
Abstract
Within neuropsychology, the term dispersion refers to the degree of variation in performance between different cognitive domains for an individual. Previous studies have demonstrated that cognitively normal individuals with higher dispersion are at an increased risk for progressing to mild cognitive impairment (MCI) and Alzheimer’s disease (AD). Therefore, we determined 1) whether increased dispersion in older adults was associated with amyloid plaques and neurofibrillary tangles (NFTs) and 2) whether increased cognitive dispersion accurately differentiated MCI and AD from non-cognitively impaired (NCI) individuals. The intra-subject standard deviation (ISD) was used to quantify cognitive dispersion, and receiver operator characteristic (ROC) analysis determined whether ISD differentiated MCI and AD from NCI. Neuropathological scores for diffuse plaques (DPs), neuritic plaques (NPs), and NFTs were used as outcome measures in a series of negative binomial regression models. Regression analyses found that increased ISD was associated with increased NFT pathology (β= 10.93, SE = 3.82, p = 0.004), but not with DPs (β= 1.33, SE = 8.85, p = 0.88) or NPs (β= 14.64, SE = 8.45, p = 0.08) after adjusting for age at death, gender, education, APOE ɛ4 status, and clinical diagnosis. An interaction term of ISD with age at death also showed a significant negative association (β= –0.13, SE = 0.04, p = 0.004), revealing an age-dependent association between ISD with NFTs. The ISD failed to show an acceptable level of diagnostic accuracy for MCI (AUC = 0.60). These findings suggest that increased cognitive dispersion is related to NFT pathology where age significantly affects this association.
INTRODUCTION
Since the underlying pathological processes of Alzheimer’s disease (AD) are thought to precede the manifestation of clinical symptoms by several years [1, 2], identifying and characterizing cognitive changes associated with the preclinical stage of AD have received significant attention in the field. This interest has resulted not only in revised diagnostic criteria aimed at providing more specificity in identifying individuals at risk for progressing to AD [3], but has also led to AD prevention trials that are enrolling asymptomatic individuals thought to be at-risk for AD by virtue of genetic and other biomarker characteristics [4, 5]. One of the primary challenges inherent in preclinical AD investigations is associating pathology with impairments in cognition. Previous cross-sectional studies have shown that cognitively normal individuals with high levels of AD pathology have significantly lower cognitive test scores relative to those with little or no AD pathology [6–12].
Recent longitudinal studies have suggested that intra-individual changes in cognition are associated with progression from normal cognition to mild cognitive impairment (MCI) [13–16]. Specifically, increased variability in an individual’s performance between different domains of cognition is associated with progression to MCI and AD. Within the neuropsychological literature, this variability is referred to as dispersion, which is defined in terms of the inconsistency in an individual’s performance between different domains of cognition (i.e., memory, executive function) [16].
Although reports have demonstrated that high levels of cognitive domain dispersion are associated with progression to MCI [13–16], a review of the literature failed to reveal any investigations showing an association between cognitive domain dispersion and AD pathology (i.e., plaques and tangles) or whether higher levels of dispersion accurately differentiate MCI and AD from non-cognitively impaired (NCI) individuals. Here we investigated whether higher levels of intra-individual cognitive domain dispersion were associated with greater neuritic plaque (NP), diffuse plaque (DP), and neurofibrillary tangle (NFT) pathology in a cohort of older adults who died with an antemortem clinical diagnosis of NCI, MCI, and AD and agreed to postmortem brain autopsy. In addition, we determined whether a measure of cognitive domain dispersion accurately differentiates MCI and AD from NCI cases.
METHODS
Data examined was derived from 249 older deceased and autopsied persons who died with a premortem clinical diagnosis of NCI (n = 123), MCI (n = 79), and AD (n = 47), had no coexisting clinical or neurological condition judged to contribute to cognitive impairment at their last clinical evaluation [17, 18], agreed to annual clinical evaluations, signed an informed consent and an Anatomic Gift Act, donating their brains at time of death, and who were participants in the Rush Religious Orders Study (RROS) [18, 19]. Data from these subjects have been used in numerous clinical pathological studies supported by our ongoing NIA program project grant entitled the “Neurobiology of Mild Cognitive Impairment in the Elderly” (PO1AG14449). At the time of these studies, individuals were chosen from all available RROS participants that came to autopsy during a rolling admission [17]. In addition, those taking anticholinesterases or medication for depression were also excluded. The Human Investigation Committee of Rush University Medical Center approved this study.
Clinical evaluation
Participants underwent a uniform, structured clinical evaluation performed by a neurologist and a trained neuropsychology test technician [17, 20]. Medications used by the subjects within the previous fourteen days of the examination were reviewed and classified. After review of all clinical data and examination of the participant, a clinical diagnosis was made by a board-certified neurologist or geriatrician with expertise in the evaluation of elderly persons with dementia. A neurologist reviewed the medical history, medication use, neurologic examination, results of cognitive performance testing, and the neuropsychologist’s opinion of cognitive impairment and dementia. Each participant was evaluated in their home, emphasizing findings deemed clinically relevant. Clinical diagnostic classification was performed as described previously [17, 20].
Tissue preparation and neuropathological diagnosis
Brain accruement and processing was described previously [20, 21]. Briefly, each brain was cut into 1 cm thick coronal slabs using a brain slice apparatus and hemisected. One hemisphere was immersion fixed in 4% paraformaldehyde (24–72 h) and cryoprotected (10% glycerol and 2% dimethyl sulfoxide in phosphate buffer solution) until processing for immunohistochemistry.
Diagnostic blocks (mid-frontal, superior temporal, entorhinal cortex, hippocampus, inferior parietal cortex, basal ganglia, thalamus, and substantia nigra) from the opposite hemisphere were paraffin embedded and cut at 6 μm. Examination for cerebral infarctions was conducted as described previously [22]. Bielschowsky silver stain was used to visualize NPs, DPs, and NFTs. Sections were also immunostained for Aβ using antibody 4G8 (1:9000; Covance, Princeton, NJ) raised against Aβ1 - 40 and Aβ1 - 42. Paired helical filament tau (AT8; 1:800, Covance, Princeton, NJ) immunohistochemistry was also used to label NFTs. Neuropathological diagnoses were determined according to CERAD [23] and Braak staging [24] as recommended by the NIA-Reagan criteria [25]. Exclusion criteria included mixed dementias, Parkinson’s disease, frontotemporal dementia, argyrophilic grain disease, vascular dementia, hippocampal sclerosis, stroke, and Lewy body disease. Lewy bodies (LB) were detected using α-synuclein (αSyn) immunohistochemistry as previously described [26] and scored semi-quantitatively according to the severity and anatomical distribution, separating brainstem predominant, limbic/transitional and diffuse neocortical types, depending on the anatomical distribution of αSyn [27, 28]. A board-certified neuropathologist or trained technician, blinded to clinical diagnosis, counted number of NPs, DPs and NFTs revealed by Bielschowsky silver stain in one square mm area (100× magnification) per cortical region as reported previously [19, 29].
Cognitive composite scores
Composite cognitive scores are based on the results of 17 individual cognitive tests divided into five domains of cognition (Episodic Memory, Semantic Memory, Working Memory, Perceptual Speed, Visuospatial) [20, 30]. For each test, raw scores were converted into z-scores based on the mean and standard deviation of the sample. The z-scores from the individual tests were averaged to create individual domain composite scores. Averaging z-scores from each cognitive domain examined produced a Global Cognitive Score (GCS). Test scores from the most recent clinical assessment prior to death were used in this study. Mini-Mental State Examination (MMSE) was used to describe the cohort overall cognition but was not used in the composite scores. For the AD group, only individuals with a MMSE score of 20 or greater were included in order to minimize floor effects on the cognitive tests and ceiling effects for the neuropathologicalvariables.
Within-subject dispersion measurement
The intra-subject standard deviation (ISD) was used to quantify cognitive domain dispersion for each individual. The ISD has been used in previous studies of cognitive domain dispersion [13–16] and consists of the standard deviation of the cognitive measures examined for an individual subject. For this study, the ISD is the standard deviation of the cognitive domain z-scores (Episodic Memory, Semantic Memory, Working Memory, Perceptual Speed, and Visuospatial) for a given subject.
Statistical analysis
For demographic and cognitive variables, the Kruskal-Wallis test was used to analyze group differences for continuous variables. The Conover-Inman test was used to discern statistically significant groupwise comparisons. Chi-square was used to analyze differences in categorical variables. Negative binomial regression models were used to assess the association between ISD and DPs, NPs, and NFTs, which displayed significantly skewed distributions with high standard deviations relative to the mean [31]. The ratio between the residual deviance value and the degrees of freedom for each model was used to assess model fit, as ratios that deviate substantially from the value of 1.00 indicate a lack of fit [32]. Clinical diagnosis, age at death, education, gender, APOE ɛ4 carrier status, and an interaction term of ISD and age at death were included in the models. Receiver operator characteristic (ROC) analyses were used to determine how well the ISD differentiated NCI from MCI and AD subjects. Diagnostic accuracy of the ISD was measured in terms of the area under the curve (AUC) value. Negative binomial regression models were carried out using the ‘glm.nb’ function in the ‘MASS’ package in R version 3.2.2 (The Comprehensive R Archive Network, http://www.cran.r-project.org/). ROC analyses were performed using MedCalc 16.2.1 (MedCalc Software). For all analyses, the significance level was set at α ≤ 0.05.
RESULTS
The cohort examined was comprised of 109 males and 140 females with an average age at death of 85.21±5.91 years and a mean of 18.26±3.39 years of education. The average duration between last clinical assessment and autopsy was 0.73±0.67 years and average post-mortem interval (PMI) was 7.63±7.01 hours. Descriptive statistics for the demographic and neuropathological variables by clinical group are shown in Table 1. No significant differences in gender frequency were noted between the samples, while the APOE ɛ4 allele was most prevalent in the AD group (p = 0.04). Education levels were similar between groups, while the AD group had a significantly higher age at death compared to the NCI cases (p = 0.01). PMI and brain weight at autopsy showed no significant differences between groups (p = 0.57, p = 0.08, respectively).
Demographic and neuropathologic characteristics by clinical groups
*APOE genotype not available for one individual in NCI and AD, two in MCI; mean±standard deviation; [range].
DPs and NPs showed significant group differences, with the MCI and AD subjects displaying significantly greater plaque pathology than the NCI group, while the AD cohort also had significantly greater NP scores compared to MCI. DPs were not significantly different between the MCI and AD groups. NFTs were significantly greater in the MCI and AD compared to the NCI subjects (Table 1, p < 0.001 for MCI and AD). A sub-analysis showed no significant differences in NP (p = 0.91) and NFT (p = 0.25) scores between the amnestic and non-amnestic MCI cases. By contrast, DPs were significantly greater in amnestic compared to non-amnestic MCI subjects (p = 0.01). The NCI group had a significantly greater percentage (37%) of lower Braak stages (0, I, II) compared to the MCI (22%) and AD (9%) groups. The prevalence of Braak stage III was relatively similar across groups (NCI –28%, MCI –24%, AD –23%) while more advanced Braak stages (IV and V) were most prevalent in the AD group (68%) followed by the MCI (54%) and NCI groups (35%). The NCI group also had a greater proportion of individuals with a CERAD classification of ‘No AD’ compared to the MCI and AD groups. For NIA Reagan diagnosis, the classifications of ‘Not AD’ and ‘Low Likelihood’ occurred more frequently in the NCI group compared to the MCI and AD groups (see Table 1).
Between-group analyses of the cognitive variables are shown in Table 2. MMSE scores showed significant differences between all three groups in the expected direction (NCI>MCI>AD, p < 0.001). Significant group differences were also noted for the GCS, Episodic Memory, Semantic Memory, Working Memory, Perceptual Speed, and Visuospatial domains (NCI>MCI>AD, p < 0.001; for all domains). ISD was significantly different between NCI and AD (NCI<AD, p < 0.001), MCI and AD (MCI<AD, p = 0.01), and NCI and MCI groups (p = 0.02) (Table 2, Fig. 1). ISD scores were not significantly different between amnestic and non-amnestic MCI cases (p = 0.25), and ISD scores were not significantly different between males and females (p = 0.44). ISD showed a weak, but significant, correlation with MMSE (r = –0.14, p = 0.03, Fig. 2).
MMSE, cognitive domain, and intra-subject standard deviation scores
mean±standard deviation; median [25th percentile, 75th percentile].
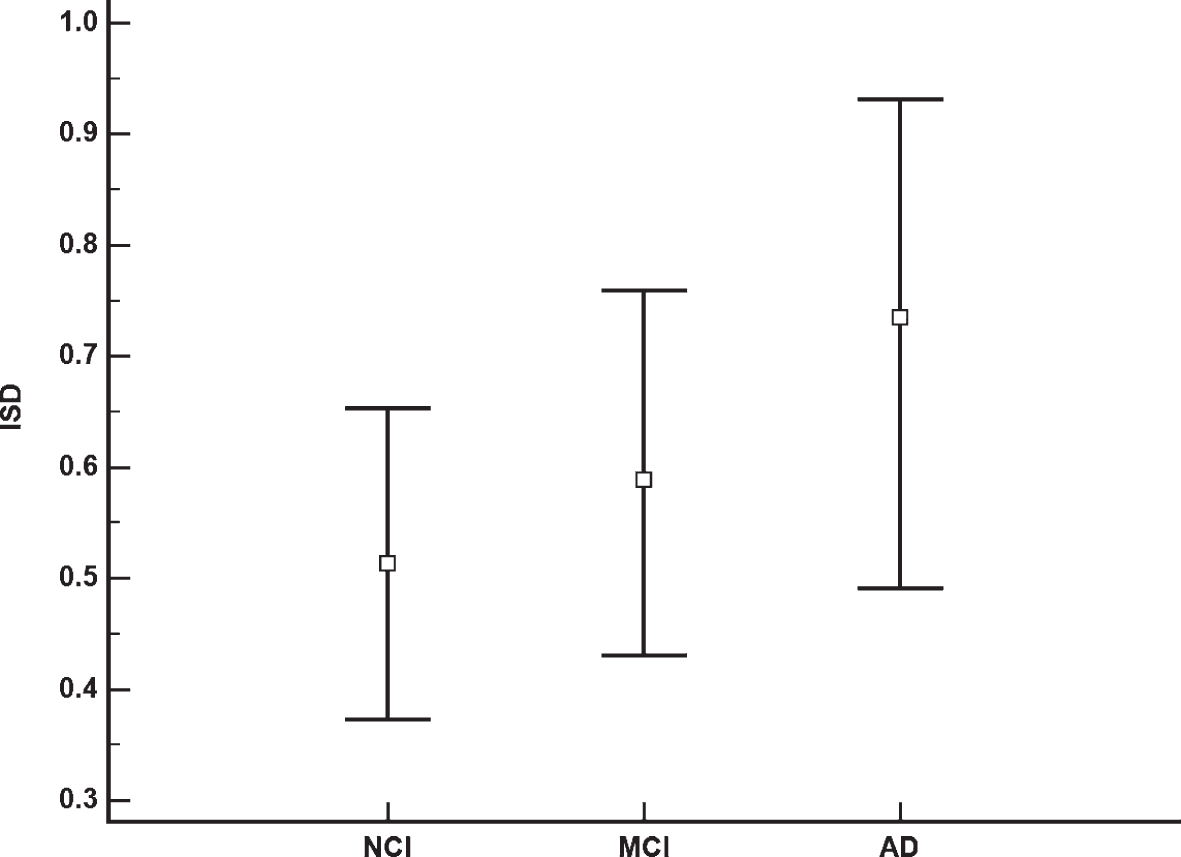
Boxplot showing statistically significant ISD differences between the NCI, MCI, and AD groups where boxes represent the median and error bars are the 25th and 75th percentiles. (NCI < MCI, p = 0.02; MCI < AD, p = 0.01; NCI < AD, p < 0.001).
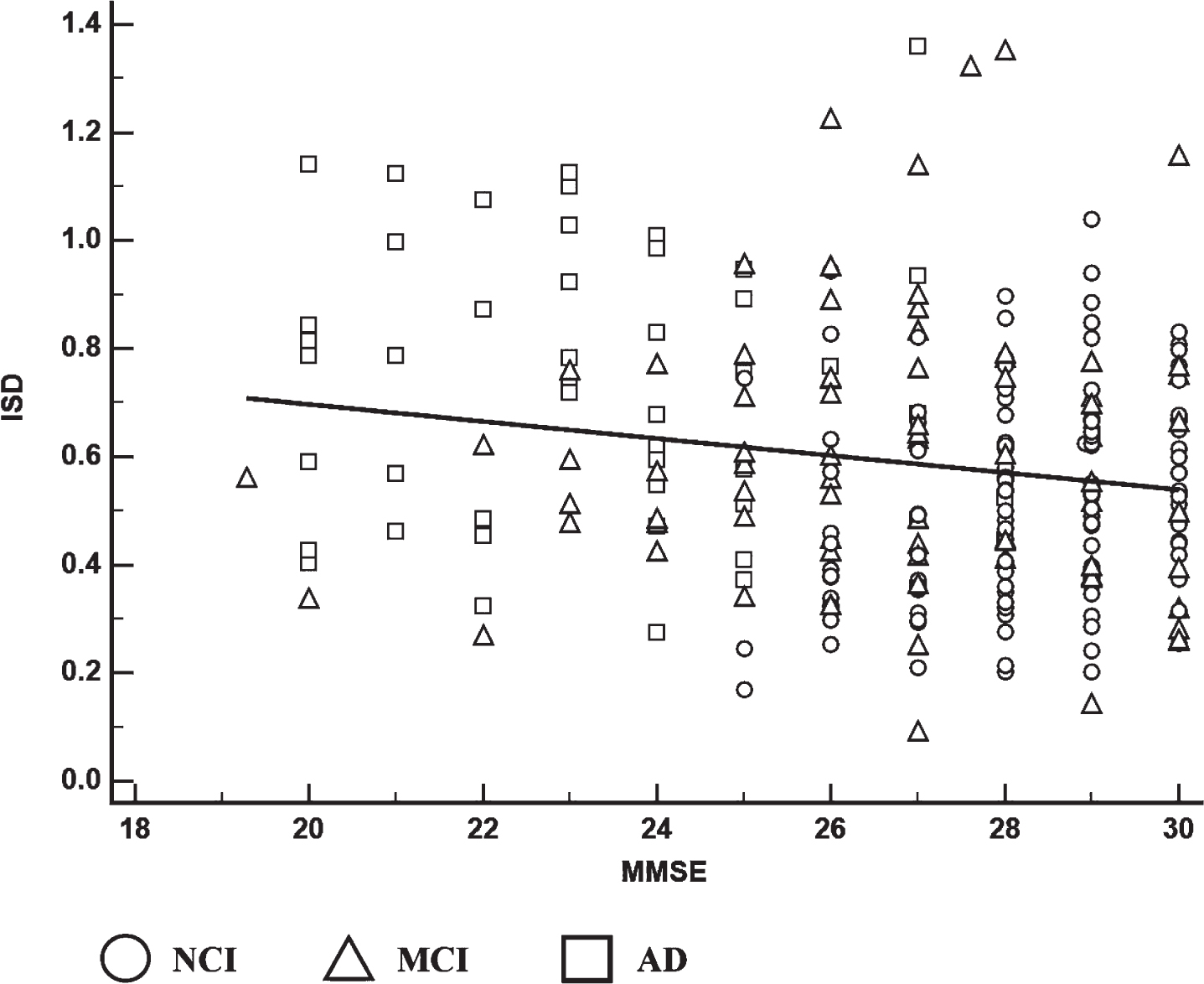
Linear association between ISD and MMSE where circles represent NCI, triangles represent MCI, and squares represent AD. Correlation is r = –0.14, p = 0.03.
Among the negative binomial regression models, ISD was significantly associated with NFTs (β= 10.93, SE = 3.82, p = 0.004), but not with NPs (β= 14.64, SE = 8.45, p = 0.08) or DPs (β= 1.33, SE = 8.85, p = 0.88) (Table 3). The interaction of ISD and age at death in the NFT model was also statistically significant (β= –0.13, SE = 0.04, p = 0.004), but not for the NP and DP models. The ratios of residual deviance to degrees of freedom for each model did not indicate a substantial lack of fit for any of the models examined, as the ratios were close to the value of 1.00 (Table 3). For the NP model, both age at death and APOE ɛ4 carrier status were associated with greater NP scores (age at death, p = 0.002; APOE ɛ4 carrier status, p = 0.003). Similar results were found in the NFT model (age at death, p < 0.001; APOE ɛ4 carrier status, p = 0.001). In the DP model, only APOE ɛ4 carrier status was associated with greater DP counts (p = 0.009). Results from the ROC analyses found that the ISD did not accurately differentiate MCI from NCI (AUC = 0.60, p < 0.001). When the MCI and AD groups were combined, diagnostic accuracy for the ISD remained poor (AUC = 0.65,p < 0.001).
Negative binomial regression results for ISD as a predictor of NFT, NP, and DP scores
All models adjusted for clinical diagnosis, age at death, gender, education, and APOE ɛ4 carrier status. *Values close to 1.00 indicate good model fit. DF, degrees of freedom.
DISCUSSION
In this study, we found that increased cognitive dispersion was associated with increased NFT pathology, after accounting for clinical diagnosis, APOE ɛ4 carrier status, gender, education, and age at death. However, the association between dispersion and NFTs was moderated by age at death. Contrary to previous studies [13–16], our findings did not show that cognitive dispersion using ISD was able to differentiate NCI from MCI, suggesting that intra-individual cognitive domain dispersion does not reflect early neuropathological changes, at least between the RROS clinical groups examined. On the other hand, Holtzer et al. [13] suggested that intra-individual cognitive domain dispersion serves as a marker for AD pathology and that increases in dispersion reflect the degradation of cortical interdomain networks involved in cognitive function. The present findings of an association between ISD and NFTs lends support to this observation since tangle pathology reflect neuronal degeneration, which would lead to a cortical network disconnection syndrome in AD. The lack of an association between ISD and plaque pathology indicates that significant cognitive domain dispersion may not be a factor during the early stages of AD pathogenesis, even though plaque pathology is thought to precede the development and accumulation of NFTs in the AD cortex [33].
In addition, older age at death and APOE ɛ4 carrier status were both associated with increased NPs and NFTs, suggesting that the relationship between AD pathology and cognitive function is indirect and multifactorial. Previously, we found a lack of association between cognition and AD pathology in elders without cognitive impairment [34], suggesting that cognitive impairment is mediated by additional processes and pathways that are not directly part of an amyloid and tau-based pathogenesis of AD [35]. Whether these subjects would fall into the category of “superagers” who withstand the behavioral consequences of AD pathology [36] is an intriguing question. Discerning the factors that offset dementia associated with AD pathogenesis may provide insight into the development of future therapies and treatment regimens. Additional work by our group found that longitudinal decreases in cognition among NCI cases were driven by the interaction of age at death, APOE ɛ4 carrier status, and Braak NFT stage [37]. The current data lend support to these longitudinal observations, given the significant association between ISD and NFT pathology. Perhaps other factors (e.g., vascular or inflammation) also mediate the neuropathology associated with age and APOE [38, 39], which affect an individual’s ISD score. In this regard, evidence derived from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) suggests that brain vascular dysregulation precedes the onset of amyloid deposition in the chain of events associated with AD pathogenesis [40]. Together, these findings suggest that amyloid plaque and NFT pathology alone may not be a necessary precondition for cognitive decline but is more likely due to a combination of factors coming together to form a perfect brainstorm. However, this study lacked the ability to explore these possibilities as data for vascular and inflammatory factors was not available.
In our findings, ISD values varied greatly across the range of MMSE scores, suggesting that measures of cognitive domain dispersion may have considerable overlap between clinical groups that would impede the ability of a dispersion measure to accurately differentiate MCI and AD from NCI individuals. Although the ISD values were statistically different between the clinical groups, each displayed a relatively wide range of ISD values between the 25th and 75th percentiles, which tended to overlap among the groups (Fig. 1). This, in part, may explain why clinically meaningful diagnostic differences were not detected via the ROC analyses. Although the ROC analyses yielded statistically significant p-values, the AUC values fall within a range that indicates poor diagnostic accuracy (0.60–0.69), which indicate a lack of clinical utility despite their statistical significance [41].
A limitation to this study was its cross-sectional design. Previous studies using the ISD as a predictor of progression from normal cognition to MCI/AD were longitudinal [13, 16] and thus the inclusion of a time component provides a substantially enhanced ability to assess associations of interest. In addition, subjects in this study were from a community-based group of highly educated retired clergy who had excellent health care and nutrition and were used in multiple clinical pathological [42] and epidemiological investigations [19]. Individuals who volunteer may introduce bias by decreasing pathology, but this is partially mitigated by high follow-up and autopsy rates of the RROS [21]. Another limitation is the relatively small number of APOE ɛ4 carriers, particularly homozygous individuals, may have effected the associations reported here. Future studies with a greater balance of APOE ɛ4 carriers and non-carriers will extend these results. Strengths include uniform premortem clinical and postmortem pathological evaluation, and that final pathologic classification was performed without knowledge of clinical evaluation.
Although intra-subject variability for cognitive tests was not able to accurately differentiate NCI individuals from MCI and AD subjects, increased cognitive dispersion demonstrated both an independent and age-dependent association with NFT pathology. A recent study found that increased cognitive dispersion is associated with decreased health status and increased frequency of self-reported cognitive complaints [43], suggesting that intra-subject measures of cognitive dispersion may provide some degree of clinical value. The extent to which these findings are associated with AD pathology is unclear, but raises the question of whether self-reported cognitive complaints and cognitive dispersion coincide with the presence of NFTs. The recent emergence of tau imaging [44] will allow for this question to be addressed in clinical samples. From a diagnostic standpoint, the results of this study contrast with the findings of longitudinal studies, using intra-subject cognitive dispersion as marker for clinical status. However, our finding of a positive association between cognitive dispersion and NFTs suggests that dispersion may be a useful cognitive marker for clinical trials utilizing therapies that targettau [45].
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants PO1AG014449, RO1AG043375, RO1AG010161, and RO1AG042146 from the National Institute on Aging, National Institutes of Health, and Barrow Neurological Institute Barrow and Beyond. We are indebted to the nuns, priests, and lay brothers who participated in the Rush Religious Orders Study and to the members of the Rush ADC.