
Abstract
BACKGROUND:
Hip flexion angle-torque may not be measured accurately due to the measurement posture.
OBJECTIVE:
Maximum isometric hip flexion torque was measured while excluding the effects of postural retention function and compensatory motion.
METHODS:
Experiment 1: Maximum isometric flexion torque of the hip joint was measured at 0∘, 30∘, 60∘, 90∘, and 105∘ in 195 participants. Experiment 2: Maximum isometric hip flexion torque of 33 participants was measured in standing and supine position at 0∘ hip flexion and in end-sitting and supine position at 105∘.
RESULTS:
Experiment 1: No interaction was observed between sex and hip angle, and hip flexion torque was minimum at 0∘ hip flexion and maximum at 105∘ hip flexion in both sexes (
CONCLUSIONS:
Maximum isometric hip flexion torque showed greater joint angle-torque characteristics in deep flexion than in shallow flexion of the hip when excluding the effects of postural retention function and compensatory motion.
Keywords
Introduction
Skeletal muscle strength and mass are known to decline with age [1]. Age-related changes are more pronounced in the extremities, with the decline more pronounced in the lower extremities [1, 2]. It has been reported that the lower extremity muscle with the most significant age-related loss of muscle mass is the psoas major [3]. The psoas major is responsible for the rapid forward movement of the lower limbs and shows great muscular activity during running and fast walking [4]. In addition, the psoas major is the only muscle that connects the lumbar spine to the lower limbs [5] and performs an important role in maintaining stable posture during activities of daily living. Therefore, the hip flexor muscles, including the psoas major, are an important muscle group in strength training.
A variable load machine that follows joint angle-torque characteristics has been reported as a safe and efficient way to perform strength training [6]. The joint angle-torque, applied during joint motion, varies with the change in angle, and training with this loading pattern is highly effective in training for the elbow and knee joints [7, 8]. Therefore, using a loading pattern in strength training that corresponds to the hip flexion angle-torque characteristics of the hip flexor muscle should also be an effective training method. In previous studies, torque exerted was reported to decrease with increasing hip flexion angle [9, 10, 11, 12, 13]. However, in these reports, the posture of the subjects during measurement was a side-lying position or sitting on the edge of a bed as the torque exerted, including that of postural retention, was assessed. Thus, the maximum isometric hip flexion torque may not have been measured accurately. In a report [14] with measurements taken with the subject in the supine position, the lumbar pelvis was fixed with a belt. Thus, lumbar pelvis motion associated with hip motion was restricted, which may have affected the maximum isometric hip flexion torque measurement. A recent simulation study using a mathematical model has reported that hip flexion torque does not decrease with increasing hip flexion angle and is maintained in the deep flexion range [15]. A study using morphological data of skeletal anatomical specimens, reported that the contribution rate of torque exerted by the iliopsoas increases as the hip flexion angle increases [16]. In an experiment in which muscle biopsies were taken from the psoas major at different angles of hip flexion, it was reported that the sarcomere length of the psoas major shortens from the extended position as the angle of hip flexion increases, with the optimal length at approximately 120∘ of hip flexion [17]. These reports predict that hip flexion torque is greater in deep hip flexion than in shallow hip flexion, contrary to the results of previous studies.
Therefore, the aim of this study is to measure isometric hip flexion torque at various hip joint angles in a stable supine position and to obtain foundational data for determining the optimal load pattern for developing a muscle training method using the hip flexion angle-torque characteristics.
Methods
Participants
Subjects were university students who indicated their willingness to cooperate in the study in response to a leaflet outlining the purpose and methods of the study and a verbal invitation to participate in the study. Exclusion criteria included (1) a history of osteoarticular or neurological disease or surgery and (2) daily strength training of lower extremities and trunk.
This study was conducted according to the Declaration of Helsinki after explaining fully the purpose of the study and the experimental methods to the subjects in advance, obtaining their written consent, and receiving approval from the Ethics Committee at Suzuka University of Medical Science (No. 384).
Experiment 1: Maximum isometric hip flexion torque without postural retention and compensatory motion
A total of 195 subjects (113 males and 82 females) participated in the study. The participants had a mean (mean
Measurement of muscle force
Schematic diagram of measurement setting of the right hip flexion muscle force. HDD, Hand-Held-Dynamometer.
Moment arm length was the distance from the estimated hip center to the HHD. HDD, Hand-Held-Dynamometer; ASIS, anterior superior iliac spine; HJC, hip joint center.
Since previous studies reported no difference in muscle strength between the dominant and non-dominant leg [18, 19, 20], the right lower limb was used as the measurement limb for all subjects in this study. The Hand-Held-Dynamometer (HHD)
The subjects were assigned randomly to start the measurement at 0∘ or 105∘, considering the effect of fatigue on the order of the measurement angles. The subjects were instructed to apply force for 5 sec after the start cue to reach maximum muscle strength and then gradually relax. The subjects were instructed to be aware of compensatory movements (trunk lateral bending, pelvic rotation, excessive lumbar kyphosis, and hip extension of the non-measured limb), and the measurement was stopped if any compensatory movement was visually apparent. Based on the findings of Sisto et al. [21] and Martins et al. [22], the interval between measurements was set to 90 s to recover the muscle strength exerted in each round.
The estimated hip joint center was 1/3 of the distance from the greater trochanter on a line connecting the greater trochanter and the anterior superior iliac spine. The distance from the estimated hip joint center to the HHD was measured and used as the torque arm length. Isometric hip flexion torque was calculated by multiplying the torque arm length by the average of the muscle forces measured 3times at the HHD, which was then normalized by height and weight (Fig. 2).
Statistical analysis
The Shapiro-Wilk test confirmed the normality of isometric hip flexion torque at each hip joint angle for both men and women. To verify whether there were differences in isometric hip flexion torque at different hip angles, a repeated measures two-way analysis of variance (ANOVA) was performed with sex and hip angle as independent variables and isometric hip flexion torque as the dependent variable. A multiple comparison test was conducted using the Bonferroni method if the main effect was found. A value of
Schematic diagram of the right hip flexion muscle force measurement setting. Setup A, Measurement setup that eliminates the postural retention function; Setup B, Measurement setup including posture retention function. HDD, Hand-Held-Dynamometer.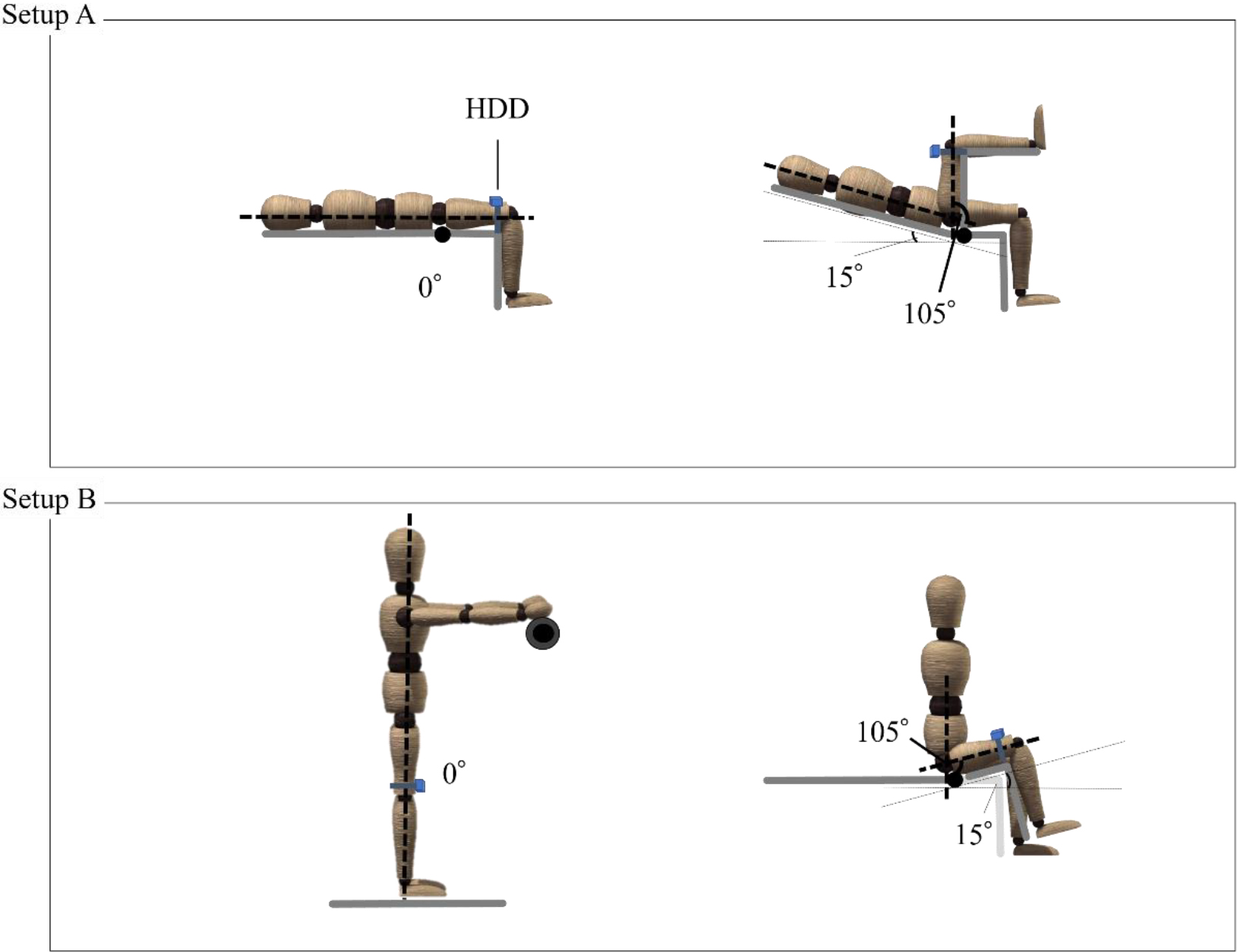
Thirty-three male participants were recruited for this study (mean age, 20.1
Measurement of muscle force
Relationship between hip flexion angle and torque in isometric contraction. *p < 0.01 vs. 0∘. †p < 0.01 vs. 105∘.
The right lower limb was used as the measurement limb for all subjects in this study. The HHD
The same method was used as in Experiment 1 (See 2.2.2 and Fig. 2).
Statistical analysis
The Shapiro-Wilk test confirmed the normality of isometric hip flexion torque at each hip angle for different measurement positions. To verify whether there were differences in isometric hip flexion torque between different hip angles, a two-way repeated measures ANOVA was performed with measurement posture and hip angle as independent variables and isometric hip flexion torque as the dependent variable. A multiple comparison test was conducted using the Bonferroni method if the main effect was found. A value of
Results
Maximum isometric hip flexion torque without postural retention and compensatory motion
Maximum isometric hip flexion torque for male and female (mean
Isometric hip flexion torque showed no interaction with sex or hip angle, with hip angle having the highest effect in both sexes and hip flexion of 0∘ having less flexion torque than all measured angles (
Maximal isometric torque change in hip flexion angle. Setup A, Measurement setup that eliminates the postural retention function; Setup B, Measurement setup including posture retention function. *p < 0.01 vs. setup B. †p < 0.01 vs. 0∘.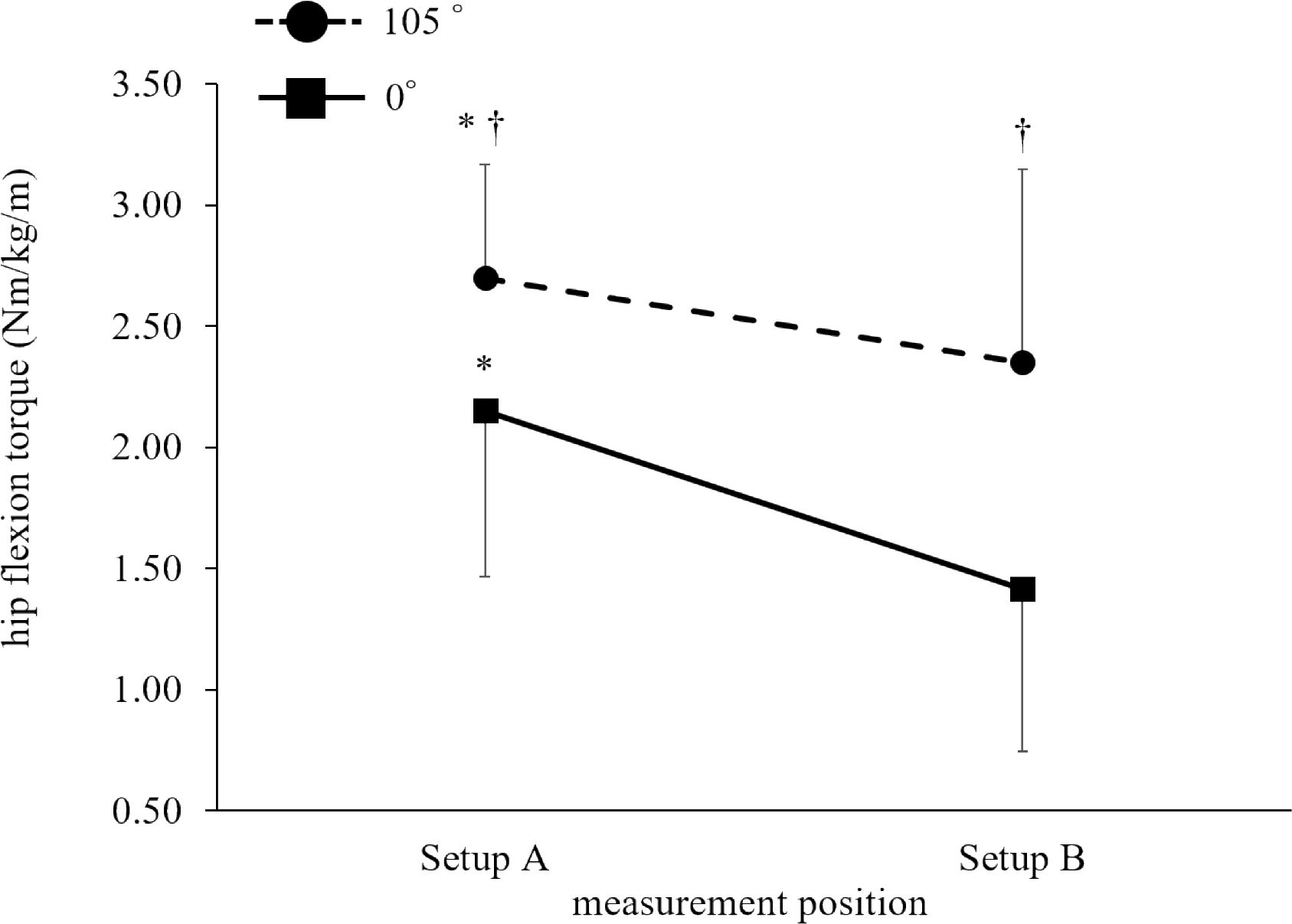
The isometric hip flexion torque (mean
Discussion
In Experiment 1, isometric hip flexion forces were measured at 0∘, 30∘, 60∘, 90∘, and 105∘ of hip flexion in the supine position, excluding the effects of postural retention function and compensatory movements. Our results showed that isometric hip flexion torque was lowest at 0∘ of hip flexion and highest at 105∘ of deep flexion. In Experiment 2, the maximum isometric hip flexion torque was greater at both 0∘ and 105∘ hip flexion in the supine position, which is not affected by the measurement posture retention function, than at 0∘ hip flexion in the standing position and 105∘ hip flexion in the edge of the bed sitting position. In addition, the maximum isometric hip flexion torque was greater at 105∘ than at 0∘ hip flexion, regardless of the measurement posture. These results are consistent with recent simulation studies using mathematical models and show that hip flexion torque has a characteristic of being maximal in the deep flexion position, which is different from previous studies [9, 10, 11, 12, 13] suggesting that hip flexion torque is decreased in the deep hip flexion position.
The differences between the results of this study and those of previous studies may be due to two factors. The first factor is the effect of the pelvic-femoral rhythm, in which pelvic and lumbar spine motions are linked to hip flexion. In hip flexion, both automatic and passive hip flexion movements are accompanied by backward tilting of the pelvis and flexion of the lumbar spine at an almost constant rate throughout the entire hip range of motion [23, 24]. In a previous study [14] that measured hip flexion torque in the supine position, the lumbar pelvis was fixed with a belt, which may have restricted the pelvis and lumbar spine motion associated with hip motion, resulting in inaccurate measurement of hip flexion torque. The second factor is the influence of the ability to stabilize the measurement posture on the exerted torque. In order to measure the maximum isometric exerted torque of a single joint, it is necessary to stabilize the posture and exclude the influence of other joints. Previous research [10, 11, 13] of hip flexion torque measured in the bed end-sitting position showed that the pelvis and lumbar spine alignment changes as the hip flexion angle increases, causing the hip to fall backward. This finding suggests that the maximum exerted torque was not measured because postural stability was not sufficiently maintained through adjustment of the back and seat. Furthermore, accurate hip flexion angle-torque should not be measured while side-lying [12] because the supporting lower limb and trunk are not fixed, and the posture is unstable. In this study, by using an examination table in which only the hip angle on the measurement side changes, we were able to measure the maximum isometric hip flexion torque without limiting the motion of the pelvis and lumbar spine thus, excluding the influence of maintaining posture and compensatory motion. The primary muscles that generate hip flexion torque are the iliopsoas, rectus femoris, sartorius, tensor fascia femoris, adductor longus, and pectineus muscles [25]. The long adductor muscle cannot generate flexion torque as the hip flexion torque arm decreases with increasing hip flexion angle and reverses to extension after 60∘ of hip flexion [25]. The rectus femoris has a reduced hip flexion torque arm in the hip extension range and a reduced exerted torque in the deep flexion range due to the shortening of muscle length. Regev et al. [17] performed muscle biopsies of the psoas major at 10∘ and 55∘ hip flexion and reported that the sarcomere length of the psoas major was 3.18
Based on the results of this study, we conclude that the training efficiency of hip flexor muscle strength training is high when the load is minimized in the initial stage of hip flexion and the maximum load torque pattern is applied in the deep flexion position. This loading pattern is simulated using a constant velocity exercise machine. However, this machine has a significant weakness in that the maximum load cannot be applied at the end of the range of motion because an acceleration phase and a deceleration phase are necessary. As a result, it is not beneficial for joint motions in which the peak torque is not in the center of the range of motion, such as hip flexion in this study. In addition, the effects of training posture and gravity make it challenging to achieve a loading pattern that maximizes loading torque in the deep hip flexion position using weights, elastic bands, and existing weight stack machines.
In the future, it is necessary to verify whether strength training based on the results of this study is helpful for people of all ages. For this purpose, it is desirable to develop a new training machine with a mechanism that can increase the load torque as the hip flexion angle increases.
Conclusions
The isometric hip flexion torque in healthy adults was shown to be minimum in the shallow hip flexion range and maximum in the deep hip flexion range, indicating a hip flexion angle-torque characteristic. Therefore, efficient strength training of the hip flexor muscle group is considered a hip flexion exercise in which the load increases gradually with increasing hip flexion angle.
Author contributions
CONCEPTION: Kazuhiro Ito.
PERFORMANCE OF WORK: Kazuhiro Ito, Koichi Saito and Kazuki Yamaguchi.
INTERPRETATION OR ANALYSIS OF DATA:Kazuhiro Ito, Etsuko Maeshima, Koichi Saito, Hiroya Koshiba, Takaaki Nakamata, Kazuki Yamaguchi, Ryota Maegawa and Yasuhiko Hatanaka.
PREPARATION OF THE MANUSCRIPT: Kazuhiro Ito, Etsuko Maeshima, Hiroya Koshiba and Yasuhiko Hatanaka.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Kazuhiro Ito, Etsuko Maeshima, Hiroya Koshiba, Ryota Maegawa and Yasuhiko Hatanaka.
SUPERVISION: Kazuhiro Ito, Etsuko Maeshima, Hiroya Koshiba and Yasuhiko Hatanaka.
Ethical approval
This study was conducted according to the Declaration of Helsinki after explaining fully the purpose of the study and the experimental methods to the subjects in advance, obtaining their written consent, and receiving approval from the Ethics Committee at Suzuka University of Medical Science (No. 384).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Acknowledgments
I would like to thank all the students who participated in this study.
Conflict of interest
The authors declare that they have no competing interests.