
Abstract
Cerebrovascular deposition of amyloid-β, known as cerebral amyloid angiopathy (CAA), is associated with MRI findings of lobar hemorrhage, cerebral microbleeds, and cortical superficial siderosis. Although pathological studies suggest that tau may co-localize with vascular amyloid, this has not yet been investigated in CAA in vivo. Three patients with probable CAA underwent 11C-Pittsburgh Compound B (PiB) PET or 18F-florbetaben PET to evaluate amyloid burden, and 18F-AV-1451 PET to evaluate paired helical filament tau burden. Regions that had cerebral microbleeds or cortical superficial siderosis largely overlapped with those showing increased 18F-AV-1451. Our preliminary study raised the possibility that lobar cerebral microbleeds, and cortical superficial siderosis, which are characteristic markers of vascular amyloid, may be associated with local production of paired helical filament tau.
INTRODUCTION
Cerebral amyloid angiopathy (CAA) is a condition in which amyloid-β protein accumulates in the walls of small cortical and leptomeningeal arterioles and arteries [1]. Although definite CAA must be confirmed pathologically, the Boston clinical radiological criteria allow the diagnosis of CAA non-invasively with high specificity and sensitivity in patients with intracerebral hemorrhage [2]. Strictly lobar cerebral microbleeds (CMBs) or cortical superficial siderosis (cSS) are also radiologic markers of CAA [3, 4]. Previous studies showed that cerebrovascular amyloid can be detected by amyloid imaging studies using 11C-Pittsburgh Compound B (PiB)-PET [5, 6].
Recent advances in in vivo tau imaging have led to a new era in neurodegenerative disease research. 18F-AV-1451 binds to paired helical filament tau, and has provided valuable data on the distribution of tau in Alzheimer’s disease [7, 8]. However, the relationship between lobar CMB and cSS with tau in CAA patients has not been defined. Previous reports suggest that abnormally phosphorylated tau is more abundant around amyloid-β laden arteries than blood vessels without amyloid-β [9–11]. We tested the hypothesis that CAA patients would have greater tau deposition in regions of lobar CMB and cSS using brain MRI, 18F-AV-1451-PET, and PiB-PET.
METHODS
Subjects
We recruited three patients who had strictly multiple lobar CMBs or cSS, indicating a diagnosis of probable CAA according to the Boston criteria (Table 1) [2, 12]. One patient (Case 1) was newly recruited from the memory clinic at Samsung Medical Center and two patients (Case 2 and 3) were selected from our previous cohort of 251 cognitively impaired patients who underwent PiB PET imaging from July 2007 to July 2011 [13]. Of these 251 patients, 11 met our criteria for strictly multiple lobar CMB or cSS and two of these were available for 18F-AV-1451 PET imaging.
Demographic characteristics of patients with probable cerebral amyloid angiopathy
APOE, apolipoprotein E; cSS, cortical superficial siderosis; PET, positron emission tomography; PiB, Pittsburgh compound B; MCI, mild cognitive impairment.
All three patients underwent neuropsychological tests using a standardized neuropsychological battery [14]. Two patients (Case 1 and 2) had multiple domain amnestic mild cognitive impairment and one patient (Case 3) had an amnestic-type dementia.
This study was approved by the Institutional Review Board of Samsung Medical Center and the methods were carried out in accordance with the approved guidelines. We obtained informed consent from all participants.
Assessment of cerebral microbleeds and cortical superficial siderosis on MRI
All participants underwent brain MRI. T2, T2*, T1, FLAIR, and T2 Fast Field Echo MR images were acquired at Samsung Medical Center using the same 3.0T MRI scanner (Philips 3.0T Achieva). CMBs were defined as homogenous, round lesions with signal loss (≤10 mm in diameter) on T2*-weighted images [15]. Strictly lobar CMBs were defined as microbleeds restricted exclusively to lobar locations. cSS was defined as linear hypointensities on T2*-weighted images consistent with chronic blood residues in the superficial layers of the cerebral cortex [16].
Amyloid PET acquisition
Patients underwent 18F-florbetaben PET (Case 1) or 11C-PiB-PET (Case 2 and 3) at Samsung Medical Center using a Discovery STe PET/CT scanner (GE Medical Systems, Milwaukee, WI, USA) in a three-dimensional scanning mode that examined 47 slices of 3.3 mm thickness spanning the entire brain. CT images were acquired using a 16-slice helical CT (140 KeV, 80 mA; 3.75 mm section width) for attenuation correction. For 18F-florbetaben-PET, a 20-min emission PET scan with dynamic mode (consisting of 4×5 min frames) was performed 90 min after injection of 381 MBq 18F-florbetaben. For 11C-PiB PET, a 30-min emission static PET scan was performed 60 min after injection of 584 (Case 2) or 356 (Case 3) MBq 11C-PiB. Three-dimensional PET images were reconstructed in a 128×128×48 matrix with 2×2×3.27 mm voxel size using the ordered-subsets expectation maximization (OSEM) algorithm (11C-PiB PET, iteration = 2 and subset = 20; 18F-florbetaben, iteration = 4 and subset = 20).
18F-AV-1451 PET acquisition
All three patients underwent 18F-AV-1451 PET at Gangnam Severance Hospital using a Biograph mCT PET/CT scanner (Siemens Medical Solutions, Malvern, PA, USA). At 80 min after intravenous bolus injections of 238, 272, and 272 MBq 18F-AV-1451 for Case 1, 2, and 3, respectively, tau PET images were acquired for 20 min. Prior to the PET scan, we applied a head holder to minimize head motion and acquired brain CT images for attenuation correction. Three-dimensional PET images were reconstructed in a 256×256×223 matrix with 1.591×1.591×1 mm voxel size using the OSEM algorithm (iteration = 6 and subset = 16).
PET data analysis
PET images were co-registered to individual MRIs, which were normalized to a T1-weighted MRI template. We applied normalized parameters to transform co-registered PET images into the MRI template. Standardized uptake value ratios (SUVR) were calculated using cerebellar gray matter as a reference region. SUVR greater than 1.5 are displayed in color. We defined amyloid PET to be positive when the global PiB SUVR was greater than 1.5 or when visual assessment of florbetaben PET was scored as 2 or 3 on the brain amyloid-β plaque load (BAPL) scoring system [17]. Data processing was performed using SPM version 8 (SPM8) through Matlab 2014b (MathWorks, Natick, MA, USA).
The correspondence of sites of CMBs/cSS and 18F-AV-1451 uptake was visually assessed. Furthermore, to quantitatively analyze the relationships between CMB/cSS, AV-1451 SUVR, and PiB SUVR, we parcellated the cerebral cortex into 8 regions (frontal lobe, parietal lobe, temporal lobe, and occipital lobe in each hemisphere). We then classified each lobe into lobes ‘with’ or ‘without’ CMB or cSS and compared the regional SUVR between the lobes with CMB or cSS and lobes on the other hemisphere of CMB or cSS.
RESULTS
In all three patients, the regions with CMBs or cSS largely overlapped with regions that showed increased 18F-AV-1451 uptake. The first case had multiple CMBs in the left parietal and temporal areas, which largely overlapped with 18F-AV-1451 uptake (Fig. 1). Florbetaben PET was positive as the BAPL score was 2 by visual assessment. The second case showed asymmetric multiple CMBs in the left temporal area, corresponding to the area of high PiB uptake. Asymmetric high 18F-AV-1451 uptake was observed in the inferior temporal area, parallel to the area of CMB or cSS identified by T2* weighted images (Fig. 1). The third case showed asymmetric CMB or cSS in the right parietal, occipital, and temporal areas, also co-localizing with high PiB uptake. Although high 18F-AV-1451 uptake was observed in the bilateral parietal, occipital, and temporal areas, there was preferential uptake on the right side, where CMBs or cSS were identified. More detailed images of each patient are shown in Supplementary Figures 1–3.
Quantitative analyses showed that lobes with CMB or cSS had higher regional AV1451 uptake compared to lobes on the other hemisphere of CMB or cSS (Fig. 2A). However, in this small case series, the relationship between CMB or cSS and PiB SUVR (Fig. 2B) or between the hemispheric ratios between regional PiB SUVR and regional AV1451 SUVR were not significant (Fig. 2C).
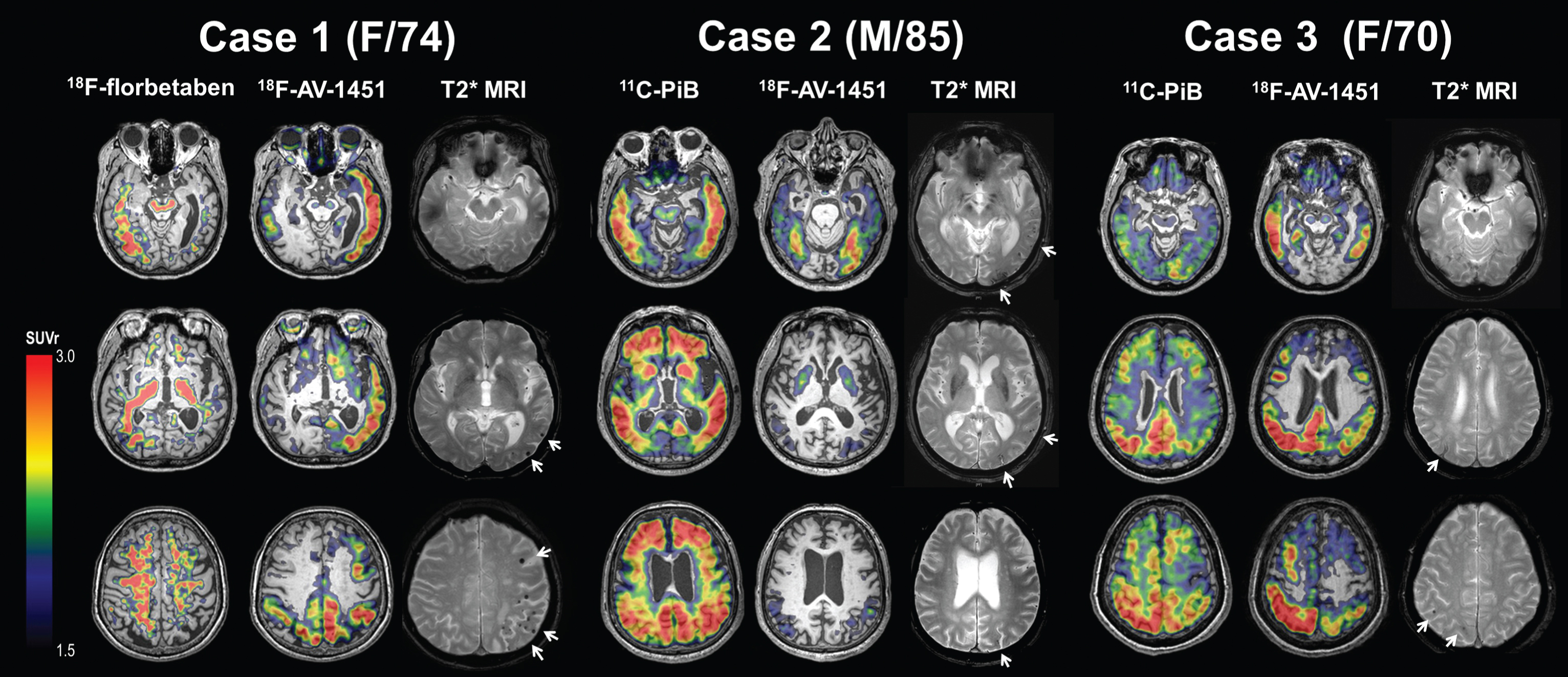
Amyloid PET, tau PET, and T2* MR images of probable CAA patients. PiB, Pittsburgh compound B; CAA, cerebral amyloid angiopathy; SUVR, standardized uptake value ratio.
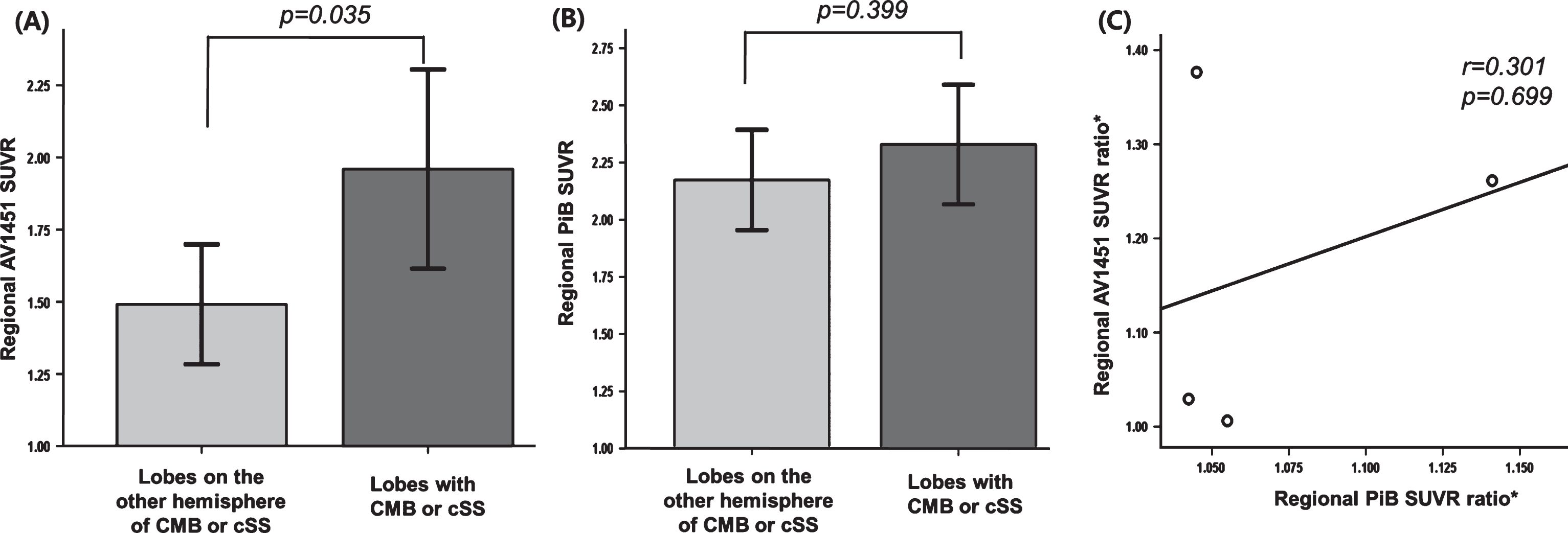
Relationships between CMB or cSS and AV1451 SUVR (A), CMB or cSS and PiB SUVR (B), and PiB SUVR and AV1451 SUVR (C). *SUVR ratio, SUVR of each lobe with CMB or cSS / SUVR of each lobe on the other hemisphere.
DISCUSSION
We report the imaging findings of three patients with multiple lobar CMBs or cSS, indicating probable CAA: One patient had left hemispheric dominant distribution of CMBs, while the other two patients had a posterior distribution of CMBs. We found that lobes with CMB or cSS had higher regional AV1451 uptake compared to lobes on the other hemisphere of CMB or cSS. Our preliminary study raised the possibility that lobar CMB and cSS, which are characteristic markers of vascular amyloid, may be associated with increased AV1451 uptake which represents paired helical filament tau.
Our suggestion that CAA is associated with tau can be explained by several aspects. First, this association is in line with previous pathology studies [9–11, 19]. Immunohistochemical studies have shown that tau immunopositive neurites cluster around cortical arteries that are affected by amyloid angiopathy [9, 10], suggesting that peri-vascular accumulation of hyperphosphorylated tau may result from elevated levels of soluble amyloid-β1 - 40 around cortical arteries and arterioles [9]. Our hypothesis that lobar CMB or cSS (indicating CAA) are related to local accumulation or production of tau is supported by a CSF biomarker study showing that patients with clinically probable CAA had higher total-tau and phosphorylated-tau compared to controls [20]. However, a recent in vitro study found no autoradiographic binding of 18F-AV-1451 in CAA or cSS lesions containing hemosiderin deposits [21]. We suspect that this discrepancy might be related to differences in binding conditions (in vivo versus in vitro autoradiographic binding). Second, as previous reports have suggested that the integrity of the blood-brain barrier is disrupted in CAA patients [22], the high 18F-AV-1451 uptake around CMB or cSS might be due to the leakage of ligands through the disrupted blood-brain barrier. Third, it is possible that these patients may also have combined Alzheimer’s disease as the patients were all cognitively impaired and were amyloid PET positive [23]. One might argue that, as tau pathology in Alzheimer’s disease and CAA both predominates posteriorly, the topographical correlation between 18F-AV-1451 uptake and CMB or cSS may reflect a mere coincidence rather than direct relationship. However, our quantitative analysis showed that AV1451 uptake was asymmetrically increased on the side where there was more CMB or cSS, which is not a common distribution of AV1451 uptake in Alzheimer’s disease. Finally, tau may exist in relation to rapidly progressive neurodegeneration, eventually resulting in axonal degeneration, rather than being specifically related to CAA [24].
We found that the distribution of PiB uptake in Cases 2 and 3 largely overlapped with CMBs or cSS in posterior brain regions. However, in the quantitative analysis CMB or cSS did not show significant relationship with regional PiB SUVR. It is possible that underlying Alzheimer’s disease pathology such as neuritic plaques might have overshadowed the effects of CAA on amyloid PET. In addition, the low statistical power might be due to the small sample size. In contrast, there was no increase in 18F-florbetaben uptake in the left hemisphere in Case 1, where there were many CMBs. Therefore, we cannot exclude the possibility that, despite meeting criteria for probable CAA, CMB or cSS are due to other pathologies such as vasculitis, subclinical trauma, or frontotemporal lobar degeneration. Alternatively, low 18F-florbetaben uptake could be due to the use of different amyloid tracers. Further amyloid PET imaging studies in a larger sample size using different amyloid tracers are needed.
Our study has several limitations. First, we did not have pathological confirmation of CAA in the three patients. Second, the use of different amyloid tracers might have affected the relationships between tau or CMB with amyloid. Third, the overlapping regions between CMB or cSS and 18F-AV-1451 uptake were based on visual assessment or crude correlation within each lobe. Lastly, since our patients were all cognitively impaired and might as well have Alzheimer’s disease, our findings have limited generalizability and one should be cautious when interpreting our data. To address the direct relationship between tau and CMB or cSS, studies on cognitively normal individuals with probable CAA are necessary to minimize the possibility of having Alzheimer’s disease. Further studies with a larger sample size would allow quantitative analysis to confirm our findings. Nevertheless, our findings raised the possibility that lobar CMB or cSS, which are characteristic markers of vascular amyloid, may be associated with local production of paired helical filament tau.
Footnotes
ACKNOWLEDGMENTS
This research was supported by National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (NRF-2015R1C1A2A01 053281); the Brain Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (2016M3C7A1913844); and Korea Ministry of Environment (MOE) as the Environmental Health Action Program (2014001360002).