
Abstract
BACKGROUND:
The gluteus medius (GM) plays an important role in stabilizing the knee and preventing injury.
OBJECTIVE:
This study aimed to determine the immediate effects of weight-bearing gluteus medius exercises on lower-extremity muscle function and dynamic knee valgus.
METHODS:
Eighteen healthy adults (nine each of both sexes) performed three types of weight-bearing gluteus medius exercises (standing, mini-squat, and dead-lift), and a range of kinematic variables were tested in triplicate. Weight-supporting GM exercise consisted of three sets of 15 repetitions of the lateral band walk. The Y-balance test (YBT) and vertical single-leg jump were used as indicators of muscle function in the lower limbs. We used a video analyzer to film the dynamic knee valgus and performed a YBT for the supporting leg and landing leg following a jump.
RESULTS:
The height of the single-leg vertical jump and the posterolateral and total YBT scores were significantly higher in the dead-lift posture than in the standing and mini-squat postures. Motion analysis of the dead-lifts revealed high hip flexion on the supporting leg in the posterolateral direction, as determined by the YBT, with low levels of internal hip rotation on the landing leg during the one-leg vertical jump.
CONCLUSION:
As an immediate effect of gluteus medius exercise, the dead-lift posture facilitated single-leg vertical jump, posterolateral balance, and reduced dynamic knee valgus.
Introduction
Lower extremity injuries account for a large proportion of sports-related injuries, including knee injuries, anterior cruciate ligament (ACL) rupture, patellofemoral pain syndrome (PFPS), and patellar tendinopathy injuries [1, 2, 3]. Particularly, serious injuries such as ACL rupture are common in sporting activities during landing, sudden stops, or changes in direction, and the rate of occurrence of such injuries is higher for non-contact mechanisms than for contact with opposing players [4]. Furthermore, research has shown that approximately 70% of non-contact injuries occur in the support leg [5].
Dynamic knee valgus (DKV) movement is a mechanical change that occurs in the knee due to non-contact injuries. DKV is an altered pattern or deformation of lower extremity alignment that is predominantly observed in the coronal plane. Studies have reported that two-thirds of all ACL ruptures occur as a result of non-contact injuries [6, 7]. In DKV, the representative changes in the joints of the lower extremities include internal rotation of the femur and external rotation of the tibia, and reduced dorsiflexion of the ankle, along with weakening of the hip abductor and external rotator function, have been reported to promote DKV [8]. Khayambashi et al. reported that low external rotational strength of the hip increased the risk of ACL rupture by 1.23-fold and abduction by 1.12-fold [9].
From a functional anatomical perspective, the gluteus medius (GM) primarily contributes to hip abduction but plays a secondary role in initiating hip extension and external rotation [10]. In addition to the GM, the tensor fasciae lata (TFL) plays a primary role in hip abduction. The abduction torque produced by the GM and TFL regulates the exercise geometry of the lower extremities by stabilizing the pelvis relative to the stationary femur in a single-legged stance [11]. Considering these facts, a study examined GM to develop a strategy for preventing ACL injury. They found that GM and abductor improvement training led to positive improvements in muscle function in the lower limbs and helped prevent valgus in the knee [12].
The GM and TFL act complementary; therefore, the weakening of GM function causes unnecessary movement of the surrounding structures, including the waist and knees, and TFL activity is likely to increase as a compensatory measure [13]. However, the TFL plays a functional role in both hip flexion and internal rotation to promote DKV movement. Mechanisms in the knee can lead to alterations in joint biomechanics, which can ultimately cause pathologies, including ACL injury [14].
Weakening of the GM, which acts as an abductor, can damage the lower extremities due to an imbalance in support and movement control for weight-bearing and DKV [15]. Therefore, exercises performed in the weight-bearing position are more functional than those performed in the non-weight-bearing position. This is crucial for joint stability in sports-related scenarios and similar to non-contact situations that may result in injury to the lower extremities, warranting investigation in similar environments. Furthermore, the weight-bearing position is more beneficial than the side-lying position because it has fewer location restrictions and offers greater convenience [16].
To the best of our knowledge, this is the first study to investigate the efficacy of GM exercise under weight-bearing conditions. In this experimental study, a motion analyzer was used to investigate the immediate effects of weight-bearing GM exercises, and a ground reaction force device was used to analyze the acute effects of DKV on muscle function in the lower limbs. The results of this study may provide additional insights into performance, injury prevention, and evidence-based knowledge to guide GM training and promote effective training.
Methods
Participants
We recruited 18 healthy adults aged 24-32 years (nine men and nine women) by advertising on the bulletin board of a training center. We used G*Power software (version 3.1.9.7, Universität, Düsseldorf, NRW, Germany) to determine the number of cases required for appropriate statistical power (
As the measurements were performed in triplicate in a single group, the experiment was conducted using a counterbalanced method to exclude learning effects. The researcher created six groups, each group featuring three participants, and assigned them to three different exercise sequences (ABC, ACB, BCA, BCA, CAB, and CBA), as described previously [18].
The demographic characteristics of 18 participants (mean
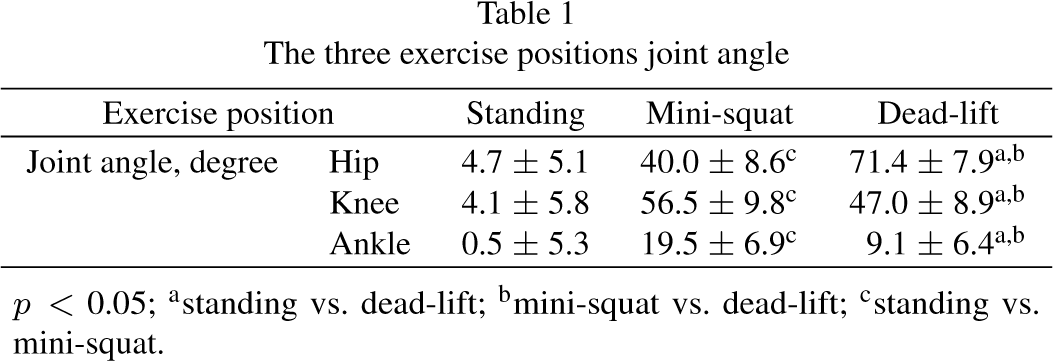
The three exercise positions joint angle
The three exercise positions joint angle
Three exercise posture for gluteus medius: a, standing b, mini-squat c, dead-lift.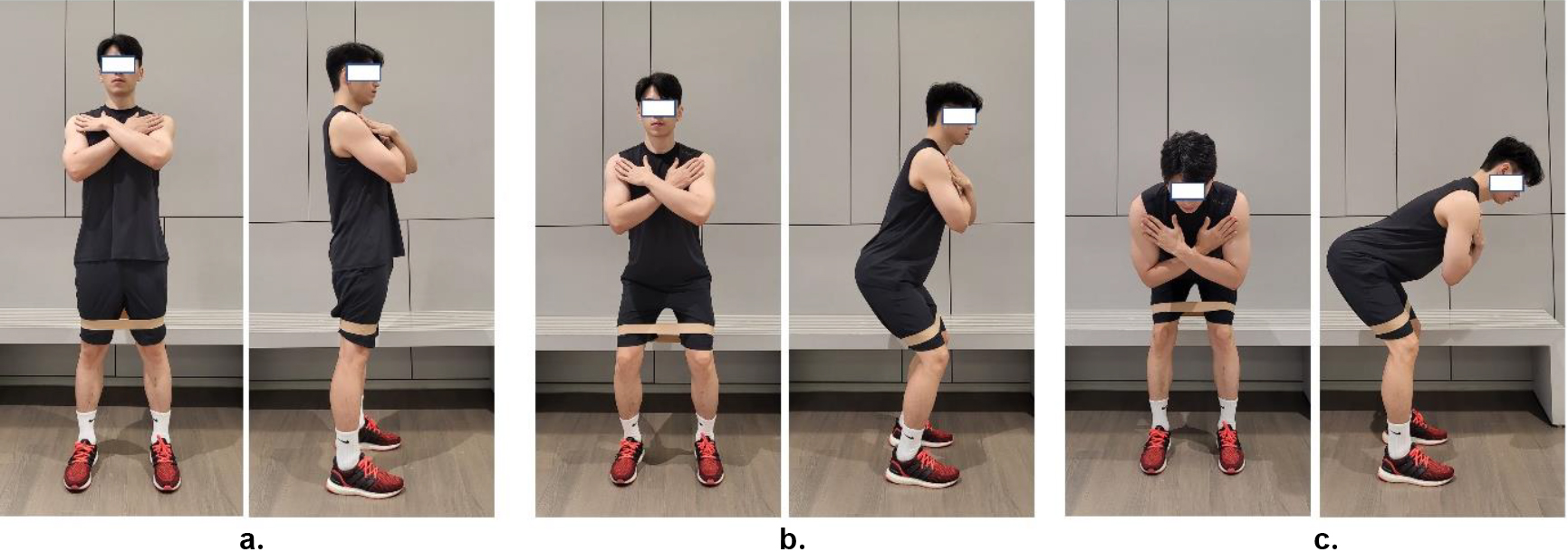
Three exercise positions (standing, mini-squats, and dead-lifts) were selected based on previous studies (Table 1 and Fig. 1) [19, 20, 21]. A red elastic loop band (Hygenic Corporation, OH, USA) was used to provide resistance to the GM exercise. Participants were asked to keep their feet at hip width and their spine neutral. The loop band was then fixed to the distal femur. Following the explanation and demonstration, participants practiced the exercise postures until they became familiar with them. The participants were asked to walk sideways in both directions at intervals 1.5-fold larger than the width of their hips. The movement was performed while maintaining the hip angle as much as possible. Tempo during measurement and exercise was limited to 40 repetitions/min (rep/min). Lateral band walking was performed with a loop band (3.7 lbs), and each participant performed 15 reps on a round trip for three sets with a 1-min rest period between sets, as described previously [22].
Anthropometric measurements
Anthropometric measurements were performed using a bioelectrical impedance analysis device (InBody 230; Biospace, Seoul, Korea) [23]. Measurements were taken in the morning after removing all metal substances in contact with the body. The researcher recorded each participant’s name, date of birth, height, and sex using the measuring device. The participant then stood on the metal foot-shaped sensor of the measuring device, and the researcher measured the participant’s weight while holding their breath for approximately 3 s. The researcher measured the participants’ weights by using a measuring device. Weight, height, body mass index, and body fat percentage were measured by lightly holding the handle with both arms spread at an angle of approximately 15∘ for 90 s.
The vertical single leg jump performed on a ground reaction machine.
The Y-balance test.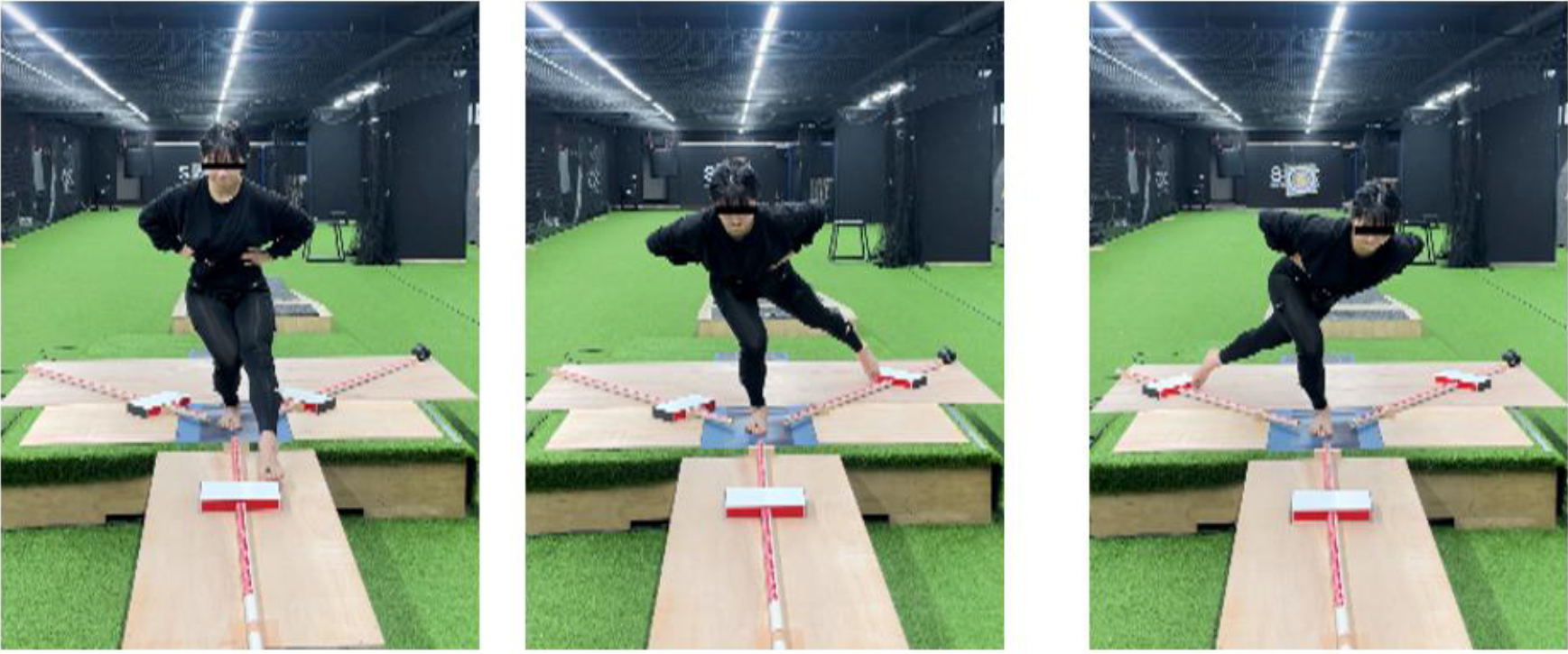
A ground reaction force device (OR6-7, AMTI, USA) was used to evaluate jumping performance and muscle function of the lower limbs. An amplifier was used to convert the charge values into force (Fig. 2). Before use, the ground reaction force device was preheated for over 30 min and calibrated to prevent drifts. During the experiment, the participants were asked to jump five times in a row on one foot as quickly and vertically as possible. Jumps were conducted using the preferred leg, and each participant was allowed three practice sessions to eliminate learning effects before data collection. If a jump was performed outside the ground reaction force machine or the foot opposite the one performing the jump touched the ground, the participant was asked to recover and repeat the test. For the analysis, the researcher utilized the highest record of all data collected over the five sessions. A 16-bit computer board A/D converter was used to acquire the measurement signals, and the ground contact and flight times obtained from the jump movement measurements were analyzed to confirm the jump height, power, and reflex strength index (RSI). Subsequently, the signals were analyzed using Nexus version 2.14.0 software (VICON Motion System Ltd., Oxford, UK) with a sample rate of 1,200 Hz, a gain of 4000, and a voltage range of
Marker site for motion analysis system.
Next, a Y-balance test (YBT) kit (FMS Inc., Evans-ville, IN, USA) was used to evaluate dynamic balance ability in relation to lower limb muscle function (Fig. 3). The YBT can help evaluate dynamic balance and a comprehensive range of functions in the lower extremities, including muscle strength, flexibility, and proprioception, by inducing coordinated movements in three directions (anterior, posterolateral, and posteromedial) [25]. Before measuring dynamic balance, each participant was trained to maintain correct posture and prevent injury. The participants were prepared by standing on the central platform of the kit on one foot. The maximum extension point was measured (in cm) while the participants held their waists with both hands and maintained balance in each direction using the opposite legs. The preferred leg was followed by the non-preferred leg, and the measurements were acquired three times in each direction. The highest values were used for the analyses. During measurements, a “foul” was declared if the extending foot touched the ground or the supporting foot deviated from the designated platform. The examiner recorded the movement in each direction (in cm), measured the leg length of each participant, and calculated the total score for each measurement item, as described previously [26].
Evaluation of dynamic knee valgus (DKV)
To measure DKV, the examiner filmed the movements of the supporting leg during the YBT and the landing leg during a single-leg vertical jump. Ten three-dimensional (3D) motion analysis cameras (Vero v2.2 VICON Motion System Ltd., Oxford, UK) and ten infrared cameras were used to cover a space of 2 m2. The camera placement was designed to provide sufficient time for image acquisition. Each infrared camera was connected to a data cable to transmit information to a desktop computer, which permitted measurements to be acquired using a local area network cable connected to a master camera. Prior to the experiment, the spatial coordinates were generated using a T-shaped wand to form a coordinate system within the room. The examiner used a wand to calibrate the system within the laboratory space to minimize the chance of data errors during the experiment. The position coordinates of the reflective marker captured by the infrared camera was calculated as a function of the position coordinates over time using digital labeling in the motion analysis system. Missing marker data were replaced with cubic spline interpolation.
To acquire 3D positional data of the body segments, the examiner attached 16 (size, 14 mm) reflective markers to a laboratory coat worn by each participant (Fig. 4). Next, the examiner used the plug-in-gait lower body marker set method to attach markers to the iliac crest, anterior superior iliac spine, posterior superior iliac spine, thigh, lateral epicondyle of the femur, lateral malleolus, 2nd metatarsal head, and heel on both the left and right sides [27]. Once all markers were attached, the examiner performed standing calibration to measure the alignment of the anatomical position.
Single-leg vertical jump performance
Single-leg vertical jump performance

3D video of motion analysis system.
For the YBT, the examiner performed an analysis when the supporting leg was fully extended. However, for the one-leg vertical jump, the examiner analyzed the maximum knee flexion of the landing leg after the jump. Next, the Vicon Nexus software (VICON Motion System Ltd., Oxford, UK) was used to calculate the three dimensions of hip and knee movement (flexion/extension, adduction/abduction, and internal rotation/external rotation) and the joint angle to explain the specific variables associated with DKV (Fig. 5).
For DKV data extraction, the data acquired from each motion were detected by an infrared camera (Vero 2.2, VICON, Oxford, UK), converted into digital signals by an integrated motion analysis system (Vicon MX Giganet, Oxford, UK), and analyzed using Nexus version 2.14.0 software (VICON Motion System Ltd., Oxford, UK). The sampling rate was set at 300 Hz. To reduce errors caused by noise associated with skin movement, inaccurate labeling, and electrical interference, the cut-off frequency was set to 10 Hz. Data smoothing was performed using the Butterworth 4th order low pass filter technique, and noise was removed [28]. Data on the joint angles (X-, Y-, and Z-axes) of the hip and knee joints were extracted from the filtered data (Fig. 5).
All data analyses were performed using SPSS Ver 25.0 (IBM Corp., Armonk, NY, USA). The mean and standard deviation of each variable were calculated. The Shapiro-Wilk test was used to verify normality. One-way analysis of variance was used to analyze differences in muscle activity according to the three postures, differences in muscle function in the lower extremities, and DKV variables following exercise. Statistically significant items were subjected to post-hoc analysis using the Least Significant Difference (LSD) test. The significance level for all tests was set at
Results
Exercise posture and muscle function
Single-leg vertical jump
Table 2 outlines the results of the single-leg vertical jump measurements. There was a significant difference in jump height depending on the posture (F
Y-Balance test
Y-Balance test

Single-leg landing leg angles after a vertical jump
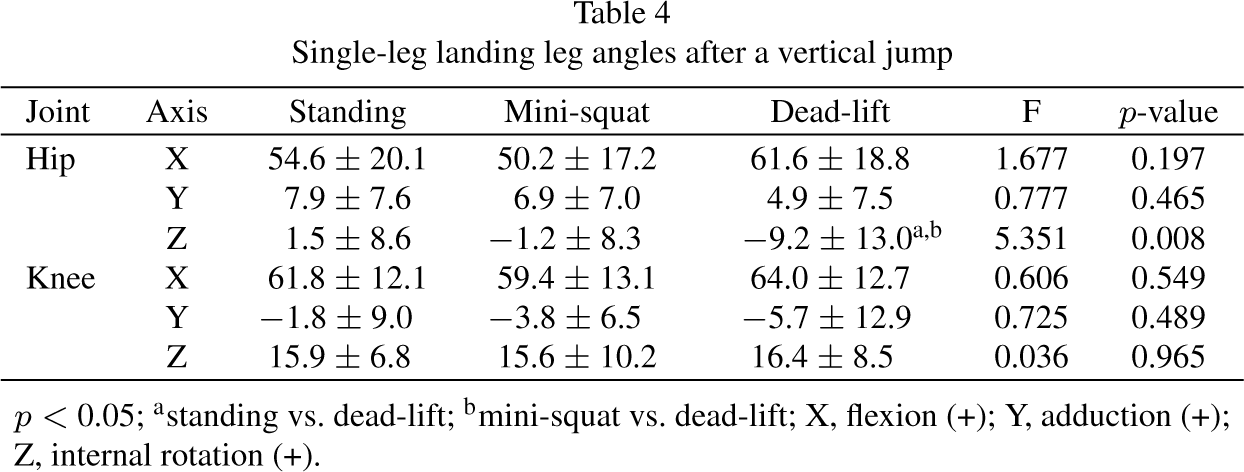
Table 3 outlines the results derived from the YBT. There was a significant difference in the total score (F
Dynamic knee valgus
Table 4 shows the results derived from the landing leg DKV during the single-leg vertical jump exercise; a significant difference was detected between postures for the hip Z-axis (F
Support leg angles during the Y-Balance test
Support leg angles during the Y-Balance test
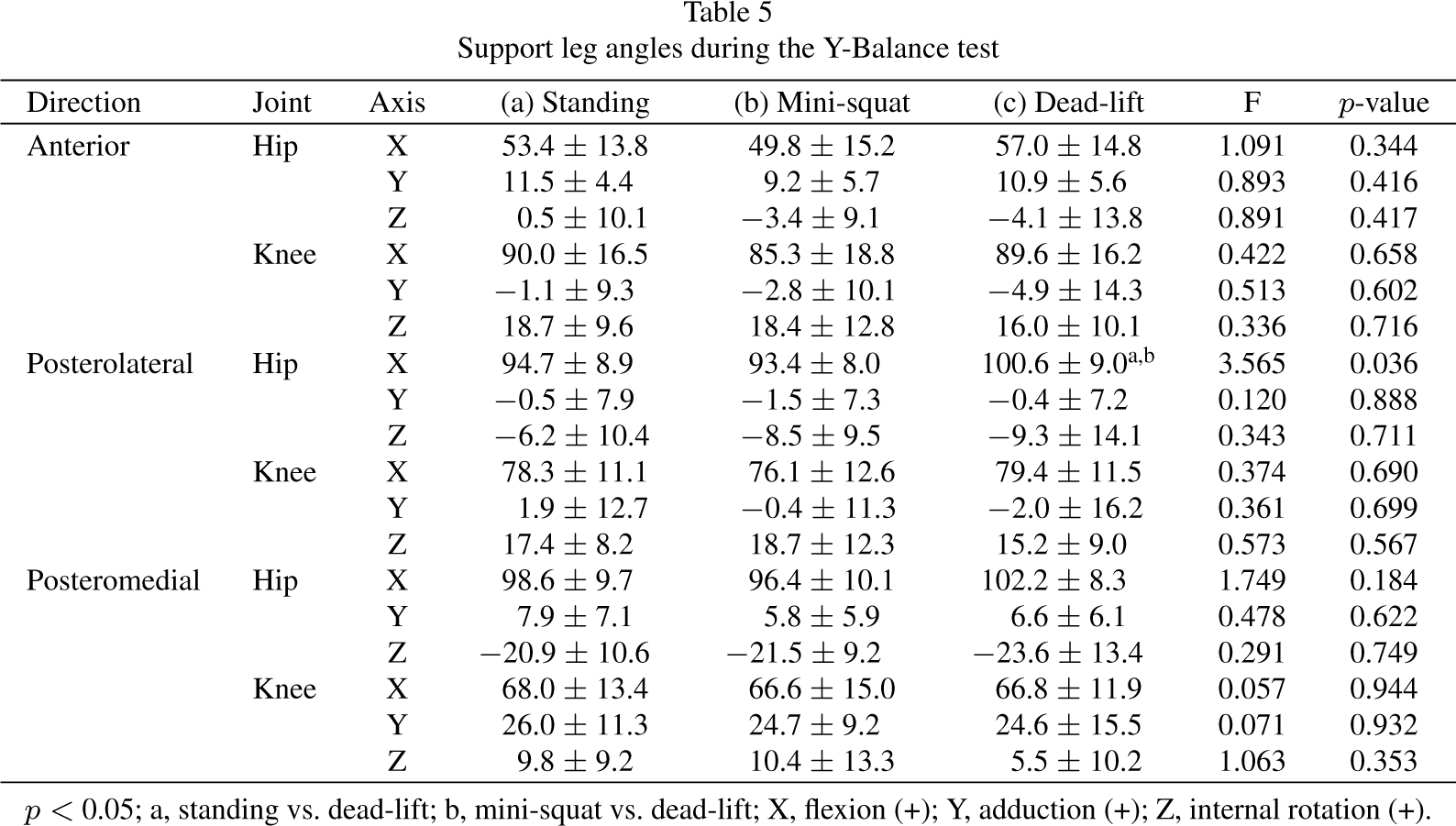
Table 5 summarizes the measurements of the support leg angle during YBT. A significant difference was detected for the hip X-axis in the posterolateral direction (F
This study analyzed the immediate impact of GM exercises performed in three postures on functional changes in the lower extremities. The vertical single-leg jump was measured following the lateral band walk exercise. In terms of jump height, the dead-lift was significantly higher than that in the standing and mini-squat trials. The GCT was also shorter for dead-lifts, although this difference was not statistically significant. Power and RSI were also higher for dead-lifts, although this was not statistically significant. These results concur with numerous studies reporting that GM exercise can influence vertical jump height [29, 30]. However, in contrast to the findings of Comyns et al. [31] and Healy et al. [32], who analyzed track and field athletes, gluteal warm-up showed no significant effect on squat jumps or countermovement jump heights.
Previous studies have also identified effects on jump performance variables, including power, GCT, and RSI [29, 33]; however, no significant differences were detected in terms of these variables in the present study. These differences may be attributed to the fact that the participants in the present study were healthy adults, whereas those in previous studies were athletes. The physiological response to the jumping technique and post-training changes may be greater in trained athletes [34], which could explain why researchers did not observe any differences in the GCT and RSI.
In a previous study, Comyns et al. [31] measured squat jumps and counted movement jumps following a glute exercise warm-up and found that jump height did not show an improvement. In a previous study, seven exercises were performed as a warm-up program for the gluteal muscles, and no change was observed due to the accumulation of fatigue. However, the authors reported that performance improved after eight minutes of recovery. In the present study, only one GM exercise was performed before measurement; consequently, the muscle fatigue was lower than that reported in previous studies. Furthermore, jump height appeared to improve because of the appropriate promotion of muscle contraction.
This study used the YBT to evaluate dynamic balance ability following lateral band walk exercises according to posture. Posterolateral and total scores for the non-preferred leg were significantly higher in the dead-lift posture than in the standing and mini-squat postures. These results are consistent with those of previous studies that showed that exercises focusing on the gluteal muscles were effective in terms of dynamic balance ability [35, 36]. In 28 female athletes, the acute effect of neuromuscular reflex training involving the gluteal muscles led to an increase in YBT scores [36], whereas in 48 soccer players, pelvic stabilization exercises involving the gluteal muscles led to an improvement in YBT scores [37]. Previous researchers have reported that strength in the hip joint can improve YBT, and that the dead-lift posture is likely to stimulate the GM and increase efficiency, thus contributing to pelvic stability and improving YBT [38, 39]. In the present study, researchers identified significant differences in the posterolateral direction. In a previous study, Francis et al. reported a strong correlation between hip abduction and the posterolateral direction (
In this study, DKV was evaluated by measuring the movements of the supporting leg during YBT and the landing leg during single-leg vertical jumps. In terms of supporting leg movements, dead-lifts resulted in significantly higher hip flexion than standing or mini-squat postures. No significant differences were detected among the other joints. In terms of landing leg movement, dead-lift resulted in a significantly higher external rotation of the hip than standing and mini-squat postures. No significant differences were observed in the other joints. These results can be compared with those of studies reporting knee valgus in one-leg squats on the supporting leg [41, 42] and with those of studies reporting knee valgus on the landing leg [43].
Mirzaee et al. [36] analyzed the acute effects of DKV on one-legged squat movements in 28 women after applying a neural reflex exercise program involving the gluteal muscles and reported an improvement in DKV. Willy and Davis [41] investigated individuals with excessive hip adduction in another study. They reported that a 6-week program involving glute-muscle strengthening exercises improved abnormal movements by reducing hip adduction and increasing abduction and external rotation. Jamali [42] reported improved DKV in response to hip abductor and external rotator strengthening exercises in 35 patients with PFPS who used elastic bands for 12 weeks. However, Wilczynski et al. [44], who used a GM exercise program in 45 soccer players with unstable knee joints for 6 weeks and measured knee valgus during one-leg squats, reported a non-significant reduction of 2.62 degrees. In the current study, we detected only high levels of hip flexion in the dead-lift position and did not detect any significant differences in variables related to knee valgus. The reason for the increased posterolateral distance during YBT appears to be better control of hip flexion. The secondary function of the GM is hip extension, which enhances control during eccentric contractions, particularly evident during activities that require hip flexion. This biomechanical role is critical, as demonstrated by a study from Overmoyer et al. [45], which reported a significant correlation between YBT and hip flexion (
Hip flexion is an important factor in determining knee valgus [46]. A previous study reported that if appropriate hip flexion was not achieved, hip joint muscle activity can decrease, thus increasing knee valgus [47]. The YBT is used as an assessment tool for lower extremity injuries and prevention. An enhanced score, even in the absence of differences in knee valgus, is believed to positively impact injury prevention [48]. Jo et al. [49] reported that hip extensor and abductor training significantly reduced DKV in women.
The hip plays an important role in neuromuscular control and compensation for the excessive movement of the lower extremities during exercise. As hip movement predominantly involves the action of the gluteal muscles, it is important to consider whether hip abduction and external rotation movements can normalize DKV [50]. Furthermore, a weakened hip abductor can require compensatory exercises for pelvic descent and lateral trunk displacement [51]. Several studies have reported an association between increased DKV and weakened hip strength in one-leg movements and abductor, external rotator, and extensor weakness in both sexes [52, 53]. In a previous study, Hiemstra et al. [54] reported that a 3∘ difference in DKV angle in knee kinematics was clinically meaningful. Therefore, providing comprehensive instructions on exercise movements is vital when performing preventive and rehabilitation exercises for patients with chronic musculoskeletal diseases.
While this research offers valuable insights into the impact of different weight-bearing exercises on the functional dynamics of the lower extremities, some limitations are important to acknowledge. First, the research included only small groups with a relatively small number of participants, and repeated measurements were performed in triplicate. In a previous study, Healy et al. [32] discussed the learning effect within the experimental methodology. Their experimental design featured measurements on three consecutive days: the first day (measurement before glute exercise), second day (measurement after exercise), and third day (measurement without glute exercise). The authors detected a difference between the first and second days but not between the second and third days, despite exercise being performed only before the second day’s measurement. This pattern was interpreted as a learning effect on the measured movement, suggesting that the gluteal exercise had no significant effect. The researcher used a counterbalanced method to consider the effects of learning in this study. As studies on the effects of preparatory exercise or acute exercise, including GM, vary depending on the intensity of exercise, it will be necessary to investigate the effects of band intensity to strengthen GM in future studies. The primary purpose of this study was to investigate the immediate effects of one-time training; the long-term effects may likely generate different results. Furthermore, because the same loop band was applied, there may have been differences in muscle contraction between the individuals. This study did not analyze potential sex-specific differences in outcomes between male and female participants. Finally, this study included only healthy and untrained athletes. Future studies should include more participants and conduct additional experiments to address these limitations.
Conclusion
In this study, we investigated the differences in muscle function in the lower limbs and DKV during weight-bearing GM exercises, depending on posture. During the lateral band walking exercise, we identified the high jump height in the dead-lifted position. A larger posterolateral direction was also detected in the non-preferred leg during YBT. During the lateral band walk exercise, there was a high level of hip flexion of the supporting leg in the dead-lift position and a high level of external hip rotation in the landing leg, suggesting that GM exercise plays a key role in stabilizing the DKV. These results suggest that the dead-lift posture has a more positive effect on muscle function in the lower limbs and DKV than standing and mini-squat postures. These findings provide key guidance for facilitating future research and developing new training strategies.
Funding
The authors report no funding.
Availability of data and materials
The data presented in this study are available on reasonable request from the authors.
Author contributions
CONCEPTUALIZATION: SO and JH and YK.
METHODOLOGY: SO and JH.
FORMAL ANALYSIS: SO and JH and YK.
INVESTIGATION: SO.
ORIGINAL DRAFT WRITING: SO and JH and YK.
REVIEW AND EDITING: SO and JH and YK.
SUPERVISION: SO and JH.
All authors contributed to the editorial changes in the manuscript. All the authors have read and approved the final version of the manuscript.
Ethical approval and consent to participate
All participants provided written informed consent for the examination and publication of the study. This study was approved by the Research Ethics Committee of Chung-Ang University (approval number: 1041078-20221130-HR-023, January 26, 2023).
Footnotes
Acknowledgments
We would like to thank Chung-Ang University for editing and administrative support.
Conflict of interest
The authors have no conflicts of interest to report.