
Abstract
Keywords
INTRODUCTION
In recent years, researchers developed and evaluated a wide range of cognitive interventions for patients with mild cognitive impairment (MCI) and Alzheimer’s disease (AD) dementia. Almost all of these interventions addressed specific cognitive functions (for reviews, see [1–3]). For example, Cognitive Training aims to maintain or improve specific cognitive functions, such as attention, episodic memory, and problem solving skills, using guided training and repetitions of standardized tasks. Cognitive Training showed positive effects on general cognitive functioning and selected cognitive abilities in MCI patients [4–6], but not in patients with dementia [2, 7]. However, even in MCI, evidence for long–term effects [4, 5] and a transfer of the trained cognitive abilities to activities of daily living is sparse [5, 6]. For this reason, cognitive interventions for AD dementia have adopted the concept of Cognitive Rehabilitation [8]. Rehabilitation in general aims to support individuals to achieve and maintain their optimal level of physical, psychological, and social functioning despite specific impairments [9]. Its main goal is to preserve the patient’s ability to engage in meaningful everyday activities. Cognitive Rehabilitation in particular aims to develop individualized strategies to deal with cognitive impairments [8]. It is characterized by 1) an individualized approach that identifies and pursues goals that are relevant to the patients and their everyday life; 2) the priority of maintenance of cognitive abilities and compensation of impairments over improvements of single cognitive skills; 3) the integration of multimodal methods by an interdisciplinary multi–professional team; and 4) the interaction with the individual’s environment to facilitate transfer from the rehabilitation program to daily life [7].
So far, only few studies have investigated the efficacy of Cognitive Rehabilitation approaches in dementia. Cognitive Rehabilitation proved to be more effective if the approach was highly individualized, focused on goals relevant to the patient [7], and if it was interactive [9–11]. In addition, training a specific everyday task required less residual transfer capabilities [11]. Furthermore, Cognitive Rehabilitation was shown to increase quality of life and to reduce depressive symptoms [12–14]. To date, however, empirical evidence that Cognitive Rehabilitation sustainably improves skills for activities of daily living (ADL) in mild AD dementia is lacking.
In the present study, we aimed to determine the feasibility and efficacy of a group–based Cognitive Rehabilitation program in a partial–randomized controlled trial with an active control condition. Additionally, we aimed at deriving effect size estimates on ADL–related cognitive skills to inform the design of future large–scale multicenter trials. We used a manual–guided Cognitive Rehabilitation approach [15] and adapted it to a group setting, allowing for social interaction effects. Furthermore, aiming to optimize the transfer of strategies, we added a problem–solving training related to everyday life.
METHODS
Subjects and design
Following a screening phase (n = 44), we included n = 20 individuals with either mild AD dementia or AD with a concomitant cerebrovascular disease (mixed dementia), recruited from the memory clinic of the University Hospital Rostock. All patients were diagnosed with probable or possible AD according to the NINCDS–ADRDA criteria [16], corresponding to a diagnosis of “probable or possible AD dementia based on clinical criteria” according to NIA–AA criteria [17], and characterized using the Mini–Mental State Examination (MMSE) [18]. Cerebrovascular comorbidity was diagnosed according to the ICD–10 criteria [19]. Patients were required to be living at home and to experience at least two face–to–face contacts with a caregiver per week. Subjects taking medication with neurological effects, such as antidementive, antidepressant, or antipsychotic medication, needed to have taken a stable dose during the past 3 months. Subjects were excluded if they had a history of epilepsy or psychiatric illness. Additionally, subjects were not included if they were unable to undergo an MRI examination. MRI data were described in an accompanying manuscript [20]. A radiologist visually inspected all MRI scans to rule out other neurological pathologies, such as tumors or acute stroke events. All participants received a neurological and psychiatric examination and blood testing to determine routine clinical parameters. The study was conducted according to the Declaration of Helsinki and had been approved by the local medical ethics committee of University Hospital Rostock, with all participants providing written informed consent. The study was registered in the database of clinicaltrials.gov (“A 2014–0113”).
Five subjects originated from a pilot trial waiting group and were already predetermined for the intervention group. We conducted a partial–randomization to assign the remaining subjects (n = 15), using a computer–based balanced randomization.
Outcome measures
All outcome measures were assessed at baseline and at follow–up, i.e., within 14 days after completion of the intervention/control program.
Primary outcome: ADL–competence
Activities of daily living (ADL–competence) were measured on two scales. Firstly, we used the Bayer Activities of Daily Living Scale (B–ADL) [21], consisting of 25 items to be answered by the caregiver, with the mean ranging from 1 (no impairment) to 10 (permanent impairment). Secondly, we employed the Nuremberg Aging Observation Scale (NSL) [22], completed by both the patients (NSL–P) and the caregivers (NSL–C). This questionnaire consists of 15 items, e.g., dressing, washing, and shopping. A score of 0 indicates no deficits; a score of 30 indicates maximum disability.
Secondary outcomes
Cognitive abilities related to daily living. We administered three tests to assess skills that are especially relevant to everyday life. Everyday memory abilities were assessed using the Rivermead Behavioural Memory Test (RBMT) [23]. This test includes practical demands such as replicating a route across the room, but also prospective memory demands such as remembering a future appointment. To assess planning and organizational skills, we used two subtests of the HOTAP (Handlungsorganisation und Tagesplanung) test [24], which differed in complexity: The subtest HOTAP–A (“individual actions”) requires the correct sorting of photos, showing sequences of typical everyday actions, e.g., making coffee or doing laundry. The HOTAP–C (“semi–structured daily schedule”) subtest requires fitting single actions into a pre–structured daily schedule, relying on logical reasoning, considering time points and rules. The ratio of the correct items and the invested time, as well as the combined sum scores across HOTAP–C dimensions were used as dependent variables. As an indicator for communication competence, spontaneous speech was measured using the Boston Cookie Theft picture description task, in which a drawn scene has to bedescribed [25].
Functional cognitive state. To assess functional cognitive state, we used the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) test battery [26], a standardized and reliable instrument to assess cognitive functions, including attention, memory, executive functioning, visuo–spatial skills, and language.
Non–cognitive domains. Non–cognitive domains comprised quality of life (measured by the Dimensions of Quality Of Life, DEMQOL [27], which is a questionnaire including patient and caregiver rating), presence and severity of depression (Geriatric Depression Scale, GDS [28], long version with 30 items), the level of consciousness (Apathy Evaluation Scale, AES –patient and caregiver rating), neurobehavioral disturbances (Neuropsychiatric Inventory, NPI, caregiver rating [29]), and the caregiver’s burden (Zarit Burden Inventory, ZBI [30]).
Intervention
Our study examined the effects of a Cognitive Rehabilitation program. This intervention was based on the CORDIAL program, a manual–guided approach combining neuropsychological and psychotherapeutic elements, presented by Werheid and Thöne–Otto in 2010 (“Cognitive Rehabilitation and cognitive–behavioral treatment for early dementia in Alzheimer disease, CORDIAL”) [15]. This outpatient intervention spans a period of 12 weeks and consists of six modules with 2 sessions each, with one session (60 min) per week. The six modules are described below: Identification of problems and definition of treatment goals. This includes determining obstacles to independent living, e.g., the inability to utilize cooking devices, and aspects that reduce the quality of life (e.g., the perception of one’s impairments, or depressive thoughts). Use of external memory aids, e.g., signposts, lists, or calendars. Introduction and implementation of daily routines and a structured framework for the day. This includes exercising daily activities (e.g., making coffee) and repeating these tasks at home, using a written instruction or a schedule, for example one listing the morning routines. Organization and implementation of pleasurable and meaningful activities. This includes activities ranging from psychoeducation (in order to prevent depression or apathy) to planning activities like social events and hobbies, etc., to enhance the perception of self–efficacy. Reminiscence, i.e., biographical work. This includes dealing with important life events or phases, such as work experience, to retain the temporal structure of life and the use of resources.
Evaluation of achieved goals and planning of future procedures.
We adapted this program in the following way: We replaced the individual format with a single therapist by a small group program, guided by a psychologist and an occupational therapist. This aimed at increasing social cohesion and support among the group members, as well as rendering the program more cost–effective in a routine care setting. We extended the sessions from a one–hour session per week to one two–hour session per week, allowing sufficient time to address individual needs despite the group setting. We allowed the order of the modules to vary flexibly in response to the participants’ needs. We reduced the complexity of the worksheets according to the cognitive state of the participants. We reduced the frequency of the caregiver participation from 6 sessions to 3 sessions, according to caregiver availability. We added advanced training of everyday tasks to facilitate the transfer of strategies to daily life, such as reading and discussing newspaper articles using the “PQRST” method [31] to improve temporal orientation and communication skills, or training basic financial transactions, etc.
During the sessions, we first set goals for the week. For example, we established possibilities to improve compensation of memory deficits (e.g., using external memory aids, or simplifying requirements, etc.). Secondly, explicit tasks were discussed, for example the individual use of a specific memory aid or performing one specific activity a day, and memory aids were created (e.g., calendar, day plan). All discussed items and the tasks were written in a diary. To monitor the activities at home, we called the caregivers once a week.
Active control condition
As an active control condition, we used a standardized Cognitive Training in the form of homework that each participant had to do on his or her own. The tasks originated from a Cognitive Training program [12] aimed at training specific cognitive functions, such as memory, attention, executive functions, and psycho–motor abilities. Patients were asked to perform one task per day; this was not monitored explicitly. The control group met every four weeks to evaluate the homework in order to maintain adherence to the study.
Statistical analysis
All data were analyzed using SPSS V.21. Missing questionnaire items (0.38%) were replaced by the respective item score, averaged over the respective group. In case of missing test data (0.74%), the subject was excluded from the respective analysis. Normally distributed dependent variables were analyzed using parametric tests, while non–parametric tests were used for non–normally distributed dependent variables. For group comparisons of demographic variables and baseline neuropsychological scores, we conducted Mann Whitney U–tests for two independent samples. Chi–square tests were used to compare gender frequency.
To assess the change from baseline to post–intervention, univariate analyses of variance (ANOVA) with repeated measures were conducted for each outcome measure, testing for the main and the interaction effects of the two–level factors intervention (intervention group or control group) and time (baseline or post–intervention). All tests were performed two–tailed, with a significance level of p < 0.05. Before entering the repeated–measures ANOVA, scores were rank–transformed across the two time points. Secondly, a rank–based inverse normal transformation (INT) [32] was used to achieve an approximately normal distribution of residuals. ANOVA analyses were conducted using data with and without INT.
As effect size, Cohen’s d was calculated for the interaction effects. Between–group differences at baseline and post–intervention, respectively, were assessed using a dependent–samples t–test, calculating effect sizes from the t–values.
RESULTS
Subjects and baseline characteristics
The screening and randomization procedure is illustrated in Fig. 1. Two patients cancelled their participation before the intervention started. During the intervention one participant became seriously ill and another patient developed paranoid delusions and was treated with antipsychotics. These participants were excluded from the analysis. The final sample included in the analysis consisted of 16 patients, of which thirteen fulfilled the criteria for probable AD and one patient the criteria for possible AD. Two patients (one in the intervention, the other in the control group) had a history of a vascular comorbidity and were diagnosed with mixed dementia. All patients had a CDR score of 1.0. 13 subjects received antidementive medication. In the control group, three subjects took donepezil, two subjects took rivastigmine, and three subjects did not take any antidementive medication. In the intervention group, three subjects took rivastigmine, four subjects took donepezil, and one subject took memantine. Regarding antidepressant medication, in the intervention group, five subjects took serotonin reuptake inhibitors (SSRI). In the control group, one patient took SSRI. All subjects treated with antidementive or antidepressive medication had a stable dose of medication at least for 6 months before the intervention started. A detailed clinical characterization of the subjects is presented in Table 1.
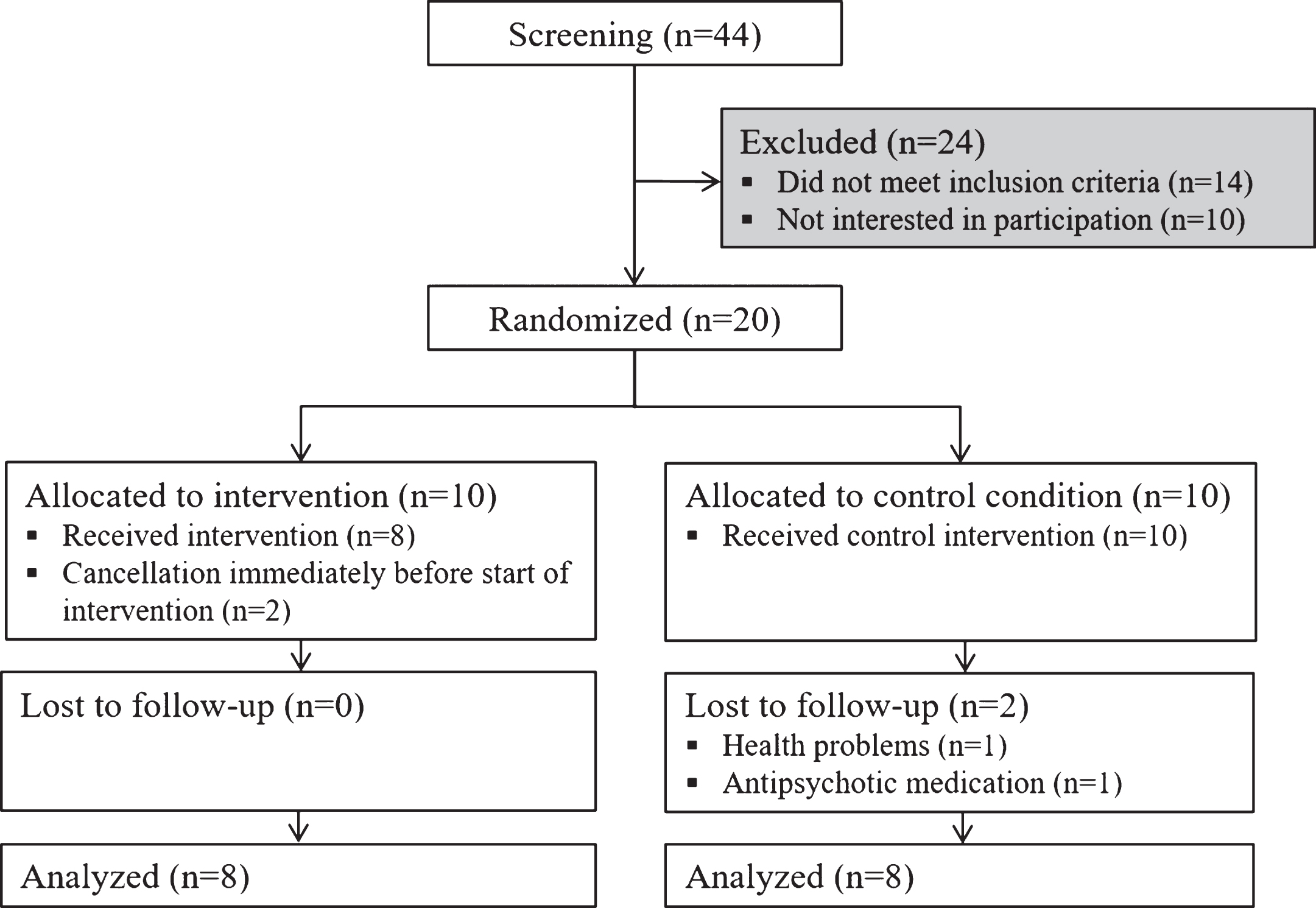
Flowchart of randomization and procedure according to the CONSORT criteria [43].
Demographic and clinical data at baseline
CG, control group; IG, intervention group; AD, Alzheimer’s dementia; VaD, vascular dementia; MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale.
The control group and the intervention group did not differ significantly in age (p = 0.916), gender (p = 0.614), education (p = 0.957), or any of the outcome variables at baseline (shown in Table 2).
Scores of outcome variables at baseline
*Higher scores indicate decreased performance, or a higher abnormality of questionnaire statements. SD, standard deviation; ADL, Activities of Daily Living; B–ADL, Bayer Activities of Daily Living Scale; NSL, Nuremberg Aging Observation Scale; RBMT, Rivermead Behavioural Memory Test; HOTAP, “Planning and organization”; HOTAP–A, “individual actions” (sorting of photos showing sequences of typical everyday actions); HOTAP–C, “semi–structured daily schedule” (fitting single actions into a pre–structured daily schedule); CTP, Boston Cookie Theft Picture Description Task; MMSE, Mini-Mental State Examination; CERAD, Consortium to establish a registry for Alzheimer’s disease; AES, Apathy Evaluation Scale; DEMQOL, Dimensions of Quality of Life; GDS, Geriatric Depression Scale; NPI, Neuropsychiatric Inventory; ZBI, Zarit Burden Inventory.
Outcome measures: Changes from baseline to post–intervention
The adherence to the treatment of the 16 patients was 100%. Table 3 shows the interaction effects based on the ANOVAs.
Baseline to post–intervention differences and interaction effects (assessed using ANOVA)
*Positive scores indicate decline from baseline to post–intervention; grey shading indicates a direction of effects as expected. SD, standard deviation; F, intervention by time; d, Cohen’s d, derived from t–values; ADL, Activities of Daily Living; B–ADL, Bayer Activities of Daily Living Scale; NSL, Nuremberg Aging Observation Scale, RBMT, Rivermead Behavioural Memory Test; HOTAP, “Planning and organization”; HOTAP–A, “individual actions” (sorting of photos showing sequences of typical everyday actions); HOTAP–C, “semi–structured daily schedule” (fitting single actions into a pre–structured daily schedule); CTP, Boston Cookie Theft Picture Description Task; MMSE, Mini-Mental State Examination; CERAD, Consortium to establish a registry for Alzheimer’s disease; AES, Apathy Evaluation Scale; DEMQOL, Dimensions of Quality of Life; GDS, Geriatric Depression Scale; NPI, Neuropsychiatric Inventory; ZBI, Zarit Burden Inventory. Bold: p < 0.05.
ADL–competence, as measured by caregiver–rating on the Bayer–ADL, increased in the intervention group over time, and decreased in the control group. However, this interaction was not significant (p = 0.109). The NSL scale showed a caregiver–rated decline of ADL–competence in both groups over time (interaction effect non–significant, p = 0.900). The NSL patient–rating scale showed a decrease in the intervention group and an increase in the control group (interaction effect non–significant, p = 0.310).
Secondary outcomes
Cognitive abilities related to daily living, as assessed by the RBMT, CTP, and HOTAP, showed no significant interaction effects (Table 3). In addition, CERAD battery scores showed no significant interactions of intervention by time. Within the non–cognitive domains, a significant interaction effect was found for the self–rated quality of life, with an increase in the intervention group and a decrease in the control group (p = 0.013). No other domains revealed significant effects. Effect sizes ranged from medium to large (Table 3). Similar results were obtained by ANOVA analyses without previous INT (data not shown).
DISCUSSION
The present study aimed to evaluate the feasibility and efficacy of a multimodal Cognitive Rehabilitation approach based on the manual–guided CORDIAL program [15], that was adapted to a group setting and expanded to include contents intended to facilitate a transfer to everyday life functioning.
We found that the adapted Cognitive Rehabilitation program was highly feasible but showed no effect on the primary outcome ADL–competence. This is in line with previous studies using short–term interventions in dementia patients (e.g., [13]). Moreover, the original CORDIAL evaluation study did not find significant changes in ADL scores, as measured by the BADL scale [33]. It has to be noted that ADL scores are difficult to assess in dementia [34], and that the BADL has been suggested to have low sensitivity in dementia [15]. Yet, when using a different ADL–scale, we did not observe a significant intervention effect either, suggesting that effects were not eliminated by a potential lack of sensitivity. Therefore, other factors may have contributed to the absence of significant improvements in ADL. Notably, the sample size was rather small. As two out of three ADL scales showed moderate to large effect size estimates (Cohen’s d > 0.5), the effects might have reached statistical significance in a larger sample.
Cognitive Rehabilitation effects need to be transferred from the therapy setting to real life. At first, transfer requires a minimum amount of preserved cognitive abilities, especially memory and the ability of abstraction, to be able to apply a strategy in different situations. The cognitive level of our patients, however, ranged from mild to mild–moderate dementia, suggesting that some participants may not have had the required cognitive resources for successful transfer. It can be speculated that Cognitive Rehabilitation benefits ADL skills especially at a mild dementia stage. Consequently, the transfer should have been increasingly supported by the therapist or the caregivers, for example by transferring the exercises to the domestic setting for patients at more advanced disease stages. To successfully achieve transfer, caregivers need to take over responsibilities in the daily setting. The frequency of caregiver’s direct participation once in four weeks was too low to achieve adequate involvement. Thus, there is a noticeable conflict of goals: on the one hand, frequent caregiver involvement is required for the Cognitive Rehabilitation to be effective; on the other hand, a higher involvement of caregivers is restricted by their limited availability and already high burden of care. A targeted program at less advanced disease stages involving caregivers may be evaluated in future Cognitive Rehabilitation studies. Additionally, successful transfer depends on well–defined personal goals. The definition of individual goals turned out to be challenging and time–consuming in our treatment group. For example, the participants tended to express global goals, such as “to feel better”, rather than specific goals. Furthermore, the intervention group rated their ADL–competence as being stable or slightly decreased (NSL) at follow–up, while the control group rated their ADL–competence as increased at follow–up. As the Cognitive Rehabilitation included a detailed analysis of the daily routine and mobility, it might have led to an increased awareness of challenges, possibly eliciting a more critical evaluation of skills.
Considering secondary outcomes, we found no effects of Cognitive Rehabilitation on cognitive abilities related to daily living. For example, we conducted the RBMT, based on its assessment of explicit daily functions. However, the RBMT includes the assessment of prospective aspects, including prospective memory [35], which deteriorate at an early stage of the disease [36]. Regarding spontaneous speech, the lower decrease in CTP scores at follow–up in the intervention group compared to the control group supports the use of communication training in future Cognitive Rehabilitation studies (Cohen’s d: –0.6, non–significant). With respect to the cognitive state measured by psychometric testing (CERAD battery), we did not expect an improvement, based on previous studies [12–14]. Studies that did find improvements in single cognitive domains [37, 38] had conducted Cognitive Rehabilitation over a longer period of time (5 months) [37], or managed to involve the caregivers to a greater extend [38]. These findings highlight the relevance of a prolonged duration of the program and of social interaction for successful transfer.
A relevant aspect to consider is the possibility of the control group benefitting more than expected from the active control condition. However, as an indirect transfer of improved cognitive functions to improved activities of daily living may not be present in dementia [3, 39], it is unlikely that this should explain the lack of effects.
In the non–cognitive domains, we found a significant interaction for quality of life with an increase in the intervention group and a decrease in the control group. This agrees with several previous studies (for a review, see [7]), but it is in contrast to the original evaluation study of the CORDIAL program [33], which found no significant effect. One could speculate that this difference reflects the advantage of a group setting over an individual setting, as other group–based interventions also found a positive impact on the quality of life [40].
Furthermore, the influence of antidementive or antidepressant medication has to be considered. We attempted to minimize this factor by only including subjects with a stable dose, and by using the differences between the two time points to assess relative change, rather than using absolute values.
Limitations of the study included a small sample size and the sample heterogeneity with respect to age and MMSE scores. Although this increases the relevance of the sample for the population of people with dementia, the high variability limits the power to detect intervention effects in addition to the small sample size. Furthermore, the assignment to the groups was only partially randomized, since five subjects stemmed from the waiting list of a previous pilot study and had been preassigned to the intervention group. Also, the duration of the intervention of only three months may have been too short for the consolidation of new strategies, however, our approach was based on an existing manual–guided program. In future studies, however, the duration could be extended.
We did not conduct interviews for a detailed qualitative data analysis. We suggest that qualitative research methods should be integrated into the evaluation of efficacy studies of Cognitive Rehabilitation approaches. However, we had the following impressions: 1) Despite a heterogeneous age range and variability in cognitive functioning, the group members shared their experiences with each other. Participants benefitted from each other’s resources and supported each other, e.g., by suggesting different coping strategies. We observed an active process of collecting and sharing ideas. 2) We extended the sessions’ durations from 1 h a week in the original CORDIAL program to 2 hours a week. However, even this period proved to be too short to address all contents in the group setting. A longer duration, including breaks, would be more favorable. 3) A variable order of modules was beneficial. For example, the analyses of problems and the resulting awareness of deficits provoked depressive symptoms and frustration in some participants, so that we chose to follow up with the biographical work (originally placed at the end of therapy) to activate individual resources. A qualitative case report of a CORDIAL trial by Tonga et al. [41] confirms the benefit of a flexible module sequence. 4) As adaptation, a problem–solving training related to daily life was included in the program. The tasks could be adjusted individually and were well accepted by the participants. However, the frequency of one session per week seemed to be too low, and no transfer effect to daily living could be observed. Thus, although implicit memory such as learning routines is better preserved than declarative memory in patients with AD dementia, a higher training frequency seems to be necessary [42]. Interestingly, however, the implementation of routines in the Cognitive Rehabilitation may be reflected in an increased functional connectivity between the posterior cingulate cortex and the cerebellum at post-intervention, as reported in an accompanying MRI study [20].
In conclusion, in our study we demonstrated the feasibility of a group–based Cognitive Rehabilitation program, adapted from the CORDIAL program for patients with mild AD [15]. As a result, we found an increased quality of life, but no improvement of ADL skills. This was mainly due to a lack of transfer between the therapy setting and daily life. We therefore recommend increased active involvement of the caregivers in future programs. Aside from that, the group context seemed to promote communicative capabilities and coping processes. However, future studies with larger sample sizes are needed for generalizing the results. Furthermore, our findings demonstrate the variety of challenges when developing Cognitive Rehabilitation approaches and contribute to the urgently required development and refinement of cognitive interventions fordementia.