. 1)
Intraclass correlation coefficients (ICC) and Minimal detectable change (MDC)
Intraclass correlation coefficients (ICC) and Minimal detectable change (MDC)
Abbreviations: rectus abdominis (RA), transversus abdominis (TrA), internal oblique (IO), external oblique (EO), lumbar multifidus (MF).
Muscle thickness was calculated at 0.1 mm intervals using calipers on the ultrasound image. The locations of the fascia and vertebral arch were identified on ultrasound images. The maximum muscle thickness was used as the measurement for the RA. For the TrA, IO, and EO, the muscle thickness was measured at 2 cm from the TrA intersection [13]. The line connecting the vertebral arch to the subcutaneous tissue was measured for obtaining MF, and the maximum value was considered as the MF measurement. Two images were analyzed once, and the average value was calculated [12]. All analyses were performed by the same examiner (C.S.).
Muscle thickness
Muscle thickness is expressed as the mean
Muscle brightness was evaluated by computer-assisted 8-bit grayscale analysis using the standard histogram function in Image J (U.S. National Institutes of Health, Bethesda, MD, USA). Muscle brightness indicates muscle quality. High muscle brightness (high value) indicates a high amount of adipose tissue and intramuscular fibrous. The region of interest for muscle brightness was selected for each muscle to include the maximum part of muscle possible without the bone or surrounding fascia [11]. The mean muscle brightness in the region of interest was calculated and expressed as a value ranging from 0 (black) to 255 (white). Two images were analyzed once, and the average value was calculated [12]. All analyses were performed by the same examiner (C.S.).
Muscle thickness. Mean and standard deviation of trunk muscle thickness in sprinters, volleyball players, and basketball players. Sprinters: right side, Volleyball, and Basket players: right and left side * p < 0.05 and †p < 0.1.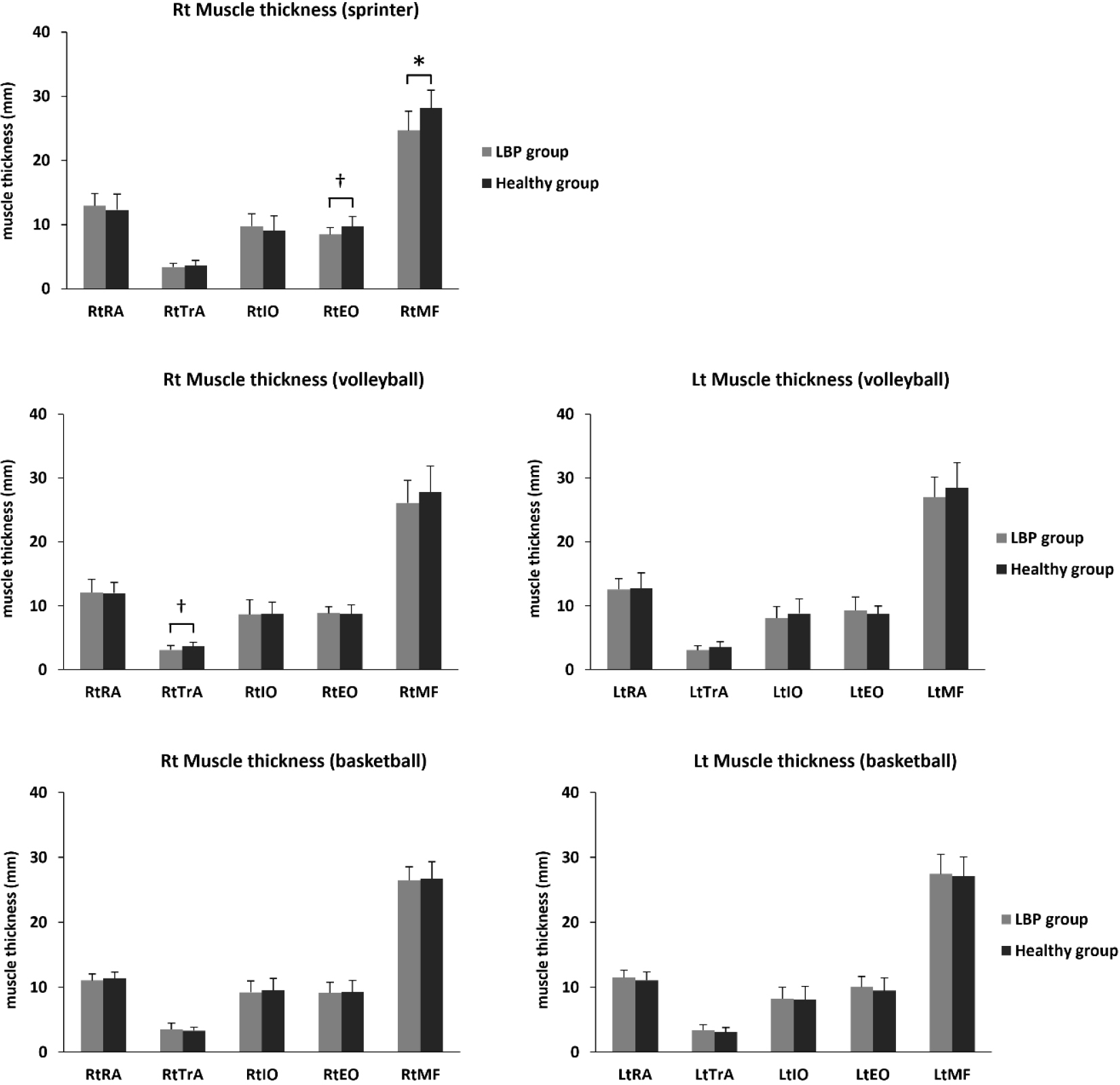
ICC (1,2) was used to examine the intra-rater reliability of muscle thickness and brightness measurements. Eight female university students were included in the ICC measurements performed by the examiner, and the measurements were identical to those used in the main experiment. The right side of the trunk was measured. We calculated the MDC with a 95% confidence interval (MDC95) using the following equation: MDC
Statistical analyses
Muscle brightness. Means and standard deviations of trunk muscle brightness in sprinters, volleyball players, and basketball players. Sprinters: right side, Volleyball, and Basket players: right and left side.
Muscle brightness
Muscle brightness is expressed as the mean
The Kolmogorov-Smirnov test was used to confirm data normality. Data on participants, muscle thickness, and brightness were compared between the LBP and healthy groups for each sport. Normally distributed items were compared between the two groups using an unpaired
Participant characteristics (Table 1)
Eight sprinters were classified into the LBP group and seven sprinters into the healthy group. Both LBP and healthy groups had eleven volleyball players each. Furthermore, 7 and 11 basketball players were classified into the LBP and the healthy group, respectively. There were no significant differences in age, height, weight, Body Mass Index, or athletic career between the two groups in any sport.
ICC and MDC95 (Table 2)
Table 2 shows the results of ICC and MDC95. The ICC (1,2) values of muscle thickness and muscle brightness measurements were
Muscle thickness (Table 3) (Fig. 2)
In sprinters, the right MF thickness was 24.66
Muscle brightness (Table 4) (Fig. 3)
In all sports, there was no significant difference in muscle brightness between the two groups for all muscles.
Discussion
In this study, we examined the relationship between the history of LBP, trunk muscle thickness, and brightness in female college athletes. The results revealed a relationship between a history of LBP and trunk muscle thickness in sprinters.
Sprinters exhibited a significant decrease in right MF thickness in the LBP group compared with the healthy group. Previous studies reported that LBP is related to MF thickness, and the results were similar in sprinters. For instance, the cross-sectional area of the lumbar MF is decreased in patients with chronic LBP compared with healthy participants [16], and the lumbar MF thickness changes during voluntary contraction are reduced compared with healthy participants [17]. Voluntary contraction of the MF muscle inhibits lumbar spine movement and increases lumbar spine stiffness in the neutral zone [18]. Thus, lumbar spinal stability may be reduced in sprinters with a history of LBP. A reduced MF thickness causes instability of the lumbar spine, which may lead to an increased risk of intervertebral disc and facet joint disorders. Furthermore, it has been reported that 100 m sprinting time is related to MF thickness [19], hence, competitive performance may be reduced in sprinters with low values of muscle thickness in the multifidus muscle.
In volleyball players, right TrA muscle thickness tended to be lower in the LBP group than in the healthy group, but there was no significant difference between the two groups. In this study, expect for one participant, the volleyball players were right-handed during the serving and spiking tasks, and those with a history of LBP tended to have lower TrA muscle thickness on the dominant side. However, there was no significant difference in TrA muscle thickness between the two groups. A study investigating the relationship between head and neck and upper extremity injuries and trunk muscle thickness in volleyball players revealed that TrA muscle thickness did not differ with varying histories of injury of the player, and these results were consistent with those in our study [20]. Alternatively, some reports indicate that adolescent female volleyball players with more than two years of experience have greater TrA muscle thickness than other women of the same age [21]. As the TrA was higher in volleyball players, the TrA may be used frequently in volleyball movements. However, the present study did not find a relationship between LBP and muscle thickness, and further investigations are mandated because TrA muscle thickness may be important in volleyball.
In this study, only the sprinter’s multifidus muscle thickness was related to a history of LBP. Previous studies have failed to reach a consensus on the relationship between LBP and muscle thickness. For example, in young soccer players, the cross-sectional area of the lumbar MF and TrA thickness does not change in the presence or absence of LBP [3, 22]. Conversely, it has been established that the cross-sectional area of the lumbar MF and TrA thickness is significantly lower in cyclists with LBP than in healthy participants [6]. The results of this study suggest that there may be no relationship between a history of LBP and trunk muscle thickness in female athletes, but further investigation is needed to make a definitive conclusion.
Additionally, changes in the TrA muscle thickness during voluntary contraction from rest were investigated. For example, the change in TrA muscle thickness during draw-in is smaller in patients with pre-existing LBP than in those without preexisting LBP [10]. In ballet dancers, it has been reported that the slide of the TrA during draw-in is smaller in those with a history of LBP than in healthy individuals [23]. Future studies, including studies investigating changes in muscle thickness during voluntary contractions, may clarify the relationship between LBP and trunk muscle thickness in female athletes.
No difference was found in muscle brightness between the healthy and LBP groups in any of the muscles in all sports. Based on the results of the present study, trunk muscle brightness may not be associated with LBP in collegiate athletes. It has been reported that trunk muscle brightness in healthy women aged 20–60 years is higher in women aged 40 years than in those in their twenties [11]. Since trunk muscle brightness increases with age, the presence or absence of a history of LBP may not cause differences in muscle brightness in collegiate athletes. However, reports indicate that the brightness of the peroneus longus muscle in individuals with chronic ankle instability is higher on the affected side than on the healthy side, even in young individuals [9]; therefore, further investigation is needed.
This study has several limitations. First, LBP severity was not assessed in this study. Differences in the severity of LBP may have affected the results. Second, the sample size was small. As this study was conducted on young female athletes, it was difficult to recruit a large number of participants. Therefore, it is desirable to recruit a larger number of participants and conduct further studies.
The results of this study suggest that LBP in female college athletes may not be related to trunk muscle thickness and brightness. Therefore, future research should focus not only on muscle morphology but also on muscle function and muscle activity during sports activities. The results of this study suggest that increasing the muscle thickness of the MF in sprinters may help prevent LBP.
Conclusions
Low back pain in female college athletes may not be related to trunk muscle thickness and brightness. In sprinters, MF thickness was significantly decreased in the LBP group compared to the healthy group, but no difference was observed between the two groups in the other sports. Regardless of the sport, muscle brightness was not associated with a history of LBP. Future research should focus not only on muscle morphology but also on muscle function and muscle activity during sports activities.
Author contributions
CONCEPTION: C.S. and M.E.
PERFORMANCE OF WORK: C.S.
INTERPRETATION OR ANALYSIS OF DATA: C.S.
PREPARATION OF THE MANUSCRIPT: C.S., H.Y., R.H., H.A., T.I., T.K. and M.E.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: C.S., H.Y., R.H., H.A., T.I., T.K. and M.E.
SUPERVISION: C.S.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the affiliated institution.
Funding
This study was supported by a Grant-in-Aid for Scientific Research (21K17556) from the Japanese Society for the Promotion of Science (JSPS) and a Grant-in-Aid from the Niigata University of Health and Welfare.
Footnotes
Acknowledgments
We would like to express our deepest gratitude to the team managers, coaches, and players who contributed to this study.
Conflict of interest
The authors declare that they have no competing interests.