
Abstract
Background:
Subjective cognitive complaints (SCCs) may be an early marker of prodromal Alzheimer’s disease.
Objectives:
Using a 10-item yes/no SCCs questionnaire (Le Questionnaire de Plainte Cognitive [QPC]), we evaluated the prevalence and distribution of SCCs in cognitively healthy Czech older adults and examined total score and specific QPC items in relation to depressive symptomology and cognitive performance.
Methods:
A sample of 340 cognitively healthy older community-dwelling volunteers aged 60 or older from the third wave of the longitudinal project National Normative Study of Cognitive Determinants of Healthy Aging, who underwent a comprehensive neuropsychological assessment and completed the QPC and the 15-item Geriatric Depression Scale (GDS-15). Regression analysis was controlled for age when GDS-15 was the outcome and for age and GDS-15 with cognitive domains as the outcome.
Results:
71% reported 1 + SCCs, with prevalence of individual complaints ranging from 4% to 40%. The number of SCCs was associated with GDS-15 (p < 0.001). Personality change (p < 0.001) and Limitation in daily activities (p = 0.002) were significantly associated with higher GDS-15 score and Spatial orientation difficulties (p = 0.019) and Impression of worse memory in comparison to peers (p = 0.012) were significantly associated with lower memory performance.
Conclusions:
We identified some cognitive complaints that were very common in our sample. Overall, a higher number of SCCs in well cognitively functioning individuals was most closely related to depressive symptomatology, while some specific complaints reflected lower memory performance and should be considered when screening for people at risk of cognitive decline.
Keywords
INTRODUCTION
Subjective cognitive complaints (SCCs) are common in older adults. In population-based studies, including both cognitively normal subjects and those with probable cognitive impairment, the prevalence of SCCs ranges from 10% to 81% [1–3]. A higher rate of SCCs is usually associated with higher age [4, 5], poorer cognitive performance [6], and a higher level of depressive symptomatology [7]. Generally, SCCs have been associated with normal aging, cognitive decline beyond normal aging, and other non-cognitive conditions such as depression and anxiety [7–9]. However, little is known about how specific SCCs may relate to each of these conditions, and this might account for some authors remaining skeptical about the importance of SCCs in preclinical stages of Alzheimer’s disease (AD) [10].
The most common cause of cognitive decline beyond normal aging is AD. The pathological changes associated with AD start decades before clinical diagnosis of cognitive impairment and biomarkers can be detected by positron emission tomography imaging of amyloid-β (Aβ), or magnetic resonance imaging of the hippocampus or cerebrospinal fluid Aβ42, together with subtle cognitive decline [11]. In early stages, highly educated subjects can compensate for the subtle cognitive decline, resulting in a normal performance on standard cognitive tests [12]. Still, using compensatory cognitive mechanisms does not prevent such individuals from self-experience of cognitive decline [13].
On the other hand, a number of cross-sectional studies found SCCs in subjects without dementia to be associated with depressive symptomatology rather than with objective cognitive status [7–9], and therefore the relevance of SCCs as a marker of cognitive decline due to neurodegeneration has been questioned by some authors [10]. However, it seems that the relationships between SCCs, objective cognition, and depressive symptomatology are much more complex. This complexity and absence of long-term longitudinal studies using biomarkers could be one of the reasons why the causal relationship between these factors remains poorly understood. It has been proposed that depressive symptoms can be an early prodrome of dementia, that depression may lead to hippocampal dysfunction similarly as AD does [10, 15], or that depressive symptoms may rather be a consequence of awareness of SCCs [16]. Nevertheless, most recent studies investigating AD biomarkers and neuroimaging markers either exclude subjects with depression, which precludes the study of the potential causal relationship, or statistically account for depressive symptoms, which may bias thefindings [17].
Other possible sources of incongruent findings among existing SCC studies are different approaches how to assess SCCs and cognition. Some studies have applied screening tools to evaluate global cognitive status [6, 18]. Only a few studies have administered complex cognitive batteries comprising traditional neuropsychological tests at a population level [2, 5]. The use of screening tools to evaluate global cognitive function could have led to an underpowering of the relationship between SCCs and cognition.
In previous studies, SCCs assessment ranged from a single question or a small number of items with varied content and unknown measurement properties to more comprehensive and validated questionnaires [19]. The differences in approaches might explain major discrepancies among studies estimating the prevalence and predictive value of SCCs in non-demented older adults. To date, there is no consensus or guidelines for instrument selection to assess SCCs. The QPC (Le Questionnaire de Plainte Cognitive; in English, Questionnaire of Cognitive Complaints) has been used to evaluate SCCs. The QPC is a relatively brief and easy to administer tool for assessing SCCs. The QPC was originally developed to help physicians in primary care identify subjects with cognitive impairment or depression and has been applied to populations of patients with mild cognitive impairment (MCI), mild to moderate dementia due to AD, and patients with depressive syndrome [20, 21]. The QPC is comprised of three types of questions that have recently been proposed as useful for differentiating between normal aging and prodromal AD [13]: 1) cognitive decline in comparison to the previous level of cognitive functioning; 2) cognitive functioning in comparison to individuals of the same age group; and 3) other specific complaints potentially specific for pathological aging or depression.
Using the Czech version of the French QPC, we aimed to evaluate the prevalence of SCCs among cognitively healthy Czech volunteers. We also assessed the distribution of SCCs according to demographic variables, such as age, education, and gender. Finally, we aimed to study the relation of the number of SCCs reported in QPC and specific SCCs in relation to depressive symptomology and cognitiveperformance.
Based on previous findings, we hypothesized that the number of complaints would increase with age and that higher number of complaints would be associated with more depressive symptoms and lower cognitive performance. We also expected to find specific complaints linked to cognitive functioning (especially memory) and depressivesymptomatology.
MATERIALS AND METHODS
Participants
Data from this study are derived from the third wave of the longitudinal project National Normative Study of Cognitive Determinants of Healthy Aging (NANOK), which includes a volunteer sample of community-dwelling adults aged 60 or older living in the Czech Republic [22]. The current study included 340 NANOK members in whom the absence of cognitive impairment was ascertained.
To ensure as representative a sample as possible, the participants were recruited from various areas, including the capital city and smaller towns and villages in 12 regions (out of 14). Participants were recruited to the longitudinal project of healthy aging through advertisements on the institutional website, local media, at post offices, general practitioners’, and organizations for seniors. Assessment near the place of living and monetary remuneration (200 CZK) was offered to participants [22]. All participants in this study had signed written, informed consent that was approved by a local ethics committee. The procedures were in accordance with the Helsinki Declaration of 1975 and later revisionin 2000.
General exclusion criteria for NANOK were diagnosis/treatment for a cognitive impairment of any kind or a serious neurological disorder (e.g., Parkinsonism, epilepsy), an acute phase of serious mental disorder (e.g., major depressive disorder), current radiotherapeutic or chemotherapeutic treatment, history of stroke, traumatic brain injury, and alcohol or substance abuse. At baseline, only participants with intact activities of daily living, with the absence of dementia, and absence of significant cognitive complaints raising suspicion of organically caused cognitive impairment (based on an initial comprehensive interview with a psychologist) were included. The participants then underwent a comprehensive neuropsychological examination, and those with performance worse than minus 2 standard deviations from the mean of the group in two cognitive scores or in one cognitive score plus a Functional Activities Questionnaire or Geriatric Depression Scale (GDS) score of≥10 were excluded.
The remaining participants were followed and retested once per year. Participants diagnosed with cognitive impairment were excluded from the study sample. Our questionnaire was administered in the third year of the study, so only participants remaining without a diagnosis of cognitive impairment during three one-year follow-ups were included.
For this study, we applied further criteria to exclude participant with possible cognitive dysfunction. Cognitive dysfunction was established when: 1) participants scored worse than the 5th percentile according to Czech age- and education- norms on the Mini-Mental State Examination (MMSE); 2) participants scored worse than minus 2 standard deviations according to age- and education-adjusted norms in either the Rey Auditory Verbal Learning Test, trials 1–5 sum (RAVLT 1-5), Trail Making Test B (TMT-B), or phonemic verbal fluency (letters N, K, P) tests; and (3) participants scored 1.5 standard deviations or worse below the mean of age- and education-adjusted norms on at least two scores in RAVLT 1-5, TMT-B, and/or phonemic verbal fluency (letters N, K, P). Also, participants with major depressive symptoms (scoring >10 on GDS, 15-item version) were not included.
MEASURES
Neuropsychological assessment
All participants underwent a complex neuropsychological battery that included measures of global cognitive functioning (MMSE [23]), attention (TMT-A [24], and Prague Stroop test - dots [25]), memory (RAVLT [26], and Free and Cued Selective Reminding Test with Immediate Recall [27]), executive function (TMT-B [24], and Prague Stroop test - color [25]), and language (categorical verbal fluency - animals; phonemic verbal fluency - letters N, K, P [28]). Each participant was also administered a self-report 15-item version of the GDS (GDS-15 [29]) to evaluate the severity of affective symptoms.
Measurement of SCCs: QPC
All participants were administered the Czech version of the QPC, which was based on an original French 10-item yes/no questionnaire assessing the presence of cognitive difficulties in the last six months [20, 21]. The Czech version was made based on a translation from French to Czech by an experienced translator, followed by a back-translation from Czech to French by a translator blinded to the original French version. The discrepancies were consulted and based on the consensus between the two translations the final version was developed to preserve the original meaning as accurately as possible. For the purpose of the publication, the QPC was translated into English in cooperation with a native English speaker and the final English version was approved by the author of the questionnaire.
The first two items inquire about general memory abilities, while the remaining eight items inquire about more particular cognitive complaints with a focus on memory. The items also cover difficulties with spatial orientation, language, instrumental activities, or personality change. The exact wording of all items is presented in Fig. 1. For each item, we indicate a key name for ease in reporting findings.
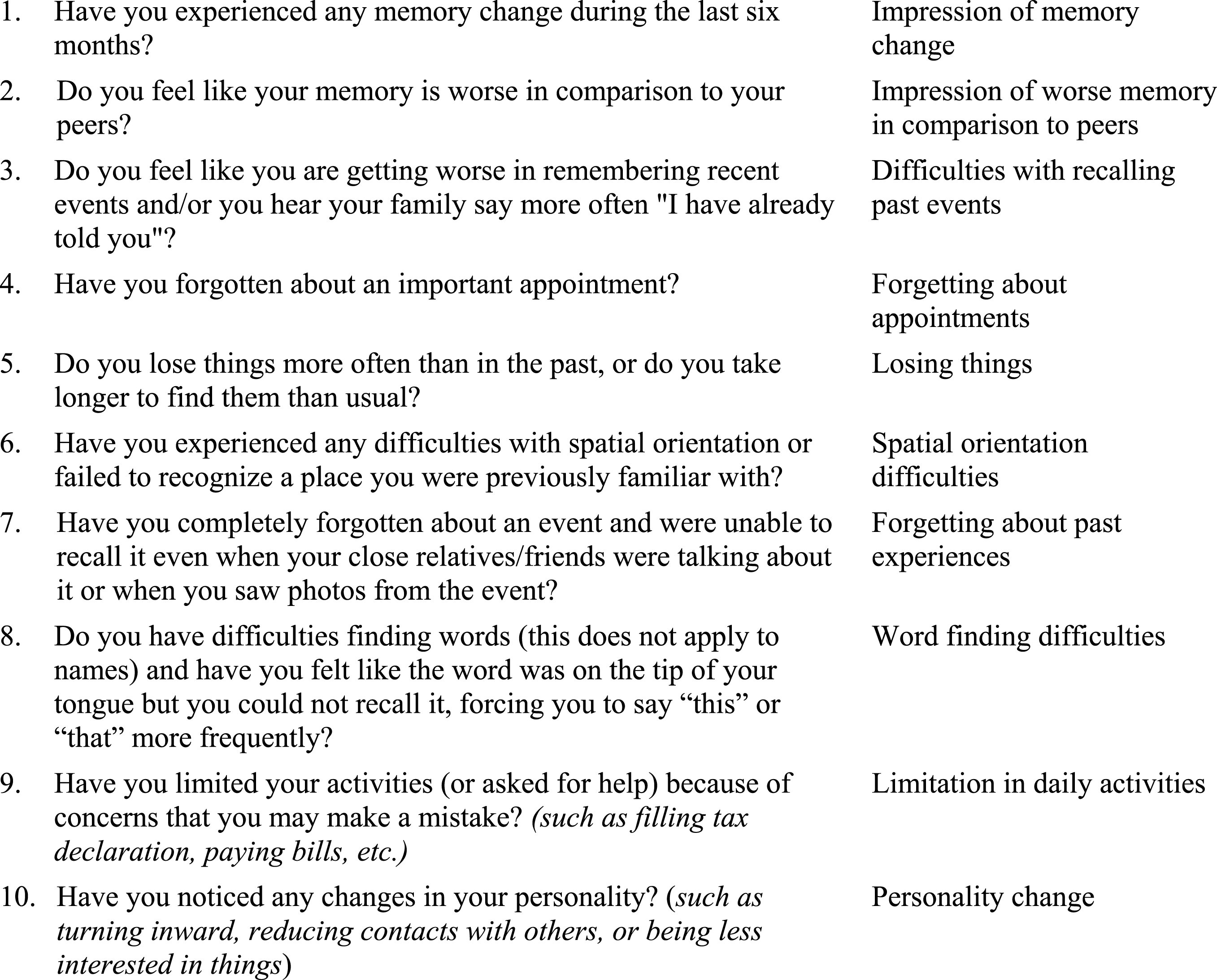
QPC, Questionnaire of cognitive complaints. Exact phrasing and key names. Questions are related to last six months.
Statistical analyses
The number of SCCs, scored from 0 (no SCC) to 5 (5 + SCCs), was the main independent variable. We capped counting SCCs at 5 due to extremely small counts past 5 SCC and to prevent bias due to outliers. Analyses of variance with post-hoc tests performed using the Tukey’s Honestly Significant Differences test was used to describe differences in study variables by the number of SCCs (Table 1). The main results were obtained from ordinary least squares (OLS) regression with SCCs (Table 2a, b) and the individual complaints (Table 3) as the independent variables. The regression estimates express the amount of change in a cognitive z-score in relation to reporting one additional SCC. When depressive symptomology was the dependent variable, OLS regression analysis was controlled for age; when any cognitive composite score was the dependent variable, OLS regression analysis was controlled for age (Table 2a) and for age and depressive symptomatology (Table 2b). The level of significance was set at p < 0.05. A non-parametric Spearman correlation was performed to describe the strength of the association between age and the number of SCCs. The Holm-Bonferroni correction was used to control for multiple comparisons (Table 2a, b). Effect size Cohen’s d was calculated using means adjusted for age and reflects the average effect size across the number of SCCs. Cognitive scores were transformed into z-scores (using sample mean and standard deviation) to allow for an easier comparison of results across the cognitive outcomes. Cognitive composite z-score of memory, attention, executive function and language were calculated as the averages of z-score of administered neuropsychological tests for each cognitive domain. Because the measure of depressive symptomology (GDS-15) was not normally distributed, it was log transformed before main analyses.
Sample characteristics presented for the entire sample and by the number of cognitive complaints
*p < 0.05, p values are based on analyses of variance with post-hoc tests performed using the Tukey’s Honestly Significant Differences test; to go along with study hypotheses, we only report mean level differences relative to those reporting no complaints; SD, standard deviation; GDS-15, Geriatric Depression Scale, 15-item version; MMSE, Mini-Mental State Examination; RAVLT 1-5, Rey Auditory Verbal Learning Test, sum of trial 1-5; FCSRT, total recall of Free and Cued Selective Reminding Test Immediate Recall; TMT, Trail Making Test; C-VF, categorical verbal fluency, animals; P-VF, phonemic verbal fluency, letters N, K, P.
The association between the number of cognitive complaints and depressive symptomatology, global cognitive functioning, and cognitive domains without controlling for depressive symptomatology
p values are based on regression analyses where the number complaints (0–5+) was the independent variable; analyses were controlled for age; †scores are represented as z-scores; aGDS-15, which was positively skewed, was log transformed before analyses; Est, parameter estimate; H-B Correction, Holm-Bonferroni Correction for multiple comparisons; GDS-15, Geriatric Depression Scale, 15-item version.
The association between the number of cognitive complaints and global cognitive functioning, and cognitive domains controlled for depressive symptomatology
p values are based on regression analyses where the number complaints (0–5+) was the independent variable; analyses were controlled for age and depressive symptomatology; †scores are represented as z-scores; Est, parameter estimate; H-B Correction, Holm-Bonferroni Correction for multiple comparisons; GDS-15, Geriatric Depression Scale, 15-item version.
The associations between specific SCCs and depressive symptomatology, global cognitive functioning, and cognitive domains
*p < 0.05, **p < 0.01, ***p < 0.001, p values are based on regression analyses where the individual complaint was the independent variable; analyses were controlled for age and depressive symptomatology; Est, parameter estimate; GDS-15, Geriatric Depression Scale, 15-item version; †scores are represented as z-scores.
RESULTS
Sample characteristics and prevalence of SCCs
Sample characteristics including neuropsychological characteristics and prevalence of SCCs are presented in detail in Table 1. The mean age for the whole study sample was 75±8.5 years, and average education was 13±3.4 years. Male (45%) and female participants were proportionally represented in the sample. In all, 71% of participants reported at least one SCC, almost one-half of participants (47%) reported two or more SCCs, and one-fourth (25%) of participants reported three or more SCCs. The non-parametric Spearman correlation resulted in a weak but statistically significant positive relationship between number of SCCs and age (ρ= 0.19, p < 0.001). There were no differences in years of education or in gender distribution by the number of SCCs.
Number of cognitive complaints in relation to depressive symptoms and cognition
A number of depressive symptoms on GDS-15 were significantly associated with the number of SCCs after adjusting for age (Estimate = 0.30, p < 0.001); this association remained significant after the Holm-Bonferroni correction for multiple comparisons (Table 2a). The average effect size, expressed as Cohen’s d, across the levels of cognitive complaints, was 0.43, or about a medium effect. In comparison, the corresponding effect size for age was0.15.
More SCCs were associated with a worse MMSE score (Estimate = –0.09, p = 0.008), worse memory (Estimate = –0.11, p = 0.002), and worse language (Estimate = –0.07, p = 0.037) when adjusting only for age and not for depressive symptomatology. The association between number of SCCs and MMSE score and memory remained significant after the Holm-Bonferroni correction for multiple comparisons (Table 2a). After adjusting for age and depressive symptoms, more SCCs were associated with worse memory (Estimate = –0.09, p = 0.022) and attention performance (Estimate = –0.08, p = 0.045), but these associations were reduced to non-significant after the Holm-Bonferroni correction for multiple comparisons; the number of SCCs was not related to executive function or language (Table 2b).
Specific complaints and their association to depressive symptoms and cognition
Of the ten SCCs included in the QPC, Word finding difficulties was the most common complaint (reported by 40%), followed by Difficulties with recalling past events (32%) and Impression of memory change (29%). Limitation in daily activities and Impression of worse memory in comparison to peers were other quite common complaints (reported by 14% and 12%, respectively). By contrast, Spatial orientation difficulties and Losing things were reported only by 4% and 7% participants, respectively.
There were two specific complaints identified that were linked to depressive symptomatology when adjusting for age. A positive answer to Personality change was associated with an increase of 2.63 points in the GDS-15 score (Estimate = 2.63, p < 0.001) and a positive answer to Limitation in daily activities with a 0.91 point increase (Estimate = 0.91, p = 0.002).
After adjusting for age and GDS-15 score, we identified complaints specifically linked to cognitive performance; these are presented according to the strength of association. Positive answer to Spatial orientation difficulties was linked to a lower MMSE score (by 0.70 standard deviation units [SD]) and lower memory performance (by 0.28 SD) (Estimate = –0.70, p = 0.012; Estimate = –0.28, p = 0.019, respectively). Word finding difficulties was linked to higher MMSE score and lower attention and executive function (Estimate = 0.38, p < 0.001; Estimate = –0.28, p = 0.003; Estimate = –0.25, p = 0.005; respectively). Difficulties with recalling past events was associated with lower attention (Estimate = –0.20, p = 0.049) and Impression of worse memory in comparison to peers with lower memory performance (Estimate = –0.18, p = 0.012). Limitation in daily activities, which was primarily associated with higher depressive symptomology, was also linked to lower executive performance when adjusted for GDS-15 (Estimate = –0.39, p = 0.002).
The remaining complaints were not associated with cognition or depressive symptomology (Impression of memory change, Forgetting about appointments, Forgetting about past experiences, and Losing things).
DISCUSSION
Using the QPC, we found a high prevalence of SCCs in a volunteer sample of Czech cognitively healthy older adults. SCC levels gradually increased with higher level of depressive symptomatology. There was an association between higher number of complaints and lower memory and global cognitive function when not controlling for depressive symptomatology. Two SCCs were significantly related to lower memory performance (Spatial orientation difficulties and Impression of worse memory in comparison to peers). Another two SCCs were related to higher level of depressive symptomatology (Limitation in daily activities and Personality change). Interestingly, none of the three most common SCCs (Word finding difficulties, Difficulties with recalling past events, and Impression of memory change) were related to lower memory performance or higher level of depressive symptomatology.
The reported prevalence of SCCs in older adults ranges from 10% to 81% [1–3]. This broad range underscores the difficulty of reliably estimating the prevalence of SCCs. In our study, prevalence of at least one SCC was 71% and prevalence of individual specific complaints ranged from 4% to 40%.
The majority of existing studies report a higher rate of SCCs with advancing age [30, 31], which is congruent with results of our correlation analysis. We have not found any association between years of education and the number of SCCs, which agrees with the previous study using the QPC [21]. Several community-based studies have reported a negative association between level of education and severity of SCCs in older adults, indicating an increasing the number of SCCs with lower formal education [5, 32]. In clinically-based studies the presence of subjective memory complaints is usually associated with a higher level of education [33]. We assume that the specificity of QPC complaints together with low variability in years of education of participants could explain why no education effects were demonstrated. Because of the absence of a significant education effect, education was not subsequently included in main analyses exploring the relationship between SCCs, depressive symptomatology, and cognition.
Previous findings about the association between gender and SCCs are incongruent. Some community-based studies reported a higher rate of SCCs to be associated with female gender [32, 34]. Other studies including the previous one that used the QPC did not find any effect of gender on the number of SCCs [21, 35], which is congruent with our findings. The previous studies included different SCC items. It is possible that some SCCs are more likely to be endorsed by women which could be one explanation for the inconsistency in findings.
The level of depressive symptomatology (measured by GDS-15) was the best indicator of SCCs, as reported on the QPC. This is consistent with findings of several previous studies [2, 18]. Although the overall percentage of elderly people with depressive disorder might seem low (between 1% and 5% of individuals aged 65 or older [36, 37]), the number of elderly individuals exhibiting minor individual depressive symptoms not meeting the criteria for major depressive disorder is much higher, ranging from 15% to 25% [38]. Depressed older adults often display cognitive complaints and somatic symptoms rather than affective symptoms [39]. Some of these cognitive complaints are even included in the GDS-15: “Do you feel you have more problems with memory than most people?” (compared with Impression of worse memory in comparison to peers), and “Have you dropped many of your activities and interests?” (compared with Limitation in daily activities). However, to our knowledge, no study has investigated individual items of the GDS-15 or any other depression scale in relation to individual SCC items. We identified two specific complaints related to higher GDS-15 score (Limitation in daily activities and Personality change). The latter was additionally related to lower executive performance, which often coexists with late-life depression (LLD), as shown previously [40]. Interestingly, in the previous study using the QPC [21], the two most common SCCs in participants with clinically manifested depression syndrome were different (Difficulties with recalling past events and Word finding difficulties). However, the sample with depression in that study differs from the study sample used here. Participants included in the current study were free of a clinical diagnosis of depression and reported only minor individual depressive symptoms in the GDS-15.
The relationship between SCCs and objective cognitive performance has been a matter of controversy. Several previous cross-sectional studies showed an association between SCCs and objective cognitive performance [6, 41], while others did not [3, 7]. The two studies without significant findings used only screening tools to measure cognitive performance, which could fail to reveal subtle cognitive changes and result in low variability of performance in the study sample, and thus the potential association between SCCs and cognition may be hidden by a stronger relation between SCCs and depression. In addition, in a community-based study [3], participants were classified as complainers or non-complainers based on a single question about memory. This simple classification could mislead the results. In our study applying a comprehensive neuropsychological battery and a SCC questionnaire, we have found a statistically significant association between higher number of SCCs and lower MMSE and memory performance. Interestingly, this relation became nonsignificant when controlling for depressive symptomatology.
The interpretation of these results should take into account the presumed complex relationship between depression, SCCs, and cognition. We propose three possibilities: 1) the depressive symptomatology can lead to lower cognitive performance, which may trigger the SCCs [40]; 2) the minor individual depressive symptoms in cognitively healthy older adults aretriggered by their awareness of cognitive capacity decline not captured by the cross-sectional cognitive testing [16]; or 3) both the depressive symptomatology and the subtle cognitive impairment can be a direct concomitant consequence of early neuropathological changes in AD [42, 43]. Therefore, we cannot interpret the decrease in relation between the SCCs and cognition, after adjustment for depression, as depression causing the SCCs.
Another source of the weak association of SCCs and cognition could lie in the discrepancy between the subjective and objective type of data, as proposed by a recent review [13]. SCCs, in general, refer to longitudinal change, whereas cross-sectional neuropsychological testing describes the cognitive capacity at a single time point, which may not be sensitive enough to capture a possible intraindividual cognitive change. In such cases, the subjective report does not correlate well with objective performance.
Specific complaints should be taken into account when trying to identify associations between SCCs and cognition. In our sample, poor memory was associated with two specific SCCs: Impression of worse memory in comparison to peers and Spatial orientation difficulties. This is congruent with former findings [6, 44].
Impression of worse memory in comparison peers has been considered a feature that increases the likelihood of preclinical AD and should raise concerns [13, 20]. In a previous study using the QPC, this complaint was commonly reported by patients with AD dementia (41.8%), but not by cognitively normal subjects. Spatial orientation difficulties was additionally associated with the lower MMSE score and was the rarest complaint in our sample. This is in agreement with the findings of previous studies. Amariglio et al. [6] also reported Spatial orientation difficulties as the rarest complaint, but associated with impaired memory and language. In a previous study using the QPC [21], no cognitively normal individual reported this difficulty, however, it was present in subjects with AD dementia. The early presence of spatial orientation impairment has already been observed [45] but probably is not usually detected when using standard neuropsychological methods. According to some recent findings, spatial navigation may be an independent cognitive domain which was not assessed in our study [46]. Based on our results, subjectively reported difficulties with spatial orientation in otherwise cognitively normal elderly should be heeded.
A previous population study which also included subjects with cognitive impairment [6] has shown a positive association between two memory complaints (difficulties in remembering recent events, experience of change in memory) and poor memory performance. Interestingly, in our sample of cognitively normal older adults, these two common memory complaints did not relate to memory. It has been postulated that during the course of AD, objective intraindividual change in memory precedes objective memory impairment [13]. From this point of view, subjective feeling of memory change may demonstrate subtle memory decline not captured by standard memory tests in a cross-sectional study. In our sample, Impression of memory change was reported by almost one-third of cognitively healthy older adults. With respect to its high prevalence, this complaint does not seem to be particularly specific for pathological aging. Still, further research in a clinical setting is needed.
The three remaining complaints, Losing things, Forgetting about appointments, and Forgetting about past experiences, were rarely reported and were not related to cognition. We assume that these complaints do not appear until advanced stages of cognitive deficit, which may explain our findings. Also, in a previous study using the QPC [21], these difficulties were reported by an insignificant number of controls in contrast to subjects with AD dementia.
Our current study is one of a few European projects with an ethnically homogeneous study sample. To overcome the limitations of previous studies, we applied a validated questionnaire for assessing SCCs and administered a complex cognitive battery that covered all cognitive domains for evaluation of cognitive performance. There are still several limitations that should be considered in the interpretation of the current results.
When recruiting cognitively healthy older participants for the study of healthy aging, intact activities of daily living and the absence of significant cognitive concerns were the basic inclusion criteria. These are also two of the core criteria of the revised Petersen’s criteria for MCI [47]. However, it is likely that when using a different approach to define cognitive impairment, as was recently proposed in the literature (e.g., [48]), participants with early cognitive deficit might have been included. Although we demonstrated associations between specific complaints and lower objective cognitive performance in this sample, these findings are not easily transferred to the clinical setting. As such, our findings should be confirmed in a future longitudinal study. Further research of specific complaints in patients with MCI and those meeting criteria for subjective cognitive decline [13] is needed.
In conclusion, cognitive complaints in cognitively healthy older adults are common. A higher number of SCCs in these well cognitively functioning individuals appears to be most closely related to depressive symptomatology, and this may hide a more subtle association between the number of SCCs and cognition. However, the causal relationship of SCCs and depressive symptoms needs further clarification, so the possible pathological significance of the SCCs in individuals with depressive symptoms should not be diminished.
Our findings support the notion that some complaints are part of normal aging while others could be specific for non-normative cognitive decline and should raise concerns. Therefore, when looking for early signs of prodromal AD, inquiring about specific cognitive complaints seems to be more relevant. Typical complaints may differ during the course of the disease. Therefore, the specific complaints rarely reported in our cognitively normal sample may be common in subjects with developed objective cognitive impairment. Using the QPC may help identify subjects that will need further neuropsychiatric examination.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Charles University in Prague, project GA UK No 135215, by European Regional Development Fund— Project FNUSA-ICRC (No. CZ.1.05/1.1.00/02.0123) and by project ICRC-ERA-HumanBridge (No. 316345), by the project no. LQ1605 from the National Program of Sustainability II (MEYS CR), by the project National Institute of Mental Health (NIMHCZ), under grant number ED2.1.00/03.0078, by the project Sustainability for the National Institute of Mental Health, under grant number LO1611, with a financial support from the Ministry of Education, Youth and Sports of the Czech Republic under the NPU I program, and by the Ministry of Health of the Czech Republic, project AZV 16-27611A.