
Abstract
Keywords
INTRODUCTION
Functional disability associated with dementia is a significant economic problem that negatively impacts the patient, caregiver, and health care system [1]. In fact, impairment in activities of daily living (ADLs) is a diagnostic requirement for Alzheimer’s dementia (AD) [2], whereas individuals with mild cognitive impairment (MCI) should not be dependent in daily functioning [3]. As a result, ADL impairment is one of the criteria used to differentiate AD from its prodromal stages. Nevertheless, recent research now suggests that although independence should be overall maintained, mild impairment in instrumental ADLs (IADLs) may occur in individuals withMCI [4].
In recent years, there has also been an increased focus on understanding potential gender differences in persons with MCI, AD, and related dementias [5]. Although women in this population tend to show worse cognitive ability [6, 7], gender differences in everyday functioning (ADLs) remain understudied, with the limited existing data showing inconsistent evidence for gender differences. A prior cross-sectional study has shown that in mild to moderate AD, men appear to be at a significantly higher risk for functional disability on the Disability Assessment for Dementia, despite greater verbal memory ability and more years of education [8]. Furthermore, a study examining gender differences in MCI found that men showed greater IADL impairment on cognitively demanding activities [9].
Inconsistent with these studies, longitudinal analyses of individuals with MCI found that women declined at a significantly faster rate over eight years of follow-up on the Clinical Dementia Rating Scale Sum of Boxes (CDR-SB) [6]. In addition to these discrepancies, one study found that functioning on the CDR-SB appears to predict conversion from MCI to AD in men [10], whereas another study found that scores on IADLs better predicted conversion to dementia in women [11].
One explanation for some of these mixed findings may be the fact that the CDR-SB is a combined measure of cognition and functioning; therefore, scores from this instrument may be measuring a construct that differs slightly from purer measures of functioning [12]. Furthermore, several studies have hypothesized that gender differences in IADL involvement (e.g., cooking, cleaning, shopping) may explain some of the differences between men and women in terms of functional disability [8, 13]. However, to our knowledge, no study to date as empirically examined the potential mediating influence of such experience in terms of gender differences or functional decline in general.
The present study introduces the novel construct of functional reserve and defines it as the protective influence of participating in IADLs throughout life, which may then guard against neurodegenerative functional decline. We operationalized this construct using IADL experience as a proxy. The purpose of this study is to examine how men and women with MCI differ in terms of functional dependence and to investigate whether IADL experience may influence this relationship by potentially contributing to an underlying functional reserve. Furthermore, we speculate on the potential cognitive and physical mechanisms that may underlie functional reserve and recommend avenues for future research needed to validate this hypothesis.
METHODS
Data were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu; accessed on June 24, 2016). The ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The primary goal of ADNI has been to test whether serial magnetic resonance imaging (MRI), positron emission tomography, other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of MCI and early AD. For up-to-date information, see http://www.adni-info.org.
ADNI was conducted according to the Good Clinical Practice guidelines, the Declaration of Helsinki, US 21 CFR Part 50 – Protection of Human Subjects, and Part 56 – Institutional Review Boards, and pursuant to state and federal regulations. Written informed consent was obtained from all participants and/or authorized representatives and the studypartners.
Participants
Of the 1,737 participants enrolled in ADNI-1, ADNI-GO, and ADNI-2 at the time of this study, only individuals with a baseline diagnosis of MCI and complete Functional Activities Questionnaire (FAQ) data were included (n = 862). Detailed information about inclusion and exclusion criteria across ADNI phases can be found within the procedures manuals [14]. Of this sample, baseline data were missing for apolipoprotein E-ɛ4 (APOE4) status (n = 3), Rey Auditory Verbal Learning Test (AVLT) delay recognition (n = 1), Trails B/A ratio (n = 13), Boston Naming Test (BNT; n = 3), resulting in a final sample size of 843 (341 women, 502 men).
Measures
Activities of daily living assessment
The FAQ is a 10-item assessment tool [15] that is administered to the participant’s study partner to assess experience and dependency in different IADLs. The items included on the FAQ are (1) managing finances; (2) assembling important forms; (3) shopping alone; (4) participating in a hobby or game of skill; (5) preparing a hot beverage; (6) preparing a balanced meal; (7) keeping track of current events; (8) watching/understanding TV, books, or magazines; (9) remembering appointment or important events; and (10) travelling out of the neighborhood. Each IADL item is scored from 0 to 3 : 0 = normal; 1 = remains independent with some difficulty; 2 = currently requires assistance; 3 = currently dependent; 0 = never did but could do now; and 1 = never did and would have difficulty now. These scores are summed to provide a total score ranging from 0 to 30 with higher scores indicating greater dependency. IADL experience was quantified as the number of IADL items scored as “normal”, “remains independent with some difficulty”, “currently requires assistance” or “currently dependent”, providing a score from 0 to 10 with higher scores indicating past experience on a greater number of IADLs.
Neuropsychological test measures
Of interest were measures of memory (delayed recall and delayed recognition on the AVLT and delayed recall on Story A from the Logical Memory [LM-II]); executive functioning (Trails B/A ratio), and language (i.e., BNT total correct and Categorical Fluency total animals correct). Raw test scores were used in all analyses. See the ADNI protocol manual for full details on neuropsychological, neuropsychiatric, and functional test measures [14].
Measure of depression
Existing research suggests that depression is predictive of decline in IADLs [16]. As such, depressive symptoms were rated using the Geriatric Depression Scale (GDS).
Statistical analysis
Statistical analyses were conducted using SPSS (Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Bivariate comparisons of men and women at baseline were conducted using independent t-tests, Mann-Whitney U, and Pearson Chi square. Variables that violated the assumption of normality were offset and log transformed (total FAQ, IADL experience, Trails B/A, and BNT). Negatively skewed variables were reflected before and after transformation (IADL experience and BNT).
Firstly, data were analyzed using a four-block hierarchical linear regression, predicting total FAQ score. Block 1 was classified as Demographic Factors (gender [0 = women, 1 = men], age at baseline, education, and APOE4 status [0 = no ɛ4 alleles, 1 = one or two ɛ4 alleles]); Block 2 as Depressive Symptoms (GDS score); Block 3 as Cognition (AVLT delay recall, AVLT delay recognition, LM-II delay recall, Trails B/A, Categorical Fluency, BNT); and Block 4 as Functional Reserve (IADL experience). Multivariate outliers were removed if the Mahalanobis distance was significant at p < 0.001 (n = 1). The assumption of multicollinearity was assessed using variance inflation factors, which was not violated for any variable.
In order to see the relative contribution of these variables within each gender, the regression models were reanalyzed separately for men and women. This approach allows for easy interpretation of the variance accounted for in men and women; however, stratification does not allow for these regression coefficients to be directly compared. As a result, a final regression was conducted, with significant variables from these stratified regressions (i.e., GDS, AVLT delay recall, AVLT delay recognition, LM-II delay recall, and IADL Experience) entered as interactions with gender within a fifth block. To meet the assumption of multicollinearity, these variables were mean-centered prior to creating the interaction terms.
RESULTS
Bivariate comparisons are summarized in Table 1. Women were significantly younger, had higher scores on the AVLT delay recall, higher scores on the FAQ, and had greater IADL experience. However, women also had fewer years of education, higher scores on the GDS, lower scores on the LM-II delay recall, and lower scores on the BNT. There were no significant gender differences in APOE4 status, MMSE scores, AVLT delay recognition, Trails B/A, or CategoryFluency.
Baseline characteristics with men and women compared using independent samples t-test, Mann-Whitney U, or Pearson Chi Square
All normally distributed data are presented as mean±SD and compared using t-tests. aPresented as median±IQR and compared using Mann-Whitney U due to non-normality. bPresented as n (%) positive and compared using Pearson Chi Square.
Regression results are reported in Table 2. Hierarchical regression revealed that at Block 1, Demographic Factors significantly predicted total FAQ (F(4,837) = 6.43, p < 0.001) and accounted for 3% of the variation in FAQ score. Including Depression in the regression model explained an added 1.4% (F(1,836) = 12.06, p < 0.001), and adding Cognition explained an additional 12.4% (F(6,830) = 20.57, p < 0.001). Finally, including Functional Reserve accounted for 4.8% of the variation in FAQ total score, above and beyond the other explanatory variables with a significant R2 of F(1,829) = 51.01, p < 0.001.
Summary of hierarchical regression analysis for variables predicting total FAQ score (log transformed) in MCI
N = 842; *p < 0.05, **p < 0.01, ***p < 0.001. aVariable log transformed due to non-normality. bLarger values indicate greater impairment.
Although the effect size was small, gender was significantly associated with total FAQ above and beyond the other demographic variables, depressive symptoms, and cognition, with men showing greater dependence (p = 0.016). However, gender did not remain significant in Block 4, after including IADL experience (p = 0.334). In Block 4, IADL experience was the most important predictor of FAQ, as it uniquely explained 4.8% of the variation. The indirect effect of IADL experience on the relationship between gender and FAQ score was significant when tested using the Sobel test (ab = 0.114, p < 0.001, BCa CI [0.76, 0.17]). Above and beyond all of the variables included in the regression, FAQ was also significantly associated with AVLT delay recall (0.7%), AVLT delay recognition (0.4%), and LM-II delay recall (2%). Trails B/A was trending (0.3%, p = 0.072). APOE4 was a significant predictor of FAQ (1%) until Cognition was added to the model. GDS was significantly associated with FAQ in all Blocks (1.4% –1.6%). Together, all variables included in the regression model accounted for 22% of the variation in total FAQ.
The contribution of these predictors appeared to differ when stratified by gender. Cognition accounted for 18% of the variability in FAQ score in women (F(6,329) = 13.1, p < 0.001) compared to 10% in men (F(6,491) = 9.1, p < 0.001). On the other hand,Functional Reserve accounted for 6.6% of the variability in FAQ men (F(1,490) = 39.8, p < 0.001) relative to 2.4% in women (F(1,328) = 10.6, p = 0.001). Of the cognitive measures entered, AVLT delay recall (2%, t(490) = –3.0, p = 0.003) and LM-II delay recall (1%, t(490) = –2.8, p = 0.005) were significant in men, whereas AVLT delay recognition (1%, t(328) = –2.5, p = 0.012) and LM-II delay recall (4%, t(328) = –4.4, p < 0.001) were significant predictors in women. Lastly, in the final block, GDS was a significant predictor in women (3%, t(328) = 3.9, p < 0.001) and in men (1%, t(490) = 2.0, p = 0.048). To test whether these variables are differentially associated with FAQ scores across men and women, these variables were entered as interactions with gender. Overall, the variance explained by GDS, AVLT delay recall, AVLT delay recognition, LM-II delay recall, and IADLexperience did not differ significantly by gender.
DISCUSSION
We sought to examine how men and women differ in terms of functional impairment in MCI and to determine whether gender differences may be related to an underlying functional reserve. Our findings suggest that, although the effect is small, male gender is significantly associated with worse functional ability in a large sample of patients with MCI. Furthermore, this male disadvantage may be partially explained by lower IADL experience in men within this cohort. The block of cognitive variables as a whole accounted for the greatest amount of variance in functional dependence, although IADL experience was the most important single predictor. This may suggest that individuals with experience in a greater number of IADLs may develop a greater functional reserve, which might delay or slow functional decline in MCI.
Of the neuropsychological variables examined, delayed memory and recognition appear to be the only variables that are associated with functional dependence. Language ability did not significantly predict functional dependence. Additionally, individuals who were APOE4 carriers were more functionally dependent above and beyond age, gender, education, and depressive symptoms. This effect, however, was not significant after adjusting for cognition. This may indicate that possessing an APOE4 allele is associated with functional dependence in MCI as a result of its negative impact on cognition [17]. Finally, individuals with higher scores on the GDS showed greater functional impairment, although this relationship was not significantly different across genders. One study found that persistent apathy is a significant predictor for functional decline in women with AD [18]. Our study did not look specifically at apathy however, but rather, depressive symptoms overall.
Stratifying by gender demonstrated that overall cognition may better explain functional dependence in women, which was consistent with existing research [19]. However, when examining interactions with individual neuropsychological variables, no significant gender difference was found in terms of the variance explained. In terms of functional reserve, IADL experience appears to explain a greater amount of variance in men than women, which may be explained by the greater range of IADL experience in men (range = 4–10) compared to women (range = 6–10). However, this gender difference was also not statistically significant.
Overall, this study suggests that individuals with MCI who have experience on a greater number of IADLs tend to show superior functioning cross-sectionally. We propose that this experience may result in a resiliency to early functional decline through an increased functional reserve. Although the data provided through ADNI did not allow for the possible mechanisms of this resiliency to be explored, we would like to provide hypotheses for these mechanisms as avenues for future research on this topic. Given that the two main components of functional independence are cognitive ability and physical performance [20], it therefore follows that functional reserve may directly enable each of these components. Specifically, we hypothesize that increased IADL experience may result in developed resiliency in the form of neurological and physical changes.
Association with existing cognitive and brain reserve theories
To our knowledge, this is the first study to examine the influence of IADL experience on functional dependence. Our functional reserve hypothesis, borne out by the present study findings, is likely complementary with other existing reserve hypotheses (i.e., brain reserve [21] and cognitive reserve [22]), both of which have also been used to explain gender differences in neurodegenerative disorders. The concept of brain reserve suggests that certain factors, such as brain size, neuronal density, and number of synapses, may provide protection against the impact of neurodegeneration [21]. Cognitive reserve is thought to develop through lifestyle-related factors, such as higher educational attainment, increased occupational complexity, and frequency of mental stimulation throughout life. This may increase the brain’s ability to utilize deficient neural networks through greater neural efficiency and/or neural compensation through intact networks [22]. Generally, men are thought to possess greater brain reserve (i.e., greater brain size, and white matter volumes, although women tend to have a greater proportion of grey matter) and cognitive reserve (i.e., higher educational and occupational attainment), which may explain some of the differences found between men and women with MCI and AD [23].
Potential underlying mechanisms of functional reserve
Proposed cognitive mechanisms
The learning and mastering of daily activities inevitably results in changes at the neuronal and functional brain network level. Taking from the cognitive reserve literature, these neural changes may increase an individual’s ability to compensate for the effects of neurodegeneration, possibly through greater efficiency utilizing residual connectivity in damaged brain regions (i.e., neural efficiency) or better deployment of unaffected brain regions (i.e., neural compensation) [22]. As a result, it is possible that repetitive IADL experience may increase the cognitive capacity specific to related and unrelated tasks, thus prolonging functional independence (see Fig. 1). This may lead to a greater efficiency of expansive brain networks required for general IADL functioning [24] and within more specific regions involved in specific ADLs (e.g., angular gyrus for financial management) [25]. To explore these speculations, structural and functional brain imaging studies are needed to examine if the association between functional reserve and IADL decline is mediated by changes at the neurobiological level.
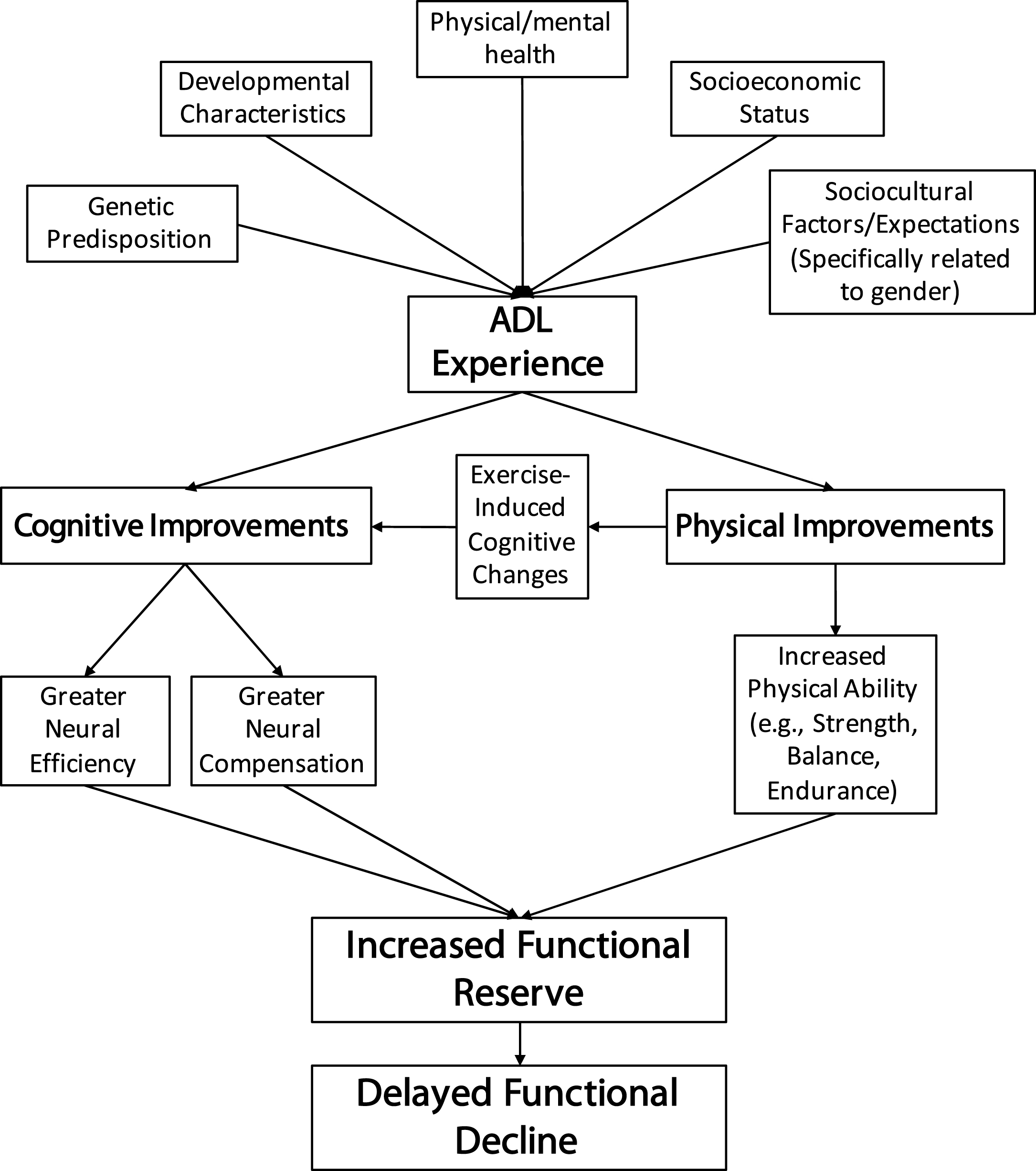
Diagram of the potential mechanisms that underlie the functional reserve hypothesis proposed in this study.
Proposed physical mechanisms
In addition to the cognitive skills necessary for functional independence, adequate motor ability is also required for many ADLs in terms of strength, coordination, and endurance, with several studies finding a direct link between physical activity and functional status [26] (see Fig. 1). Many IADLs in themselves may be considered a form of exercise, and as such, the physical demands of frequentlyperforming these tasks may contribute to a physical resiliency to functional decline. Furthermore, physical exercise may act upon functional ability through exercise-induced cognitive enhancements [27], with some studies showing significant cognitive improvements after a single aerobic session [28]. Resistance training is also thought to impact cognition through the effects of insulin-like growth factor on brain regions, such as in the hippocampus [29]. Interestingly, it appears that a combination of aerobic and resistance training programs may be the most beneficial in terms of cognitive outcome, relative to either form of exercise independently [27, 30]. Therefore, performing IADLs that involve aerobic and resistant activity may result in both physical and cognitive improvements, both of which may result in increased independence. Unfortunately, the data available did not allow for the physicality of IADL experience to be quantified; therefore, the validity of these proposed physical mechanisms could not be tested. However, future research examining the associations between IADL experience, physical decline, and functional impairment may allow for these hypotheses to be directly tested.
Limitations, future directions, and conclusion
Although this study has the strength of a large sample size, there are limitations. Firstly, the FAQ may not be sensitive to subtle IADL changes that occur early in the course of MCI between men and women. Additionally, the use of the FAQ in an MCI population resulted in a ceiling effect of scores, which we improved using log transformation. Recent ADL assessment tools have been developed to better quantify early functional impairment [31]; however, these were not collected as part of the ADNI protocol. Secondly, the FAQ is an informant-based measure, and as such, reporting bias may exist. However, one study found stronger associations between executive functioning and informant reports than with self-reports [32]. Furthermore, we contend that this bias would not differ across genders, mitigating its impact in the present analyses [33]. Additionally, a study by Farias and colleagues (2005) found that informant-reports of functional status were effective in differentiating normal elderly, MCI, and AD; however, self-reports could not differentiate these diagnostic groups [34]. A study by Tabert and colleagues (2002) suggests that this may be due to decreased awareness in MCI, with a greater discrepancy between informant- and self-reports predicting conversion to dementia [35]. Overall, these studies support the validity of informant-reports on the FAQ in this study.
A third limitation is that although we theorize that greater IADL experience results in independence in everyday functioning, the present analysis cannot infer causation. Additionally, although we propose potential cognitive and physical mechanisms that may underlie functional reserve, the available ADNI measures did not allow for the cognitive and physical contributors to IADL experience to be discerned. Similarly, it has been proposed that cognitive reserve may attenuate the association between cognition and functioning [36]. Although we did not find a significant association with years of education, other measures of cognitive reserve that are not collected in ADNI (e.g., type of education, bilingualism) may be of interest in future research.
Finally, our measure of functional reserve dichotomizes each IADL and therefore does not incorporate information regarding frequency and duration of experience. For this reason, further research is needed to validate and incorporate a more sophisticated measure of functional reserve, which should be used to replicate these findings. Future longitudinal analyses are required to examine the influence of functional reserve on the rate of functional decline, as well as the relationship with neuroimaging markers. Additionally, examining functional reserve within MCI subcategories (e.g., converters versus non-converters, amnestic MCI versus nonamnestic MCI) will be investigated in future studies. Finally, further analyses looking at the impact of specific IADLs on patient outcomes are of interest. For example, the Lawton ADL scale omits several ADLs when assessing men as these are deemed to be gender-biased (i.e., food preparation, housekeeping, and laundry) [37]. Therefore, future studies examining how experience on these activities may influence the trajectories of individuals at risk for dementia should be conducted.
In summary, this preliminary study suggests that women with MCI may be better protected against functional dependence as a result of greater IADL involvement (i.e., functional reserve). We hypothesize that performing IADLs throughout life may produce neural and physical alterations, resulting in a greater capacity to withstand neurodegeneration. However, future prospective studies are needed to test and validate these potential mechanisms. The findings from this study may have implications for delaying and treating functional disability associated with aging and dementia. Specifically, this study may provide an empirical basis for a shift toward implementing therapeutic interventions that focus on functional skills training.
Footnotes
ACKNOWLEDGMENTS
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of SouthernCalifornia.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of SouthernCalifornia.
CB gratefully acknowledges partial financial support through a Canadian Graduate Scholarship from the Natural Sciences and Engineering Research Council of Canada. JR acknowledges financial support from the Canadian Institutes of Health Research (MT#13129), the Linda C. Campbell Foundation, Heart & Stroke Foundation Canadian Partnership for Stroke Recovery, and the Canadian Vascular Network. ACR acknowledges support from the New Investigator Salary Award (MSH–130177), the Canadian Institutes of Health Research, and an Early Researcher Award (ER14-10-185) from the Ministry of Research and Innovation, Province of Ontario. JDE gratefully acknowledges support from the Heart and Stroke Foundation of Canada with a Focus on Stroke Post-Doctoral Fellowship award and from the Canadian Partnership for Stroke Recovery and Linda C. Campbell Foundation. BLC gratefully acknowledges financial support from the Alzheimer’s Association (#AACF-16-443540).
SEB receives financial support from the Department of Medicine, Sunnybrook HSC, the Sunnybrook Research Institute, the Brill Chair in Neurology from the University of Toronto and as Executive Director of the Toronto Dementia Research Alliance.
These findings have been presented as a platform presentation at the 2016 Alzheimer’s Association International Conference (AAIC) in Toronto, Canada.