
Abstract
BACKGROUND:
Recovery of the isokinetic knee extensor strength on the operated side following anterior cruciate ligament (ACL) reconstruction is commonly calculated as a ratio with the value from the non-operated side serving as the denominator. However, the validity of the values of the non-operated side remains unclear.
OBJECTIVE:
This study aimed to determine the relationship between whole-body muscle mass and non-operated knee extensor strength after ACL reconstruction.
METHODS:
In 27 patients who underwent ACL reconstruction, muscle mass was measured using bioelectrical impedance analysis, and bilateral concentric knee extensor strength was measured using an isokinetic dynamometer at angular velocities of 60∘/s and 180∘/s. Correlation and single regression analyses were performed to examine the relationship between whole-body muscle mass and knee extensor strength.
RESULTS:
There was a strong to very strong positive association between whole-body muscle mass and non-operated knee extensor strength (60∘/s:
CONCLUSIONS:
Assessing both whole-body muscle mass and knee extensor strength may be used to determine whether muscle strength on the non-operated side is appropriate for the individual’s body composition.
Introduction
A reduction in knee extensor strength on the operated side is one of the primary problems that patients experience following anterior cruciate ligament (ACL) reconstruction [1, 2, 3]. The decreased knee extensor strength on the operated side relative to the non-operated side (asymmetry) is associated with asymmetry in daily activities such as walking [4], running [5], stair climbing [6], and sitting to standing [7]. Additionally, it affects sports activities such as single-leg hop [8] and landing [9]. This reduced knee extensor strength not only delays the return to sports but also contributes to poor outcomes such as subsequent injury and osteoarthritis of the knee [10, 11, 12]. Therefore, monitoring the degree of improvement and transition in knee extensor strength on the operated side is essential in postoperative rehabilitation.
Knee extensor strength on the operated side is typically evaluated using the limb symmetry index (LSI), calculated as (operated side/non-operated side)
However, LSI may overestimate the improvement in operated knee extensor strength because the denominator (i.e., the reference value) of LSI-non-operated knee extensor strength-declines over the postoperative course [16, 17]. Using both LSI and pre-injury muscle strength values to inform rehabilitation progression could be a solution; however, pre-injury data is usually unavailable in routine practice [18]. Although reference values for knee extensor strength after ACL reconstruction have been established [18], they are only representative of a specific population. The relationship between meeting reference values and outcomes, such as a second ACL injury, has not yet been investigated [18]. Given these uncertainties, the validity of using only the absolute value of the non-operated knee extensor strength as a reference for assessing improvement in the operated knee extensor strength remains questionable. Therefore, complementary indicators of LSI issues need to be examined.
As one possible solution, we propose an assessment within individual athletes based on physiological theory. Physiologically, muscle strength is proportional to the volume and size of the respective muscle [19, 20, 21]. Postoperatively, there has been a strong positive correlation (Spearman’s rho
Therefore, the purposes of this study were as follows: 1) to determine the relationship between non-operated knee extensor strength and whole-body muscle mass in patients following ACL reconstruction, and 2) to develop a regression equation for estimating non-operated knee extensor strength from whole-body muscle mass and confirm its accuracy. We hypothesized that a strong positive correlation between non-operated knee extensor strength and whole-body muscle mass would be present, and the regression equations to estimate non-operated knee extensor strength from whole-body muscle mass would be accurate.
Methods
Participants
Patients who underwent primary ACL reconstruction between March 2018 and November 2021 were included if they met the following criteria: (1) age of 16-45 years at the time of measurement [24, 25], (2) participation in sports with a modified Tegner activity scale score
Procedure
A cross-sectional single-center study was conducted. Demographic and surgical data were obtained from medical records. Demographic data included age, sex, and activity level, which were measured using a modified Tegner activity scale [23]. Surgical data included graft type, presence of meniscal repair, and number of months since the surgery. The participants’ knee extensor strength and whole-body muscle mass were measured on the same day. The study was reviewed and approved by the review board of Tokyo Medical and Dental University (approval number: M2019-158) and was performed in accordance with the ethical standards of the Declaration of Helsinki. All participants provided written informed consent prior to participation.
Postoperative rehabilitation
The postoperative rehabilitation protocol was based on a previous study [27]. Crutches and a straight-position knee-joint immobilizer (Knee brace, ALCARE Co., Ltd., Tokyo, Japan) were used and gradually phased out 4-w post-ACL reconstruction. The patients who underwent repair of the middle-posterior segment of the meniscus were prohibited from bending the knee
Whole-body muscle mass measurement
Whole-body muscle mass was measured using a dual-frequency body composition scale (DC-430A; Tanita, Tokyo, Japan). Body composition scales using BIA can accurately measure whole-body muscle mass in clinical settings [29]. BIA estimates body composition by applying harmless low-frequency electric currents through the body [30]. DC-430A is a dual-frequency (6.25 and 50 kHz) BIA device that uses reactance technology [31]. The body composition outcomes derived by this system highly correlate with those obtained by dual-energy X-ray absorptiometry (DXA) [32, 33], which is considered the gold-standard method for body composition assessment.
Body composition measurements were performed before the muscle strength measurements, with participants dressed in standard sports clothes without footwear. To ensure participants maintained normal hydration status, they were assessed based on the following criteria: having refrained from consuming any food for at least 2 hours prior to the measurement, avoiding excessive intake of caffeine or alcohol for at least 12 hours before the measurement, and urination and defecation having been completed before the measurement [29, 30].
Knee extensor strength measurement
Knee extensor strength was assessed using an isokinetic dynamometer, with isokinetic knee extensor strength measured at angular velocities of 60∘/s and 180∘/s (Ext 60 and Ext 180, respectively) according to previous studies [34, 35, 36]. The muscle contraction type utilized was concentric, which is commonly employed to determine return to sport after ACL reconstruction [15, 37]. In this study, knee extensor strength of both the non-operated and operated sides were measured for comparison. Before measurement, participants were checked for the absence of excessive muscle fatigue, and a 5-min warm-up was performed with unloaded ergometer pedaling before the test. Participants were positioned with their hips in 90∘ of flexion, their backs supported, and their test limbs securely strapped into an isokinetic dynamometer. They performed knee extensions within a set range of motion of 0-100∘ [37]. The axis of knee rotation was aligned with the shaft of the dynamometer, and the bottom end of the resistance pad was placed directly above the medial tubercle [38]. Gravity compensation is recommended to maintain the lever arm as horizontal as possible, while avoiding the extension of the muscle antagonist pair. Therefore, the gravity correction angle was set at either 10∘ or 20∘ of knee flexion, while ensuring the participant’s hamstring was not excessively stretched [39]. All participants performed at least two practice repetitions to become familiar with the task followed by five maximum repetitions. Participants were then verbally encouraged to give their maximum effort. The inter-velocity rest period was 1 min, and the inter-side rest period was 5-min. Peak torque was expressed in Newton meters (Nm). High intra-rater and inter-rater reliability for this measurement have been reported previously [40, 41].
Characteristics of the participants (
27)
Characteristics of the participants (
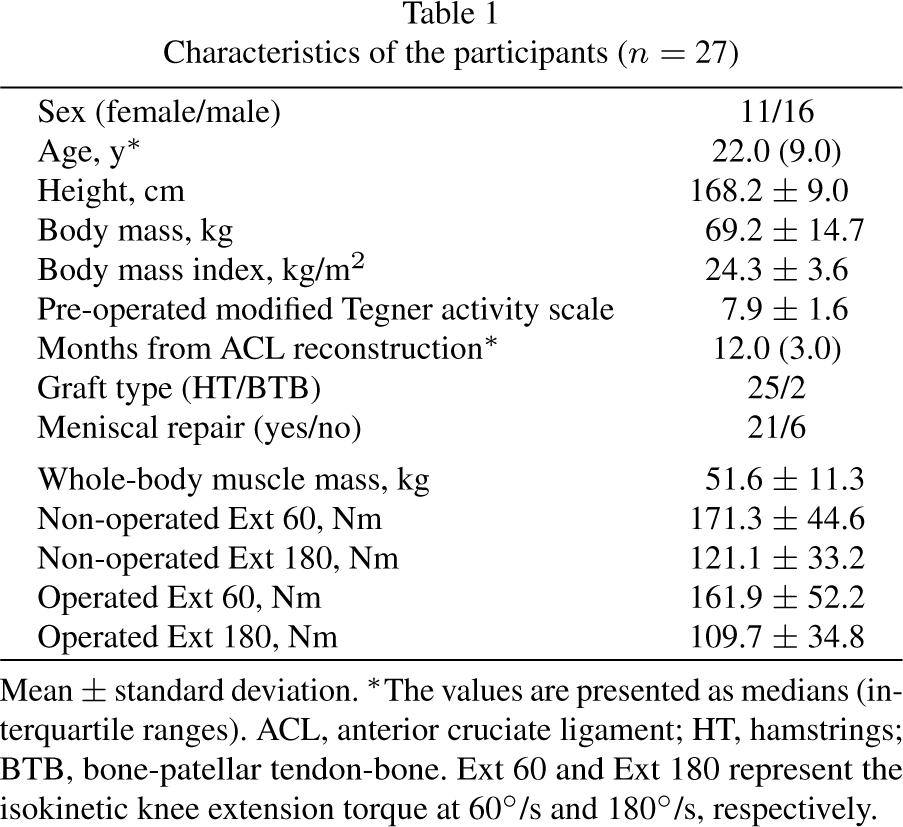
Mean
The Shapiro-Wilk normality test was performed, and histograms were checked to determine the data distribution of each variable. The mean and standard deviation were calculated for variables that were normally distributed, and the median (interquartile range) was calculated for variables that were abnormally distributed.
First, bivariate correlation analyses were performed to examine simple linear correlations (Pearson’s
Second, a simple regression analysis was performed with non-operated knee extensor strength as the dependent variable and whole-body muscle mass as the independent variable. A residual plot was used to validate the model [43].
Considering the potential influence of sex on the results of this study, additional analyses were performed. These included: correlation analysis between whole-body muscle mass and non-operated knee extensor strength by sex (Pearson’s r), and comparisons of knee extensor strength between sexes (using an unpaired
The alpha (
Results
A total of 27 participants (11 females and 16 males) with a median age of 22.0 years (interquartile range: 9.0), a median duration since ACL reconstruction of 12.0 months (interquartile range: 3.0), and a mean pre-operated modified Tegner activity scale of 7.9
The correlation between non-operated knee extensor strength and whole-body muscle mass is shown in Fig. 1. A strong to very strong positive correlation existed between whole-body muscle mass and non-operated knee extensor strength (60∘/s:
Sinple regression for non-operated knee extensor strength
Sinple regression for non-operated knee extensor strength
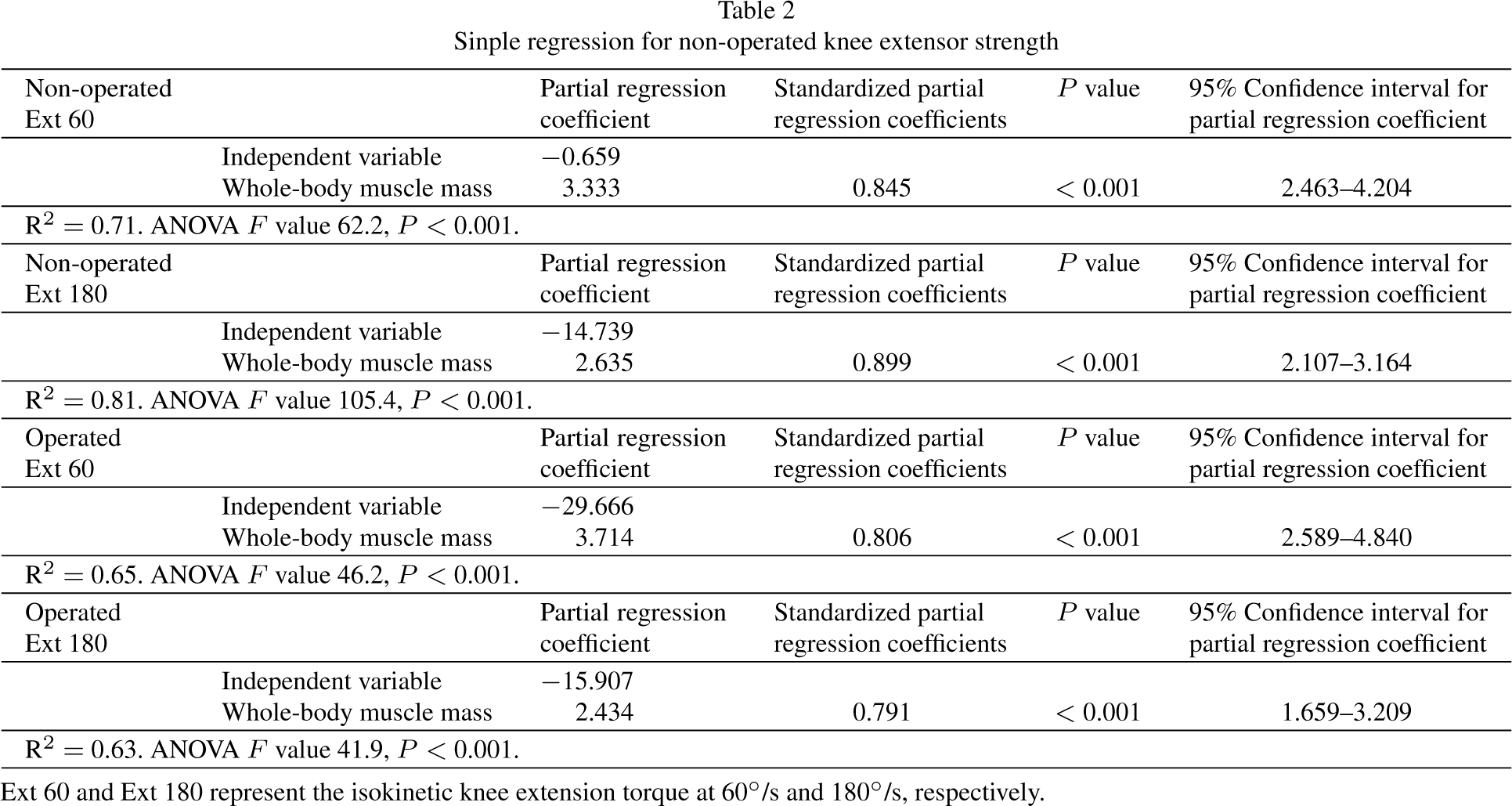
Ext 60 and Ext 180 represent the isokinetic knee extension torque at 60∘/s and 180∘/s, respectively.
The results of the univariate regression analysis are presented in Table 2. On the non-operated side, the predicted rates of Ext 60 and Ext 180 from whole-body muscle mass were 71% (R2
[Ext 60] Predicted non-operated knee extensor strength [Ext 180] Predicted non-operated knee extensor strength [Ext 60] Predicted operated knee extensor strength [Ext 180] Predicted operated knee extensor strength
Residual plots of the simple regression analysis are shown in Fig. 2. All residual plots were almost evenly distributed in relation to zero.
The results of the correlation analysis by sex showed a strong positive correlation between whole-body muscle mass and non-operated knee extensor strength in female individuals (60∘/s:
Comparison of non-operated knee extensor strength by sex

Scatter plots of the relationship between knee extensor strength and whole-body muscle mass. Ext 60 and Ext 180 represent the isokinetic knee extension torque at 60∘/s and 180∘/s, respectively. CI, confidence interval.
Unpaired
Multiple regression for non-operated knee extensor strength
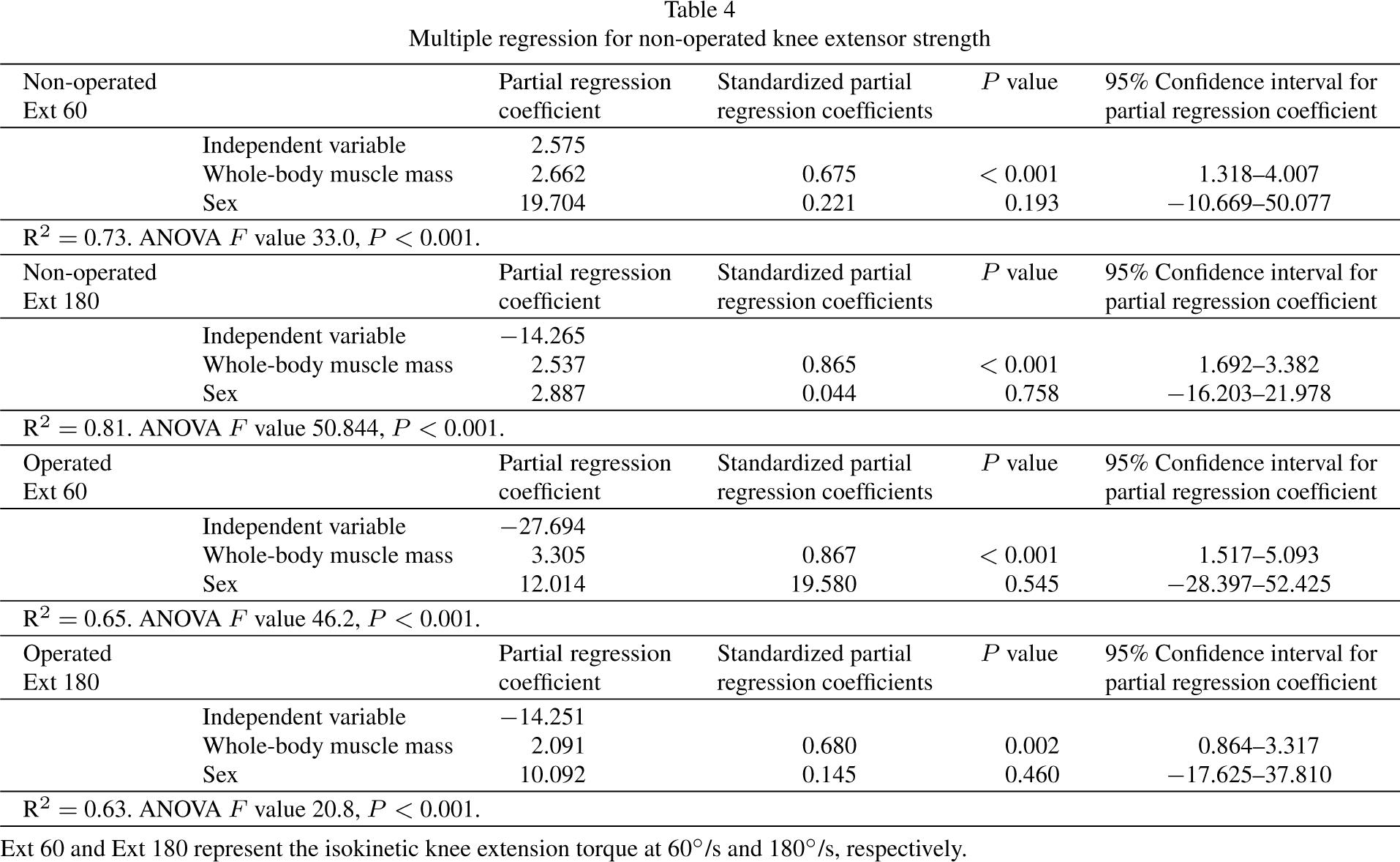
Ext 60 and Ext 180 represent the isokinetic knee extension torque at 60∘/s and 180∘/s, respectively.
Residual plots of the estimated and actual knee extensor strength of the non-operated side. SD, standard deviation.
Multiple regression analysis showed that sex was not a significant independent variable (Table 4). The coefficient of determination in the multiple regression analysis including sex as an independent variable was similar to that in the single regression analysis for whole-body muscle mass and non-operated knee extensor strength (Tables 2, 4).
The primary findings of this study supported our hypothesis: a strong positive correlation between whole-body muscle mass and non-operated knee extensor strength was confirmed, and the regression equation for predicting non-operated knee extensor strength from whole-body muscle mass had a good level of accuracy.
A strong to very strong positive correlation was found between the knee extensor strength of the non-operated side and whole-body muscle mass. Physiologically, muscle strength is proportional to muscle volume and cross-sectional area [19, 20, 21]; therefore, the results of this study can be theoretically explained. Our results support these previous studies, showing that the greater the whole-body muscle mass, the greater the non-operated knee extensor strength.
The coefficient of determination of the regression equation for estimating knee extensor strength of the non-operated side from whole-body muscle mass was high (R2
The regression equation formulated in this study shows that the predicted value of knee extensor strength of the non-operated side can be calculated with acceptable accuracy using whole-body muscle mass measured through BIA. By comparing the predicted values with the actual values of knee extensor strength of the non-operated side, it was possible to determine whether a patient’s knee extensor strength of the non-operated side is suitable for their whole-body muscle mass. BIA can simply and accurately measure whole-body muscle mass [29] without the costs (time, financial, and expertise) of other methods such as DXA and magnetic resonance imaging [30]. We have presented basic information that can be applied in rehabilitation settings.
In the present study, the predicted value of knee extensor strength of the operative side based on whole-body muscle mass (R2
Our study showed a strong correlation between whole-body muscle mass and non-operated knee extensor strength. However, a cross-sectional study design was employed, which prevented analyses of the reasons for the change in knee extensor strength of the non-operated side. In the future, longitudinal studies should be performed to determine the association between chronic postoperative changes in whole-body muscle mass and knee extensor strength of the non-operated side. This would provide insight into the reasons for changes in knee extensor strength of the non-operated side, based on changes in whole-body muscle mass, and provide supporting evidence that whole-body muscle mass should be measured in conjunction with knee extensor strength.
Correlation analysis by sex showed a statistically significant positive correlation for both sexes, but the effect size was lower than the corresponding for all participants. This trend was confirmed irrespective of sex, suggesting that the observed reduction in power was attributed to reduced sample size rather than a sex effect, although the reasons for this are unclear in this study. Unpaired
It is important to note that BIA is not a substitute for knee extensor strength assessment. The results of this study should be used to assess whether the absolute value of non-operated knee extensor strength is a valid reference for the muscle strength that an individual can perform. The evaluation of knee extensor strength after ACL reconstruction is commonly performed by using LSI, where the muscle strength of the operated side is calculated relative to that of the non-operated side, which serves as the denominator in the equation and acts as the reference for comparison. However, there is currently no established method to ascertain whether the value of knee extensor strength on the non-operated side is adequate. Traditionally, the weight ratio of knee extensor strength is calculated as an indicator of strength; however, normalization by body weight is less accurate because it includes fat mass [22]. Based on the results of this study, it could be feasible to calculate the estimated knee extensor strength according to the whole-body muscle mass of each patient. This estimation could then be compared with the measured knee extensor strength on the non-operated side to evaluate whether the patient has achieved muscle strength proportional to their body size. In addition to the LSI meeting a specific value (e.g.,
The present study has some limitations. Its results are based on the assumption that the participants were able to achieve their maximum strength during knee extension of the non-operated side. We addressed this limitation by pre-measurement practice and by allowing a rest period between measurements, but this may not be sufficient. To objectively address this issue, it might have been necessary to evaluate both eccentric and concentric contractions and confirm the eccentric to concentric strength ratio based on physiological characteristics [50]. The data derived from BIA used to calculate whole-body muscle mass included smooth muscle mass; thus, skeletal muscle mass and the mass of the extensor muscles of the knee alone are unknown. Therefore, the regression equation we presented may only be applicable to the type of dual-frequency body composition analyzer used in this study. In the future, the validity of this study should be further strengthened by examining the relationship between segmental muscle mass in the lower extremity [51] and knee extensor strength. Factors affecting muscle strength in this study, such as muscle fiber type and nervous system function, are unknown. In addition, participant variables such as sex, age, and sports discipline were not considered in the analysis. In future studies, the sample size should be increased, and the accuracy of the estimations derived from the regression equation should be improved by performing subgroup analysis and multivariate analysis based on participants’ sex, age, and sports discipline.
Conclusion
This study analyzed the relationship between whole-body muscle mass and non-operated knee extensor strength in patients approximately 12 months after ACL reconstruction surgery. Non-operated knee extensor strength may be estimated with acceptable accuracy from the whole-body muscle mass in patients following ACL reconstruction. Integrating assessments of both whole-body muscle mass and knee extensor strength could help assess whether the strength on the non-operated side aligns with an individual’s body mass.
Funding
This work was supported by the Japanese Physical Therapy Association (JPTA1-B17).
Ethical considerations
The study was reviewed and approved by the review board of Tokyo Medical and Dental University approval number: M2019-158, approval date: October 8th, 2019). All participants provided a written informed consent prior to participation.
Author contributions
CONCEPTION: SO.
PERFORMANCE OF WORK: SO, JA, KH, TO, SM.
INTERPRETATION OR ANALYSIS OF DATA: SO, JA, KH, TO, SM.
PREPARATION OF THE MANUSCRIPT: SO, JA, KH, TO, SM.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: JA, HK, KY.
SUPERVISION: HK, KY.
Footnotes
Acknowledgments
We would like to thank Editage (
Conflict of interest
The authors have no conflicts of interest to report.