
Abstract
INTRODUCTION
Dementia with Lewy bodies (DLB) is the second most common degenerative dementia subtype following Alzheimer’s disease (AD) [1], but it remains under-recognized [2]. DLB is characterized by progressive dementia accompanied by one or more core features, i.e., fluctuations in cognition, visual hallucinations, and spontaneous features of parkinsonism, and supportive features such as rapid eye movement sleep behavioral disorder, reduced uptake on dopamine transporter imaging, and neuroleptic hypersensitivity. Due to the complex clinical profile, DLB patients can present to a range of different medical services like psychiatry, neurology, memory, sleep, and geriatric medicine clinics, and thus recruitment of sufficient numbers of DLB patients for observational or intervention trials can be difficult.
There are few longitudinal studies of DLB, and thus the disease course is unknown. Most single-center studies indicate that DLB patients suffer from higher mortality [3], shorter time to nursing home admission [4], caregiver burden [5], and use more resources than those with AD of similar severity [1]. No large longitudinal cohort-study of the rate of cognitive decline in DLB exists. Early observations [6] suggested that DLB patients had a faster cognitive decline as compared to AD, but later studies have reported contradictory results. In a recent systematic review [7] including 18 longitudinal DLB studies, the six studies based on the Mini-Mental State Examination (MMSE), we found that DLB had a more rapid decline than AD, a more rapid decline in AD, or no difference. The meta-analysis showed no significant difference between DLB and AD in the rate of decline on MMSE. However, these studies were small, with the largest study included only 65 DLB patients.
The main aim of the current study, based on patients from the European Consortium for DLB(E-DLB), was to describe the rate and clinicalpredictors of cognitive decline over three years in a large multicenter cohort of DLB, and to compare this with the decline in AD and Parkinson’s disease dementia (PDD) patients.
METHODS
Study design
Longitudinal data from a multicenter cohort of patients who were diagnosed with probable DLB from a new pan-European consortium on DLB were analyzed. The consortium consists of 19 European and one US centers that agreed to share clinical data on patients with DLB, as well as PDD and AD.
The patients were referrals to outpatient clinics including memory, movement disorders, geriatric medicine, psychiatric, and neurology clinics. From a total database of 2,085 patients, longitudinal cognitive data, i.e., at least one MMSE score after baseline assessment, were available for 1,290 patients from 17 centers (835 DLB, 198 PDD, and 257 AD patients) (Table 1).
Characteristics of the three patient groups
Data are expressed as mean±SD for continuous variables, and as n (%) for categorical variable. MMSE, Mini-Mental State Examination; N, number; DLB, dementia with Lewy bodies; PDD, Parkinson’s disease dementia; AD, Alzheimer’s disease; ChEI, cholinesterase inhibitor.
The number of included patients at each center is shown in Supplementary Table 1. Due to the naturalistic multicenter design, there were differences in the follow-up procedures. Not all patients were followed, and the follow-up time varied among those who were followed up. Similarly, at most but not all centers, patients started treatment with a cholinesterase inhibitor after baseline assessment. The details are provided in the flowchart (Fig. 1).

Flowchart of patients at baseline and follow-up. DLB, dementia with Lewy bodies; PDD, Parkinson’s disease with dementia; AD, Alzheimer’s disease; On therapy, treated with cholinesterase inhibitors; RBD, REM-sleep behavioral disorder.
Diagnostic and clinical examination
The diagnoses were made according to the most recent international consensus criteria for probable DLB [8], PDD (MDS consensus criteria), and AD (ICD 10) by the treating physician, a group of at least two expert clinicians, or by a multidisciplinary team at a consensus diagnostic meeting on the basis of all available clinical and diagnostic test data.
Per design, the clinical procedures were not harmonized across centers, but a detailed history and clinical examinations, including physical, neurological, and psychiatric, were performed by a licensed specialist on all patients. Centers were requested to record whether patients fulfilled criteria for parkinsonism (84%), visual hallucinations (64.7%), and fluctuating cognition (72.9%) as specified in the consensus criteria [8], based on all available information (data missing for 160–240 DLB patients). Cholinesterase inhibitors were used by 674 (69.2%) (data missing for 316 patients). Routine blood tests and brain imaging were performed, and often also neuropsychological tests. Results of dopamine transporter SPECT scans were available for 188 DLB patients, and 147 (78.2%) of these had an abnormal scan. At all participating centers, cognitive screening was performed using the MMSE [9]. Patients with acute delirium or terminal illness, those recently diagnosed with a major somatic illness, and patients with previous psychotic or bipolar disorders were excluded from the study.
Ethics
The local ethics committee at the individual center have approved the inclusion of data in this study. The patients gave their written consent to use the unidentified results of their clinical, instrumental, and laboratory investigations for research purposes.
Statistics
The statistical analyses were done using IBM SPSS version 20 and R Project for Statistical Computing [10]. Results are shown as mean±SD for continuous variables, and number and percentage for categorical variables. Comparisons of baseline clinical and demographic data in the three groups were performed using one-way ANOVA or chi square test as appropriate. Analyses with linear mixed effect (LME) models were used to determine the rate of cognitive decline measured by MMSE during the 3-year follow up in the three groups. The large number of data assures asymptotic normality of the test statistics used in the analyses.
The impact on decline is represented by the interaction term between factor and time (year of follow up). One of the LME analyses did not use baseline MMSE as response but instead used its tertiles as an adjusting covariate. There is considerable individual variation in both level and decline of MMSE, therefore LME models with both random intercept and random slope at individual and center level were used for the analysis. In the figures, there are some seemingly systematic discrepancies between empirical averages at each follow-up and the results of the LME analyses. This is not indication of misfit, but is caused by random effects modeling and the estimation procedure. On statistical bases (likelihood ratio tests), differences between centers need to be modeled as random effects, since focus is on common population decline rates and not center differences. The random effect of centers causes the deviations in level. Differences between individuals are also modeled with random effects and population level and rate are estimated using (restricted) maximum likelihood (ML). The empirical means are influenced by drop out. If there is a tendency for patients with low MMSE to drop out, the mean MMSE for the remainders will increase. This would be Drop Out At Random (DAR). In this situation, the ML estimation of the LME model shows the expected development of individuals if they did not drop out. This explains the differences in rates between trajectories of empirical means and model estimated lines.
RESULTS
The baseline characteristics of the three groups are presented in Table 1. There were significant differences between the three groups for gender, duration of symptoms, and antidementia treatment status, but not for baseline MMSE or age. Comparisons of baseline data in the three groups with follow-up were performed.
Post-hoc analyses on gender were in PDD versus AD and DLB versus AD: p < 0.001 and in DLB versus PDD: non-significant. The analysis on duration in DLB versus AD: p = 0.023; PDD versus AD: p = 0.001, DLB versus PDD: non-significant and the results on cholinesterase inhibitors therapy were in PDD versus AD: p < 0.001; PDD versus DLB: p < 0.001, and in AD versus DLB: p = 0.015.
Decline on MMSE
All three groups declined during the 3-year follow-up period (Fig. 2). Based on the LME analysis, the annual decline on MMSE score was 2.1 points in DLB, compared to 1.63 in AD and 1.75 in PDD. The differences between groups were not significant, although there was a trend toward significant difference between DLB and AD (p = 0.0693).
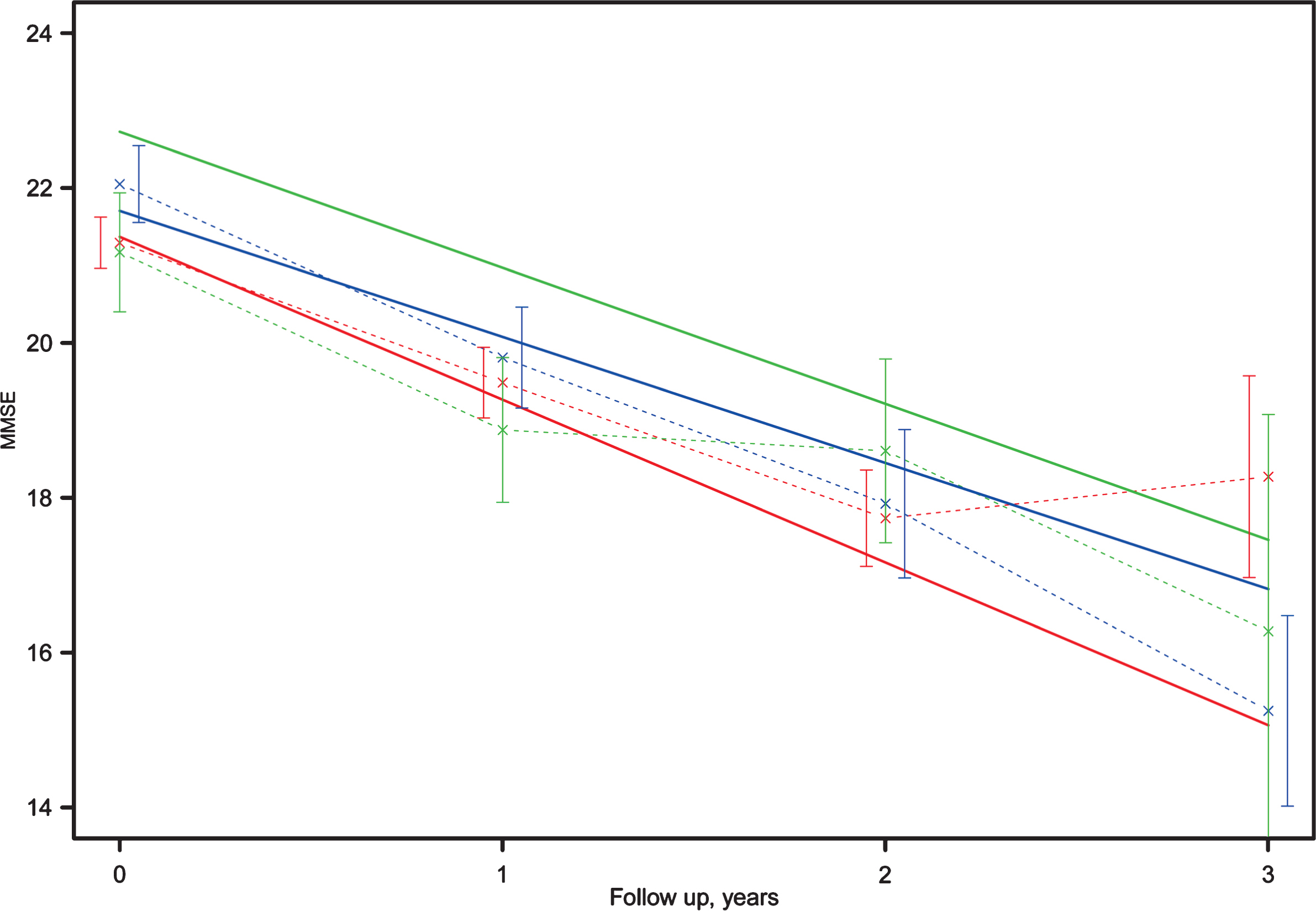
Decline on the MMSE in DLB, AD, and PDD over 3 years. Dashed lines and × show data averages at baseline, one, two, and three years for the groups DLB (red), PDD (green), and AD (blue). Vertical lines depict 95% CIs around the averages. The solid lines show the model-estimated development for the groups DLB (red), PDD (green), and AD (blue). MMSE, Mini-Mental State Examination; DLB, dementia with Lewy bodies; PDD, Parkinson’s disease with dementia; AD, Alzheimer’s disease.
A number of sub-group analyses were performed due to the wide variations in the rate of annual decline, in particular in the DLB group, where the 95% confidence interval for the standard deviations of annual decline was 3.67 to 4.05, compared 3.33 to 4.06 in PDD, and somewhat narrower in AD (2.96, 3.52). Of note, 18% of patients had a higher MMSE score after two years compared to baseline. Since the diagnosis of patients who improve during two years may be less certain, even on treatment, the analyses were performed including only those with declining or stable MMSE score at the two-year follow-up. The results were similar to those in the total group (Supplementary Figure 1). There was no significant interaction between gender and rate of decline (p = 0.0855), with men having a somewhat more rapid decline than women.
There were also wide variations in the baseline MMSE scores, range 2–30. To control for a possible floor-effect, the analyses were performed after excluding those with severe dementia (i.e., MMSE ≤10 (n = 37). The results were similar as the analyses of the total group (data not shown). To explore in more detail how rate of decline was associated with baseline dementia severity, patients were grouped according to baseline MMSE tertiles and an LME analysis using these tertiles as covariate was run. This restated the different decline rates in the diagnosis groups, but it did not give any indication of additional dependence of rates on baseline tertiles (p = 0.964) (Fig. 3). In this analysis, including baseline MMSE tertile as a co-factor, the annual rate of decline in DLB was significantly more rapid in DLB (2.59), compared to AD (1.71, p = 0.0271) and PDD (1.46, p = 0.0062). Similarly, the rate of decline of DLB patients with an abnormal scan (n = 147), was significantly more rapid compared to AD (p = 0.0025) and PDD (p = 0.0004) (Fig. 4). When we included only those patients with two or more follow-up analyses, the rate of decline in DLB patients (2.1 points per year) remained higher than that of the AD group (1.4). Finally, there were no significant effects of gender on the rate of decline in the three groups (F = 0.3, p = 0.09) (Fig. 5).
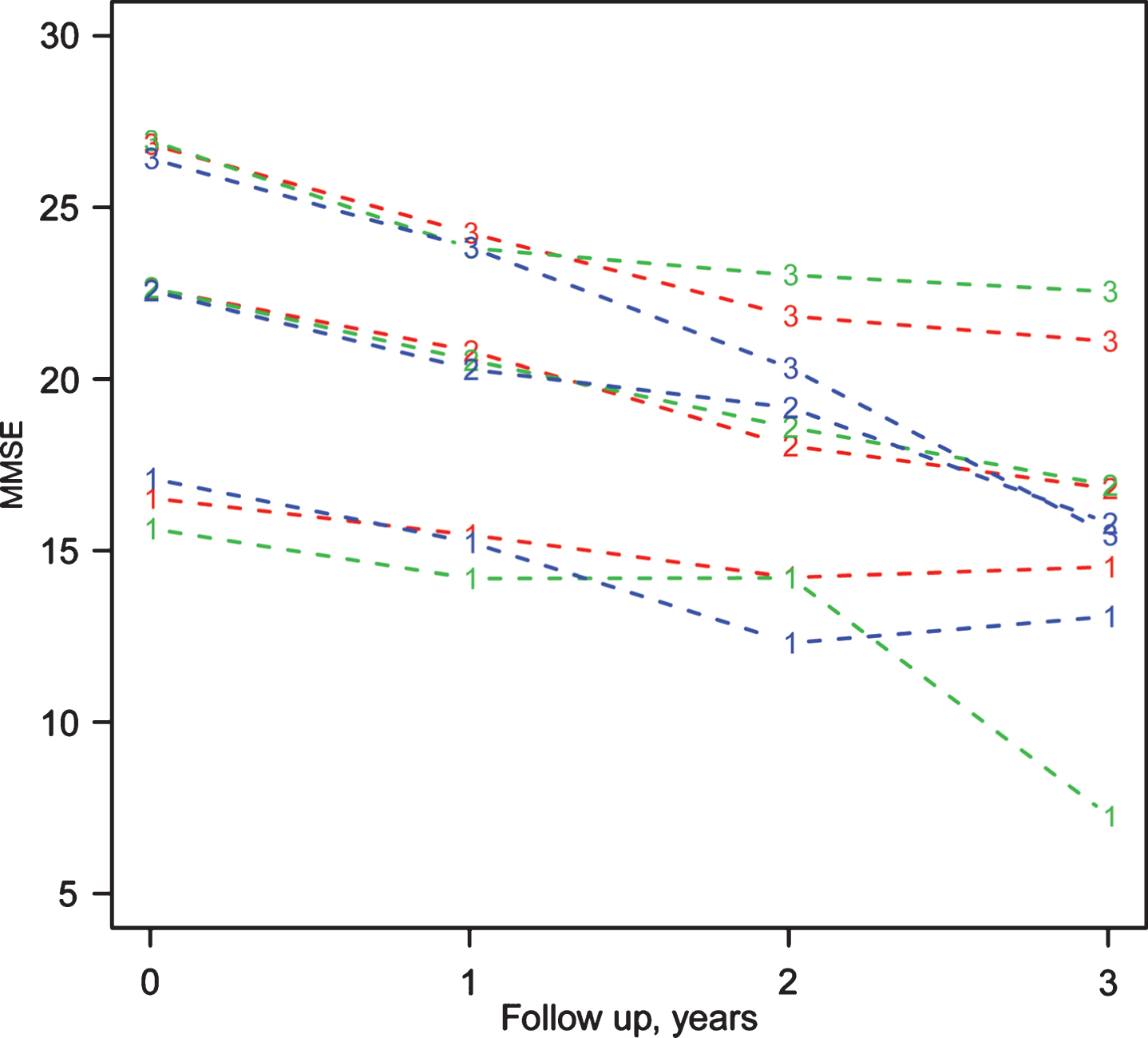
Rate of MMSE decline according to baseline MMSE tertile. Rate of MMSE decline according to baseline MMSE tertile for the groups DLB (red), PDD (green), and AD (blue). MMSE, Mini-Mental State Examination; DLB, dementia with Lewy bodies; PDD, Parkinson’s disease with dementia; AD, Alzheimer’s disease. 1, 2, and 3 denotes the lowest, middle, and highest tertiles, respectively. Follow up 0 = baseline, 1 etc. are follow-up evaluation after 1, 2, and 3 years.
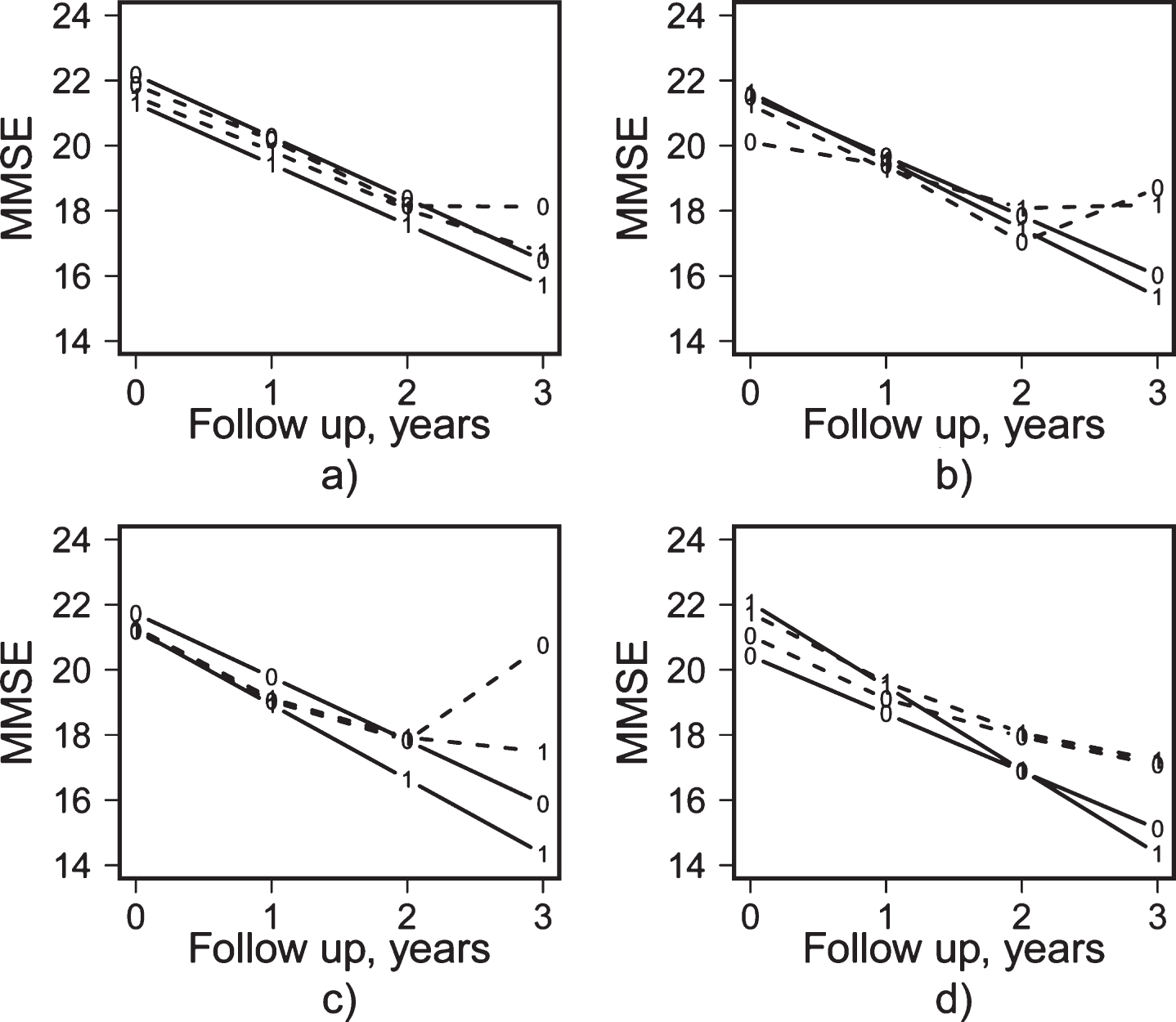
Rate of decline in DLB according to core features and dopamine transporter scan. DLB follow up data at 0, 1, 2, and 3 years divided into the two groups according to presence of a) vishal (visual hallucinations) (0 = no, 1 = yes); b) Parkinson (signs of parkinsonism) (0 = no, 1 = yes); c) cognfluct (cognitive fluctuation) (0 = no, 1 = yes); d) dat scan done (0 = no, 1 = yes); averages at stapled lines. Solid lines show results from an LME analysis. DLB, dementia with Lewy bodies; MMSE, Mini-Mental State Examination.
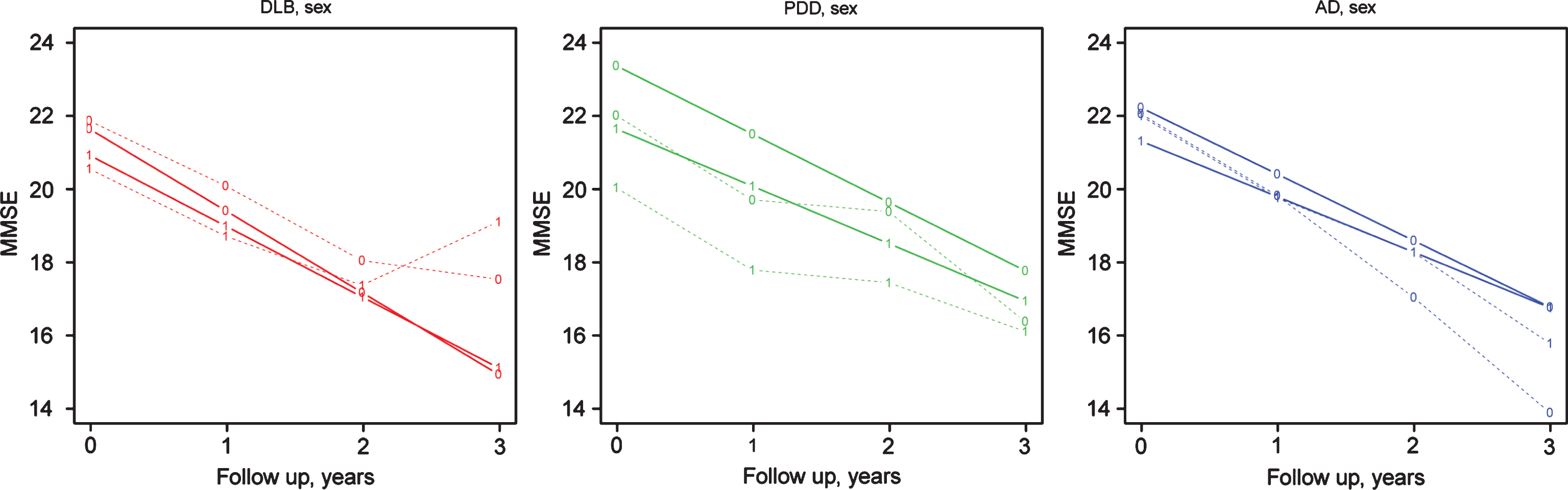
Rate of decline in diagnostic groups according to sex. Data averages at baseline, one, two and three years for the groups DLB (red), PDD (green), and AD (blue) separated by sex (0-male, 1-female). The solid lines show the model estimated development for the respective group. MMSE, Mini-Mental State Examination, DLB, dementia with Lewy bodies; PDD, Parkinson’s disease with dementia; AD, Alzheimer’s disease.
In order to control for a potential bias by treatment, we compared only those patients who received treatment. The findings are similar to those in the overall analyses of the total group (Supplementary Figure 2). Finally, there were no significant associations between presence of core features at baseline and rate of cognitive decline in the DLB group, i.e., the presence or absence of visual hallucinations, parkinsonism, or cognitive fluctuations was not associated with the rate of decline on MMSE (Fig. 4).
DISCUSSION
This is the largest longitudinal study of patients with probable DLB. We found that although in the main analysis the difference in rate of decline between the groups did not reach significance, some of the sub-analyses indicated that the decline was more rapid in DLB compared to AD and PDD, with a difference of approximately 0.5–0.8 point on the MMSE per year.
Previous smaller single-center studies have shown inconsistent results, and in a recent meta-analysis based on six small studies, we did not find differences in the rate of decline on MMSE between DLB and AD [7]. However, a recent single-center study with 67 patients followed for up to 5 years, also included in this study, found a more rapid decline in DLB than in AD of approximately 1 point per year, supporting the current findings [11]. We are not aware of longitudinal studies comparing the rate of cognitive decline in DLB and PDD, and thus our findings of a similar rate of decline in DLB and PDD is novel, and in line with other evidence of similar clinical and pathological features in DLB and PDD.
The underlying mechanisms of cognitive decline and progression in DLB are poorly understood, but it is likely that both the cortical Lewy body and the Alzheimer-type pathology, which occurs in most DLB patients, contribute. Evidence from some autopsy studies suggest that the combination of pathologies causes a more rapid decline [12, 13] and for high CSF tau to be associated with shorter survival in DLB [14–16]. The indication of more rapid decline in DLB compared to AD and PDD is consistent with this, since most DLB patients have higher levels of combined pathology compared to AD and PDD.
Although the participating centers specialized in the diagnosis and care of patients with DLB, using the same diagnostic criteria, a main limitation of this study is the lack of harmonized clinical procedures. The main outcome, cognitive decline, was, however, measured using the MMSE in all patients.
Although the MMSE is likely less sensitive to the early executive and visuospatial impairments in early DLB than other instruments such as Montreal Cognitive Assessment (MoCA) [17], we [18] and others [19] have found that the MMSE is as sensitive to change in DLB and PD as the MoCA. A limitation of MMSE and other screening instruments is that they track global decline, and thus possible differences in the decline of different cognitive domains cannot be assessed with such scales but require detailed neurocognitive assessments.
This is a naturalistic study and thus there were differences in the clinical management, including treatment. Most, but not all, patients started treatment with cholinesterase inhibitors, which are effective in DLB and PDD [20] and thus differences in the treatment may influence the comparison between groups. However, the findings remained similar when only treated were included.
Another limitation is that data on treatment and core features were missing in many DLB patients. The number of patients at each assessment declined with time, in particular from year 2 to year 3. Although this was partly due to the retrospective design, i.e., patients were not entered in a prospective longitudinal study protocol; we cannot exclude the possibility of selective attrition due to more rapid decline, which may have influenced the findings.
Diagnosis was clinical, made by specialists in dementia or movement disorders with a special interest in DLB. There is therefore a risk for misdiagnosis; both over- and under-diagnosis of DLB has been shown [21–23], and DLB can be misdiagnosed as both AD and PDD. Dopamine transporter imaging was available to support the diagnosis, although cannot distinguish between DLB and PD, but only in a subgroup of patients, and the longitudinal design likely increases the accuracy of diagnosis, since other diseases masking as DLB may be revealed with time. Thus, we believe the diagnoses are fairly accurate. Pathological verification would have provided important evidence of the diagnostic accuracy but is difficult to perform in a large multicenter study. A larger proportion with dopamine transporter imaging, and more detailed tests of motor, cognitive, and behavioral changes would have potentially improved diagnostic accuracy [24].
The variability in rates of decline complicates the interpretation of the findings. We therefore performed a number of sub-group analyses to explore this in more detail. The variation was particularly large in DLB, and when baseline MMSE score was included as a co-factor, the decline in DLB was significantly more rapid than in AD and PDD. Furthermore, the finding of a more rapid decline in the small subgroup of DLB patients with an abnormal DAT-scan supports the hypothesis of a more rapid decline in DLB, since in this group the diagnosis of DLB is likely to be very accurate. The presence of DLB core features at baseline did not influence rate of decline. Gender was not significantly associated with the rate of decline, although there was a trend towards more rapid decline in male DLB patients.
The main strength of this study is the large number of patients included, with more than 800 DLB patients with longitudinal data, which ensures sufficient statistical power. This is particularly important in DLB given the cognitive fluctuations and wide variation in course. In addition, the multicenter design, with centers all over Europe represented, suggests that the cohort is representative of the European DLB population, and also ensures recruitment from a variety of specialties, suggesting that most DLB subgroups were included. On the other hand, since patients were recruited from tertiary care centers, more atypical or more severe cases may be overrepresented in the cohort.
To conclude, we found indications of a more rapid cognitive decline in DLB compared to AD and PDD. The difference in cognitive decline between DLB and AD was small however, and thus the more severe prognosis related to nursing home admission and carer burden reported in DLB is likely related more to the many non-motor symptoms, which commonly occur in DLB. There are large individual variations in the rate of decline and future studies based on the E-DLB cohort will explore the effect of potential clinical and biomarker predictors.
Footnotes
ACKNOWLEDGMENTS
The authors would like to express their thanks to all the members of the E-DLB consortium: Angelo Antonini, Center for Parkinson’s disease and Movement Disorder Venice-Lido, Italy; Bradly Boeve, Mayo Clinic Rochester, USA; Richard Dodel, University Hospital Marburg, Germany; Gert J. Geurtsen, AMC Amsterdam, The Netherlands; Oskar Hansson, Lund University, Sweden; Zoe Katsarou, Aristotle University of Thessaloniki, Greece; Arvid Rongve, Haugesund Hospital, Norway; Per Svenningsson, Karolinska Institutet, Sweden; John Paul Taylor, Newcastle University, UK; Latchezar Traykov, University Hospital “Alexandrovska”, Bulgaria; Eric Westman, Karolinska Institutet, Sweden; Henrik Zetterberg, University of Gothenburg, Sweden.
The project was partly funded by the EU Joint program for neurodegenerative diseases.