
Abstract
BACKGROUND:
It has been demonstrated that maximum isometric muscle moment can surpass maximum eccentric muscle moment at individually adjusted joint angles in men. However, no information about these muscle mechanics is available for women.
OBJECTIVE:
To examine the maximum muscle moment hierarchy with equal conditions in women.
METHODS:
Maximum voluntary concentric, eccentric, and isometric muscle moments of ankle, knee, and hip flexors and extensors as well as hip adductors and abductors were tested in eighteen young women. The sequence of muscle group testing was the same for all subjects, and the sequence of contraction types was randomized. All dynamic contractions were performed at 60∘/s. Peak moment angle of concentric contractions was applied for isometric moment testing. A repeated measures ANOVA with posthoc Bonferroni correction was used to compare means between contraction types.
RESULTS:
Differences in maximum moment mean values between the three contraction types were apparent for all muscle groups (
CONCLUSION:
Significant differences in maximum lower body muscle moments exist between concentric, eccentric, and isometric contractions in women. Compared to previous research for men there appears to be a sex-specific contraction type hierarchy with women exhibiting superior ability to generate higher eccentric muscle moment relative to other contraction types. These results should be considered when designing contractiontype specific intervention programs.
Introduction
The musculoskeletal system produces movement through muscle contraction which gets translated over tendons to bones functioning as levers [1]. However, in everyday life different movements such as getting up from a chair, descending stairs, or holding an object require different muscle contractions with specific muscle mechanics [2].
Traditionally, shortening and lengthening muscle contractions are referred to as concentric and eccentric contractions respectively. Muscle contractions in a static position are characterized by a constant muscle length and are known as isometric contractions [3]. In the scientific literature there is a well-established contraction type hierarchy regarding the magnitude of moment these contraction types can produce. Concentric contractions exhibit the smallest amount of muscle moment compared to isometric contractions and eccentric contraction [4, 5, 6, 7]. Eccentric contractions typically exceed the moment of isometric contractions but the difference varies throughout the literature and depends on multiple parameters including the tested muscle group, joint angle, and contraction speed. For example faster contraction speeds and joint angles at a disadvantageous muscle length can lead to lower eccentric and isometric muscle moment, respectively [6, 7, 8].
Recently, we demonstrated that muscle moment generated during isometric contractions can exceed the moment generated during eccentric contractions in lower limb muscles when individually optimized joint angles are used for isometric contractions [9]. However, a key limitation of this novel protocol was that it provided data regarding men only, and therefore equivalent data in women is absent. Indeed in this regard previous examinations rarely provided considerations for sexspecific interactions in muscle mechanics [7, 8, 10] which might be due to the fact that women are generally under-represented in sports and exercise medicine research [11, 12]. The need for a sex-specific analysis of muscle contraction characteristics is supported by a number of studies that have shown that women and men are not only different in the anthropometry, biomechanics and injury mechanisms, but also respond differently to high-intensity eccentric [13] and isometric resistance exercise [14]. While it is believed that muscle mass, blood flow, fiber types, hormonal status could play a considerable role for these observations the underlying mechanism are still mostly unknown [15].
Another research deficit is that previous examinations did not compare all three contraction types often focusing only on the comparison between concentric and eccentric contractions and providing no information about isometric moment [4, 5]. This might be attributed to the methodological challenges of choosing an isometric test angle appropriate for the research question. Previous research that attempted to find the joint angle at which peak muscle moment occurred used a sequence of multiple joint angles without validation that the overall best joint angle was found [7, 10, 16, 17]. While it can be hypothesized that the application of an optimized isometric angle will lead to higher isometric muscle moments it remains unclear how this will affect the contraction type moment hierarchy in women, especially considering evidence that women exert much larger eccentric to concentric moment ratios compared to men [5]. Therefore, the question stands if women will present similar moment relations between contraction types to those previously demonstrated in men [9] or whether each sex has a unique contraction type moment profile.
To close the aforementioned research gaps the aim of this study is to examine the maximum voluntary lower body muscle moment hierarchy of all three contraction types in women using optimal joint angles for isometric moment assessment.
Methods
Participants
Eighteen women with an age of 23.1
Testing procedures
All assessments were performed in one single testing session by a trained member in isokinetic strength testing of the research team in the biomechanics laboratory. A counterbalanced crossover design was applied to mitigate possible effects of fatigue, test familiarity, and neuronal excitability due to the testing sequence. Since optimal joint angles for peak isometric contraction vary between individuals, the approach of Stotz et al. (2022) to choose an individualized isometric test angle derived from peak moment angle from concentric contraction was adapted. The participants could therefore be randomized in only three test groups because concentric testing needed to be performed before isometric trials. Participants were therefore randomly assigned to three test groups to cover the three possible testing sequences. The contraction type sequence for group 1 was concentric, isometric, and eccentric. Group 2 started concentrically, followed by eccentric and isometric contractions. Group 3 was first tested eccentrically followed by concentric and isometric contraction types.
General subject information
At first basic information including age, main sports activity, weekly training volume in hours, previous injuries, and leg dominance (preference leg to kick a ball) was obtained with a self-designed questionnaire [18].
Anthropometrical assessment
In the next part of the assessment anthropometrical parameters including height, weight, skeletal muscle mass fat mass, and body fat percentage were obtained with a stadiometer and a bioimpedance scale InBody 720 (JP Global Markets GmbH, Eschborn, Germany), respectively.
Muscle moment assessment
Muscle moments of all tested muscle groups and all contraction types were measured with the Isomed 2000 isokinetic dynamometer (Isomed 2000®, D&R Ferstl GmbH, Hemau, Germany). The muscle group test sequence was identical for all subjects starting with ankle plantarflexion and dorsiflexion, followed by knee flexion and extension, continuing with hip abduction and adduction and ending with hip flexion and extension. Dynamic contraction types were assessed with an angular speed of 60∘ per second with three repetitions per trial. The test duration to produce maximum isometric contraction was set at three seconds. The moments of concentric and isometric contractions were measured across two trials. Since there is a possible eccentric activation deficit in individuals not familiar with these contractions an additional test trial was implemented for eccentric moment assessment to provide a third opportunity to display the complete eccentric moment potential. The highest peak moment reached in these two and three trials respectively was used for the statistical analysis. The rest time between test trials was 90 s and participants remained sitting on the dynamometer. Longer rest periods of approximately 5 min in which participants could move around the test room were available while the investigator changed the dynamometer setting for the next muscle group. The limb weight was measured and zeroized by the dynamometer to eliminate its influence on moment values.
shows the test positions, pivot points, ranges of motion, and adapter positions for all muscle group settings
shows the test positions, pivot points, ranges of motion, and adapter positions for all muscle group settings

For each muscle group test, the dynamometer was adjusted to the anthropometry (hip dimensions, femur, and lower leg length) of the subject. Also, for each test setting the respective adapter (foot platform, lever with pad, and straps) was used. To prevent evasive movements and to maintain the proper testing position the subjects were fixed with straps, belts, and a pad on the lower limbs, pelvis, and shoulders. The pivot points (Table 1) of the tested joints were synchronized with the pivot point of the dynamometer. Overall, sufficient to good reliability was reported for isokinetic ankle plantarflexion, dorsiflexion, knee flexion, knee extension, hip abduction, hip adduction, hip flexion and hip extension [19, 20, 21, 22]. After all preparatory actions were finished participants worked through a familiarization and warmup phase. For the concentric contraction type the joint was moved through the full test range of motion and a transition between flexion and extension was practiced. Participants were notified that the dynamometer would move at a constant angular speed and that they must apply maximum force throughout all positions and all test repetitions. Following this, participants were instructed to increase the amount of force to execute the movement while staying on a submaximal level. Lastly, the test starting position, the movement sequence (starting with flexion or extension), and the countdown of the dynamometer were explained.
Study design including randomisation and testing sequences.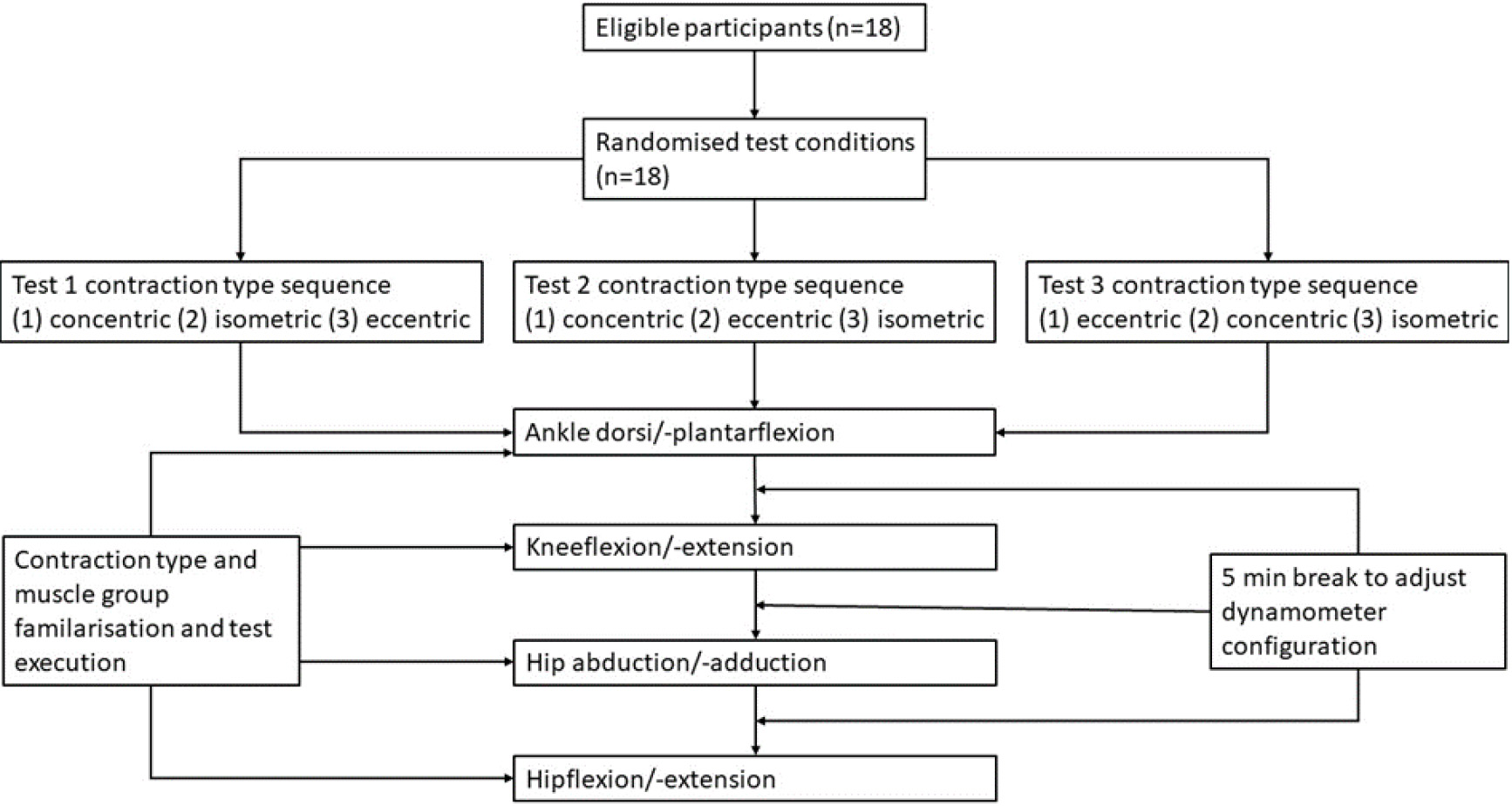
For the isometric testing the angle derived from the peak moment angle from concentric contraction was adapted and participants tested out applying force against the immovable adapter. They were asked to perform submaximal repetitions with increasing force, and to track the force curve on the display. For the eccentric contraction type the tested joint was also moved through the full range of motion. Participants were familiarized with the concept of working against the movement direction of the dynamometer. Again, the transition between flexion and extension was practiced so that the participants changed the direction of their force output simultaneously with the direction change of the dynamometer. Only once multiple repetitions of smooth transition were executed the participants were then asked to submaximally increase their force output to prepare their central nervous system for the maximum voluntary contractions. After every familiarization and warmup phase participants rested two minutes to ensure that maximum voluntary testing was performed with no pre-exhaustion. The study design and testing sequences are illustrated in Fig. 1.
Statistical analyses were performed with JASP (JASP Team (2020), version 0.164.9, JASP Team 2020, Amsterdam, The Netherlands). A one-way analysis of variance for repeated measures was used to compare the maximum force between contraction types. When a level of significance (
Results
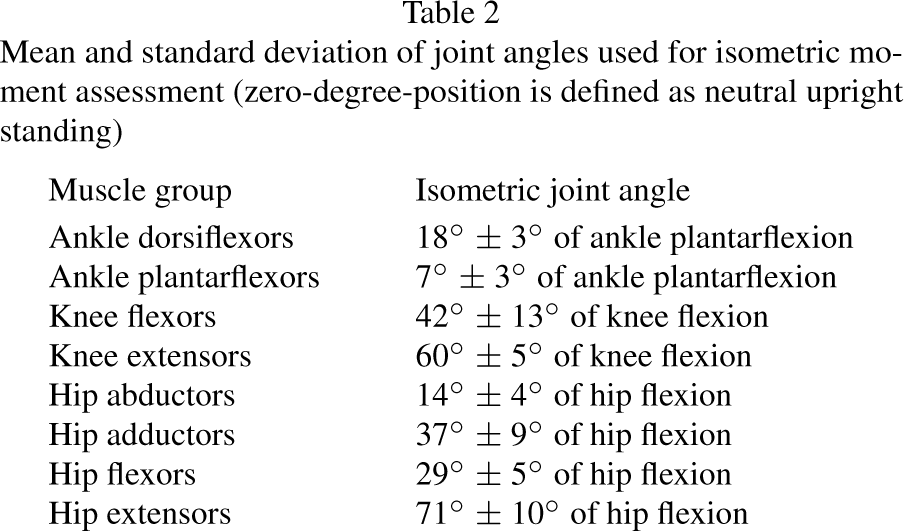
Figure 2 shows the maximum moment mean values and 95% confidence interval for all muscle groups and all three contraction types. Table 2 presents mean values and standard deviations of peak moment joint angles from concentric contractions that were used for isometric moment assessments.
Mean and standard deviation of joint angles used for isometric moment assessment (zero-degree-position is defined as neutral upright standing)
Mean and standard deviation of joint angles used for isometric moment assessment (zero-degree-position is defined as neutral upright standing)
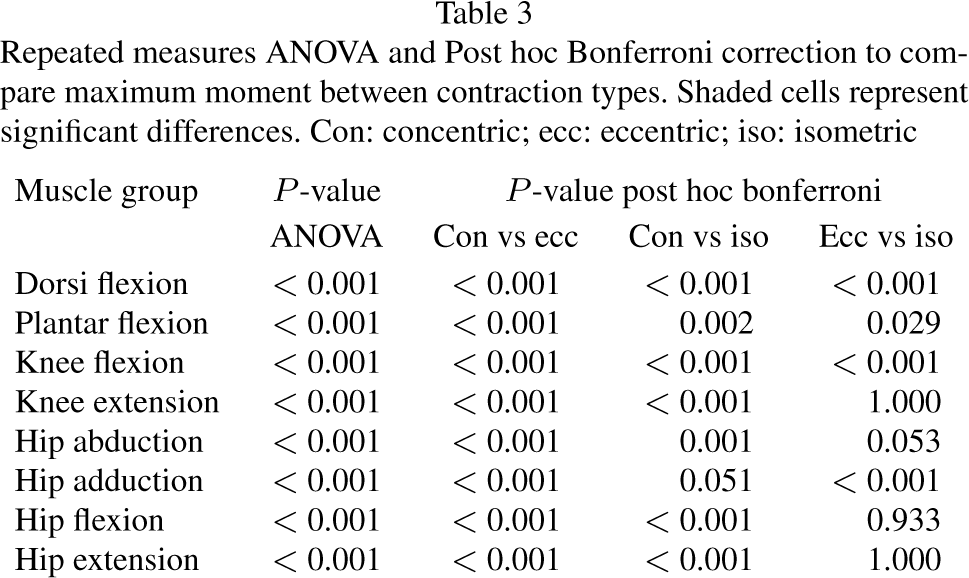
Repeated measures ANOVA and Post hoc Bonferroni correction to compare maximum moment between contraction types. Shaded cells represent significant differences. Con: concentric; ecc: eccentric; iso: isometric
Means and 95% confidence intervals of maximum muscle moment of all contraction types in all muscle groups (*indicates significant differences between concentric and eccentric muscle moment, #indicate significant differences between concentric and isometric muscle moment, and ‡indicates significant differences between eccentric and isometric muscle moment).
The Repeated Measures ANOVA in Table 3 presented significant differences in maximum moment mean values between the three contraction types for all muscle groups (
This study aimed to elucidate the maximum voluntary muscle moment hierarchy of concentric, eccentric, and isometric contraction in women using optimized joint angles for the isometric moment assessment. Our results show that the magnitude of muscle moment differed between the three contraction types in all lower body muscle groups. As observed in many previous reports concerning contraction type comparisons concentric muscle moment was consistently significantly the weakest contraction type compared to isometric and especially eccentric contractions [5, 7, 10, 23, 24, 25]. Eccentric muscle moment significantly exceeded isometric muscle moment in four out of the eight tested muscle groups. These results differ from the contraction type hierarchy we showed previously in men [9] where isometric contractions reached overall the highest moment values. Summarizing the differences in results between contraction types for both sexes we conclude that the most important finding of our study is that there may be a sexspecific contraction type hierarchy in lower limb muscles. Specifically, our results indicate that that women exhibit a far superior ability to generate higher eccentric muscle moment relative to the other contraction types compared to men while men have a vastly stronger ability to generate higher isometric forces. However, these muscle mechanics depend on the tested lower limb muscle group and it seems that a similar trend is apparent for both sexes. For instance, in knee extensors, hip flexors and extensors women showed relatively high isometric moments leading to no significant moment differences compared to eccentric muscle actions. This was also true for men because in those muscle groups isometric moments were exceptionally high in comparison to the other contraction types [9]. There were also notable similarities between both studies in terms of average joint angles at which peak moment occurred with the notable exception of the hip adductors (25∘ for men and 37∘ for women) [9]. Therefore, we conclude that that differences in sex-specific moment arrangements between contraction types may not be attributed to differences in peak moment joint angles used for isometric contractions.
Sexspecific differences in moment production during different contraction types were recently reported in a review by Nuzzo et al. 2023 [4], however, the authors focused solely on the ratio between eccentric to concentric moment, and no comprehensive information is available for isometric data. This is likely due to very few studies measuring all three contraction types, combined with the difficulty of providing a valid comparison of isometric moment between studies given differences in methods and the sensitivity to factors such as joint angle. Nuzzo et al. 2023 [4] suspected that the eccentric to concentric moment ratio differences may be attributed to the higher concentric contraction capabilities of men compared to women. The authors argued that since men participate in muscle-strengthening activities more regularly than women [26] the usage of constant load (which represents a higher percentage of the concentric and eccentric 1-RM) leads to greater concentric than eccentric strength increases. However, the suggested explanation was not confirmed with valid evidence. It is also possible that other training experience modalities e.g. the type of strength training (strength endurance, maximum strength, power training) or training equipment (free weights, machines, bodyweight) could have influenced the contraction type results [27]. Therefore, further research is necessary to examine how strength training experience influences the contraction type ratios of men and women.
It is also unclear how other aspects of morphological differences between men and women affect the unique moment production capabilities of the various contraction types, but there are many differences in neuromuscular characteristics which are candidate contributors. For example, it has been reported that men and women have different compositions of muscle fibers for selected muscle groups [28, 29]. It is also known that men present larger muscle size in terms of thickness and length [30, 31], as well as unique pennation angle of the muscles [32]. Differences in tendon properties including stiffness, fascicle length and viscoelasticity are also reported to differ between men and women [33, 34, 35, 36]. Similarly, differences in neuromuscular function between men and women have not been studied regarding their influence on contraction typespecific moment production [37]. Combined, we speculate that these factors may at least partially underpin the sex-specific findings of our studies.
Although this was not an intervention study seeking to improve force production capabilities important practical implications can be drawn from the findings of this study. Athletes aiming to increase their muscle strength through intervention programs using specific contraction types, for example eccentric training [38] should refrain from using arbitrary and standardized moment ratios to select training intensities. We suggest performing preliminary strength testing to properly assess contraction typespecific strength capabilities and select the training load according to the results and in consideration of their sex, the targeted contraction speed, applied joint angle and selected muscle group.
Limitations
While our findings provide further insights about the contraction typespecific muscle mechanics in women a few limitations and further research questions need to be addressed. Despite performing a standardized familiarization phase to ensure appropriate test execution for eccentric contractions and increasing the number of test trials (compared to isometric and eccentric contractions) for this contraction type, we cannot guarantee that potential eccentric activations deficits were completely eliminated [39]. A separate familiarization session focusing on isokinetic eccentric contractions might have been more appropriate to mitigate practice-based improvement [40]. However, there is no consensus about the familiarization modalities in isokinetic testing with some research suggesting one familiarization session but other research indicating that one single testing session produces similar and sufficiently reliable test results [40, 41, 42]. Only one angular speed was used for dynamic muscle contractions and the corresponding peak moment angle was applied for isometric contractions. However, it is unclear if peak moment angles derived from concentric contractions with slower angular velocities would be significantly different across all tested muscle groups and would fit more appropriately for isometric testing. Also, the moment magnitude would change with different contraction speeds which therefore would influence the moment hierarchy [4, 43]. However, it must be noted that it is not possible to perform one single study that accounts for all testing variables, as central and local fatigue limits the total amount of possible test trials even with longer rest periods. Additionally, testing the same subjects over multiple sessions may not be recommended because additional exposure to the maximal strength test itself can influence the results due to familiarization and the rapid acquisition of the skill of producing force without changes in the underlying physiology [44, 45]. Further, the testing procedure was carried out only for the lower limbs of young healthy active women. Therefore, further research is necessary to examine the moment hierarchy in other muscle groups including upper body and trunk muscles, particularly given the variations in sex-based strength differences between the lower limbs and upper limbs [26, 46]. Finally, with advanced age of life muscle strength and function changes [47] and therefore the muscle contraction moment hierarchy with all the aforementioned influencing parameters also needs to be examined with older women and men.
Conclusion
There are significant differences in maximum lower body muscle moments between concentric, eccentric, and isometric contractions in women. Concentric muscle moment produces lower muscle moment compared to isometric and eccentric contractions. Eccentric contractions surpassed isometric contraction moments for plantar flexion, dorsi flexion, knee flexion and hip adduction. Compared to previous reports for men [9] there seems to be a sex-specific contraction type hierarchy. Contraction typespecific intervention programs should consider that sex, the targeted muscle group, the contraction speed and joint angles might influence the strength capabilities of all three contraction types.
Author contributions
CONCEPTION: Andreas Stotz.
PERFORMANCE OF WORK: Steven Richter.
INTERPRETATION OR ANALYSIS OF DATA: Andreas Stotz, Joel Mason, Astrid Zech.
PREPARATION OF THE MANUSCRIPT: Andreas Stotz, Joel Mason, Astrid Zech.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Joel Mason, Astrid Zech.
SUPERVISION: Astrid Zech.
Ethical considerations
Every participant received a study information sheet and provided informed consent. Ethical approval has been obtained by the Ethical Commission of the local ethics committee (protocol number: FSV 20/002, 31.01.2020).
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.