
Abstract
BACKGROUND:
Warm-up exercises are often recommended to enhance flexibility, reduce the risk of injury, and improve performance. However, the optimal number of warm-up repetitions remains unclear. Additionally, the previously suggested sit-and-reach test may not be suitable for efficiently stimulating the target muscles.
OBJECTIVE:
This study investigated the effects of a warm-up consisting of 15 straight leg raise (SLR) repetitions on hip and knee flexibility by comparing individuals with and without hamstring tightness (HT and NoHT, respectively).
METHODS:
Thirty healthy adults were classified as having HT or NoHT based on their SLR angle before warm-up. The participants performed 15 repetitions of the SLR as warm-up, followed by hip and knee flexibility tests.
RESULTS:
Warm-ups significantly improved hip and knee flexibility in both HT and NoHT groups. Improvements in flexibility were not significantly different between groups. The most notable increase in flexibility was observed between the sixth and ninth SLR trials.
CONCLUSIONS:
The clinical utility of a warm-up consisting of 15 SLR repetitions is supported by this study, as a substantial increase in hip flexibility was observed in all participants regardless of HT. In clinical settings, a maximum of 10 repetitions may be sufficient to achieve optimal results.
Introduction
Warm-up exercises are widely employed to prevent sports injuries before exercise, and are categorized into passive and active types based on the participant’s voluntary movement. Passive warm-up utilizes external heat sources, such as hot packs, to conduct heat from external mediators to internal tissues [1, 2]. In contrast, active warm-ups generate heat within internal tissues through energy metabolism by contracting muscles without causing muscle fatigue, thereby increasing their temperature and making them more pliable [3, 4]. Active warm-ups typically involve repeated concentric and eccentric contractions of target muscles. For example, when targeting the hamstrings, repeated flexion and extension of the hip and/or knee joints are performed based on the anatomical characteristics of these muscles. Repeated hamstring movements can be broadly classified into straight leg raise (SLR), which primarily involves hip joint movement, and active knee extension (AKE), which primarily involves knee joint movement [5, 6]. SLR-based warm-ups enhance hip extensor flexibility, while AKE improve knee flexor and hip extensor flexibility due to stimulation of the entire musculature of the posterior thigh during maximal knee extension [7].
Warm-up protocols using the AKE test typically consist of six repetitions, considering the first five repetitions as warm-up and the last as baseline [8, 9]. However, scientific evidence for this repetition number is ambiguous. Many experimental studies have referenced the research of Atha and Wheatley on warm-up exercises involving repeated reciprocal joint motion [10]. It appears reasonable to set the sixth repetition as the baseline because there is a partial attenuation of the increase in flexibility after four repetitions. However, the flexibility continued to increase even after the fifth repetition. Additionally, the modified sit-and-reach hip flexion test rather than the AKE test was used in the reference experiment. Unlike the AKE test, the sit-and-reach hip flexion test maintains full knee extension and concentrates most of the stimulation on a single joint, namely the hip extensor. In summary, no statistically significant differences were observed between repetitions, and the reciprocal joint motion used in the Atha and Wheatley study differed from the AKE motion. Therefore, determining the optimal number of repetitions based solely on this study is inappropriate.
Questions can arise regarding the appropriateness of the sit-and-reach hip flexion test as a warm-up for lower body muscles [11]. In the sit-and-reach test, the participant sat on the floor with the knees fully extended and leaned forward with the upper body. This can stimulate not only the lower body muscles but also passive connective tissues, such as the thoracolumbar fascia, to a greater extent [12]. In clinical settings, the SLR motion is often preferred. Many examinations of hamstring flexibility and interventions to improve hamstring flexibility are based on the hip flexion-extension movement. Notably, scientific studies have demonstrated that PNF stretching using the hold-relax technique significantly enhances hip flexion flexibility [13, 14]. While the tensile force is higher than that during warm-up, studies on stretching performed in the SLR position have shown significant increases in both hip and knee flexibility. However, the effectiveness of a warm-up utilizing the SLR motion has not been verified.
Participant characteristics
Participant characteristics
HT, individuals with hamstring tightness; NoHT, individuals without hamstring tightness; BMI, body mass index.
The effect of the warm-up can vary depending on an individual’s inherent flexibility, even when the type of warm-up and number of repetitions are identical. Assuming that a constant force is applied to body tissues, individuals with hamstring tightness (HT) are expected to have a smaller increase in flexibility due to the stiffness of their tissues compared to individuals without hamstring tightness (NoHT), as observed in sex comparisons [15]. Conversely, individuals with NoHT may experience a smaller increase owing to the ceiling effect [16]. To verify these two contrasting inferences, separate analyses of flexibility changes based on inherent flexibility are required. Unfortunately, most existing studies do not directly compare HT and NoHT, and focus only on individuals with muscle tightness. Some studies have verified significant increases in flexibility after stretching in individuals with normal flexibility; however, no studies on the effect of warm-ups have been conducted to date [17]. Women generally have greater joint flexibility than men and show greater increases in flexibility after stretching [18, 19, 20]. However, it cannot be concluded that the difference in flexibility increase between men and women is solely due to the initial flexibility difference, as women have different hormone levels that affect muscle composition and flexibility, as well as different resistance to muscle fatigue [21, 22, 23, 24]. If the initial difference in joint flexibility influences the effects of warm-ups to some extent, it is necessary to establish different warm-up protocols in clinical settings for verification.
This study aimed to investigate the effects of warm-up exercises consisting of 15 repetitions of the SLR on hip and knee flexibility and the difference in flexibility improvement between individuals with HT and those with NoHT. In doing so, it seeks to contribute to the formulation of more effective warm-up strategies tailored to an individual’s inherent flexibility.
Participants
Thirty healthy adults (10 males and 8 females in the HT group, and 7 males and 5 females in NoHT group) participated in this study (Table 1). Participants were excluded if they had neurological problems in the vertebral column or lower extremity joints or if they had experienced musculoskeletal pain within the past 6 months [25, 26]. Initially, 32 participants were enrolled; however, two were excluded from the analysis because of data collection errors during measurement. The study was approved by the Institutional Review Board of Woosong University and informed consent was obtained from all participants.
Procedures
Baseline flexibility was measured using the SLR and AKE tests before warm-up, and the results were recorded as Pre-SLR and Pre-AKE, respectively. During warm-up, which consisted of 15 repetitions of the SLR motion (maximal hip flexion and full hip extension), the angle of maximal hip flexion was recorded for each trial. Flexibility improvement was measured using the SLR and AKE tests after warm-up, and the results were recorded as Post-SLR and Post-AKE, respectively. The detailed procedures for the two tests and warm-up are as follows.
For the SLR test, the participants lay supine on a treatment table with their backs against the floor. Both legs were placed comfortably on the treatment table with full hip and knee extension. The examiner instructed the participants to slowly raise their legs for testing. The contralateral leg and pelvis were secured to the treatment table by using straps. The participants actively raised their lower extremities ensuring that the knee remained extended. Slight ankle plantar flexion was allowed to prevent unnecessary stretching of the neural and soft tissues due to ankle dorsiflexion. When the maximum angle was reached, the examiner measured the hip flexion angle using a smartphone inclinometer application installed on the iPhone 14. The smartphone was positioned along the midline of the femur, referencing the axis of the femoral greater trochanter and lateral epicondyle [27, 28].
Changes in range of motion over 15 repetitions of straight leg raise in HT (a) and NoHT (b) HT, individuals with hamstring tightness; NoHT, individuals without hamstring tightness. *Significant difference compared to the first trial.
Improvement of flexibility assessed by straight leg raise test (a) and active knee extension test (b) HT, individuals with hamstring tightness; NoHT, individuals without hamstring tightness; WU, warm-up. *Significant difference compared with Pre-WU.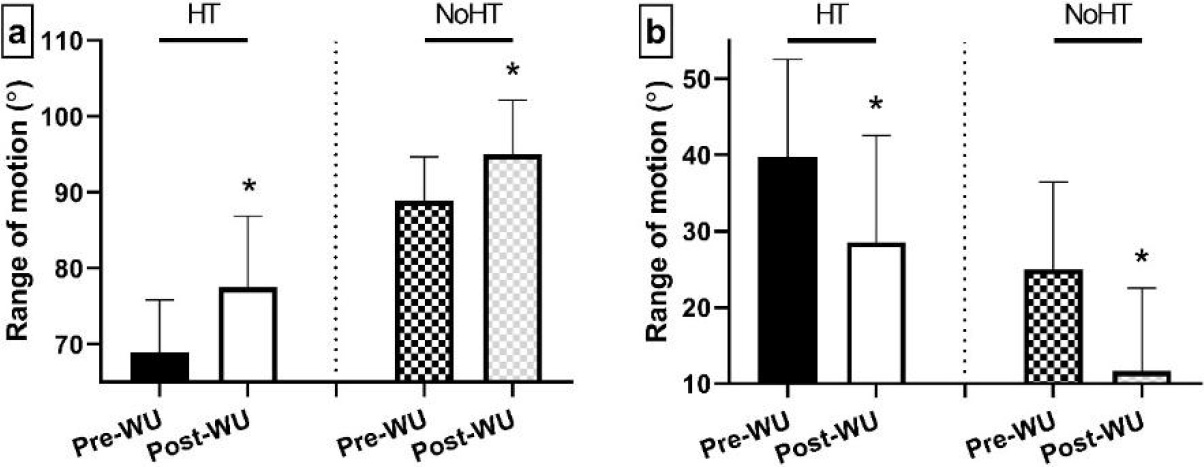
For the AKE test, the participants lay supine on a treatment table. The hip and knee joints of the leg being tested were flexed to 90
The active warm-up consisted of 15 SLR motion repetitions. In the supine position, the participants actively raised their legs in accordance with the examiner’s cues. To prevent bouncing at the end range owing to rapid movement, the leg was slowly raised. The participant briefly held the position at maximal hip flexion, and the examiner measured the angle using the inclinometer application [5]. Once the angle measurement was completed, the participant slowly lowered the leg until it touched the treatment table. Without resting, the participants immediately raised their legs again to perform the next trial.
The Shapiro–Wilk test was conducted to examine data normality. Independent
Within each group, paired
Data analyses were performed using IBM SPSS Statistics version 25 (IBM Corp., Armonk, NY, USA). Statistical significance was set at
Results
In this study, participants with a hip flexion angle
In the HT group, the third (
In the HT group, the Post-SLR angle was 77.0
In the NoHT group, the Pre-SLR (
Discussion
This study contributes to the understanding of the effects of a warm-up exercise consisting of 15 SLR repetitions on hip and knee flexibility. Additionally, it examined whether there was a difference in flexibility improvement between individuals with HT and NoHT.
The observed improvements in flexibility measured by the SLR and AKE tests following warm-up support the hypothesis that specific repetitions of the SLR targeting the hip joint can enhance both hip and knee flexibilities. This suggests a comprehensive enhancement of musculotendinous flexibility in the back of the entire leg rather than isolated improvements in the hip region. Although a direct comparison with high intensity stretching has some limitations, similar results have been reported in various stretching studies. The ROM of AKE increased after PNF stretching was performed in the hip joint without knee joint movement, and also after static stretching [13]. These changes were not limited to maximal intensity. A significant increase in the ROM of AKE was observed even in static stretching at a relatively low intensity, and the ROM of AKE improved by more than 10% in PNF stretching performed at 10% of the maximum [30, 31]. The flexibility increased after PNF stretching performed at 40% and 10% of the maximum could be maintained by simple standing toe touch, which involves full knee extension and hip flexion [32]. This is likely due to the influence of the tensile force on active and passive contractile proteins linked from the upper leg to the lower leg in the body [33]. Anatomically, all hamstrings, except the short head of the biceps femoris, are connected to the knee [34, 35]. In addition to muscles, many connective tissues connect the back of the upper trunk to the foot. Therefore, movement of the upper trunk is known to affect the ROM of the knee and ankle [33, 36]. Thus, increased flexibility of the lower back, which is connected to the pelvis and hip joints, leads to increased knee extension [37]. Notably, while the flexibility measured after the warm-up was significantly higher than that measured before the warm-up, flexibility did not continue to increase throughout the 15 trials.
In this study, flexibility peaked between six and nine trials and then gradually decreased. Most previous studies recommended six repetitions to avoid a cold start without providing real-time changes during the repetitions. A recent study measured the real-time changes during five AKE repetitions and observed a continuous increase in flexibility [6]. Similarly, in another experiment, both groups that held maximal knee extension for 5 s and those that did not hold it showed a continuous increase during six repetitions [5]. This suggests that the six repetitions suggested in previous studies may be insufficient to achieve the maximal effect. In this study, the number of repetitions was set to 15 to clearly identify changes in flexibility, which successfully identified a different pattern from that of previous studies. The ROM of the SLR started to show a significant difference from the third trial and gradually decreased after approximately the 10th trial. Several factors are likely to have contributed to this lack of continuous increase. Muscle fatigue can also occur during repeated tasks. The entire lower extremities account for a significant portion of the total body mass [38]. Repeated lifting of the legs requires substantial effort, and performing consecutive repetitions without rest may gradually make it more challenging to reach the maximal ROM [39]. During knee extension in the supine position, the hamstrings were coactivated with the quadriceps [40]. The lifting motion is a movement against gravity, but the lowering motion is a movement with the help of gravity; therefore, the fatigue of the quadriceps could be relatively high. In addition, tensile force to stretch the antagonist may occur at the endpoint, which may cause the participant to feel discomfort or pain, which may have led to unconscious avoidance of reaching the end point [41]. Looking at the longitudinal changes over 15 repetitions, it appears that more than the conventional six may be beneficial but exceeding 10 repetitions is unnecessary.
The increase in SLR due to warm-up was 8.6
The limitations of this study included the relatively small sample size and the absence of long-term follow-up assessments to gauge the persistence of flexibility. Additionally, it did not account for individual variations in daily physical activity or preexisting conditions such as joint injuries, which could influence flexibility outcomes. Future research should explore the long-term effects of warm-up exercises across diverse populations, considering variables such as age, sex, and physical activity levels.
Conclusion
This study provides valuable insights into the effects of a warm-up protocol involving 15 SLR repetitions on hip flexibility, with a particular focus on individuals with HT and NoHT. These findings indicate that warm-up routines require more than six repetitions of the SLR, with a suggested maximum of 10 repetitions. Although the limitations include a relatively small sample size and the absence of long-term data, this study clinically underscores the importance of incorporating warm-up exercises to enhance hip flexibility across all individuals, regardless of HT. This approach can potentially reduce injury risk and improve overall physical performance, highlighting the value of tailored warm-up protocols in sports and rehabilitation settings.
Author contributions
CONCEPTION. PERFORMANCE OF WORK.INTERPRETATION OR ANALYSIS OF DATA.PREPARATION OF THE MANUSCRIPT.REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Wootaek Lim.
Ethical considerations
All study procedures were approved by the Institutional Review Board of Woosong University. Informed consent form was obtained from all participants before the experiment.
Funding
This work was supported by 2023 Woosong University Academic Research Funding.
Footnotes
Acknowledgments
The author has no acknowledgments.
Conflict of interest
The author has no conflicts of interest to report.