
Abstract
This 6-month experimental case series study investigated the effects of a dual-task gait training and aerobic exercise intervention on cognition, mobility, and cardiovascular health in community-dwelling older adults without dementia. Participants exercised 40 min/day, 3 days/week for 26 weeks on a Biodex GaitTrainer2 treadmill. Participants were assessed at baseline (V0), interim (V1: 12-weeks), intervention endpoint (V2: 26-weeks), and study endpoint (V3: 52-weeks). The study outcomes included: cognition [executive function (EF), processing speed, verbal fluency, and memory]; mobility: usual & dual-task gait (speed, step length, and stride time variability); and vascular health: ambulatory blood pressure, carotid arterial compliance, and intima-media thickness (cIMT). Fifty-six participants [age: 70(6) years; 61% female] were included in this study. Significant improvements following the exercise program (V2) were observed in cognition: EF (p = 0.002), processing speed (p < 0.001), verbal fluency [digit symbol coding (p < 0.001), phonemic verbal fluency (p < 0.001)], and memory [immediate recall (p < 0.001) and delayed recall (p < 0.001)]; mobility: usual & dual-task gait speed (p = 0.002 and p < 0.001, respectively) and step length (p = 0.001 and p = 0.003, respectively); and vascular health: cIMT (p = 0.002). No changes were seen in the remaining outcomes. In conclusion, 26 weeks of dual-task gait training and aerobic exercise improved performance on a number of cognitive outcomes, while increasing usual & dual-task gait speed and step length in a sample of older adults without dementia.
INTRODUCTION
As the global population ages, the incidence of dementia is expected to continually rise [1]. An integral component to dementia prevention efforts will be the identification of modifiable risk factors associated with cognitive worsening [1–4] and the development of interventions that can improve brain health and functioning in older adults [5]. For instance, cardiovascular disease (CVD) risk factors have been recognized as some of the most readily modifiable risk factors for dementia [4, 6]. Indeed, the association between heart and brain health is evident, as greater vascular risk factor burden has been found to increase the risk of incident dementia over five years of follow-up among older adults with mild cognitive impairment [7]. Moreover, increased CVD risk factors have been associated with greater task-related activation and poorer task performance on executive function (EF) tasks in community-dwelling older adults [8].
Habitual participation in aerobic exercise (AE) consistently reduces CVD risk factor burden and may be an important strategy to reduce the risk of cognitive impairment and slow the progression of dementia [4, 9]. Previous meta-analyses suggest that AE can improve cognitive function within a number of cognitive domains, including processing speed, memory, and EF in healthy older adults [10–12] and can improve verbal fluency in those with indications of underlying cognitive impairment [13]. Of particular interest, EF appears to be exceptionally responsive to AE training [10] and can also improve following cognitive training [14]. Furthermore, cognitive training (CT) leads to improvements in EF and memory in healthy older adults [14, 15] and in those with cognitive impairment [16]. Although the evidence from these reviews is promising, recent meta-analyses have revealed inconsistencies regarding the impact of AE interventions and improvements in aerobic fitness on cognitive functioning in older adults, and the specific exercise training modality that is best suited to benefit the brain remains to be determined [17–19]. In addition to AE and CT, the effect of novel exercise modalities [i.e., dual-task (DT) training] on cognition and mobility in older adults has received increasing attention. DT training is a multi-dimensional intervention that combines physical and cognitive tasks in order to directly train the parieto-frontal networks of the brain [20] to divide attention and co-ordinate actions more efficiently [21, 22]. In this perspective, Erickson et al. [22] observed a DT training-related ‘shift’ in the location of DT-related brain activity (i.e., reduced activation within the right ventral inferior gyrus, right and left superior parietal lobules, and right dorsal inferior gyrus accompanied by increased activation within the dorsolateral prefrontal cortex from pre- to post-training), and suggested that this may represent a training-induced reorganization of the cortical areas involved in dual-tasking processing. DT exercise training improves memory [23, 24], EF [23–26], and global cognition [27], and can reduce the activation within regions of the brain associated with short-term memory dysfunctioning [24], and increase DT gait speed [28] in cognitively healthy older adults. DT exercise training has also been shown to benefit memory and EF, as well as usual and DT gait speed among elderly fallers [29] and improve DT performance among older adults with dementia [30]. Collectively, these observations suggest that DT exercise programs can benefit neural functioning, which may in turn mediate improvements in objective cognitive functioning, dynamic balance, and usual and DT gait performance among older adults. More specifically, early evidence indicates that DT training carried out using variable priority training strategy (i.e., allocating attentional resources intentionally to specific components of the DT at times), may lead to greater improvements in cognitive performance of older adults under DT conditions in comparison to others strategies, such as fixed-priority DT training (i.e., when attention is equally divided between both tasks at all times) [28].
Despite these initial observations, several limitations within the current literature must be addressed before the cognitive benefits of aerobically based exercise training can be fully understood. Furthermore, it is crucial to determine the efficacy of interventions aimed at simultaneously reducing the burden of modifiable dementia risk factors (i.e., CVD risk factors) and improving cognition and mobility in older adults at increased risk for future cognitive decline. The current body of literature suggests that aerobic-based exercise programs incorporating some form of cognitive training (e.g., DT) might impart a significantly larger global cognitive benefit then those focusing on single strategies [5]. Nonetheless, the specific type of exercise intervention, along with the frequency, duration, and intensity that would yield cognitive and mobility improvements, as well as reduce CVD risk factors, remains equivocal [19].
Therefore, the primary objective of this study was to test the hypothesis that 26 weeks of DT gait and AE intervention improves performance on an EF task. Secondary objectives determined whether the 26-week exercise intervention: i) improved performance on cognition tasks across multiple domains, including: information processing, verbal fluency, and memory; ii) enhanced usual and DT gait performance; iii) reduced 24-h ambulatory systolic and diastolic blood pressure (BP), and decreased vascular stiffness [i.e., carotid arterial compliance (CAC) and intima media thickness (cIMT)]; and iv) stimulated positive changes in cognition, mobility, and vascular outcomes that were maintained six months following the cessation of training.
MATERIALS AND METHODS
Study design
This study was a 6-month experimental case series coupled with a 6-month no-contact follow-up. Participants were assessed at four time points throughout the intervention and follow-up period: baseline (V0), interim (V1: 12-weeks), intervention endpoint (V2: 26-weeks), and study endpoint (V3: 52-weeks).
Participants
Participants were recruited from London, ON, using town hall announcements, calls to past research participants, and the distribution of advertisements to various locations throughout the community (i.e., Boys & Girls Clubs, Kiwanis Clubs, media outlets). Community-dwelling older adults (60–90 years) without dementia [i.e., no previous dementia diagnosis and a Mini-Mental State Examination (MMSE) score >24] [31], and preserved instrumental activities of daily living (Lawton-Brody Instrumental Activities of Daily Living scale) [32] were invited to participate. Older adults who demonstrated significant neurological (i.e., Parkinson’s) or orthopaedic (i.e., severe osteoarthritis) conditions, clinical depression (i.e., >16 on Center for Epidemiologic Studies-Depression Scale) [33] or at the discretion of the study physician), or BP unsafe for exercise (i.e., 180/100 mmHg or <100/60 mmHg) [34], and those who reported a recent severe cardiovascular complication (i.e., congestive heart failure, stroke), or could not comprehend the questionnaire material were excluded from participation.
Sample size
No study to date has observed the impact of laboratory-based DT gait and AE on EF in older adults; however, following reviews of studies using AE [10, 35] and other cycle-based exercise [36] aiming to improve cognition [i.e., EF measured via the Trail Making Test Part B (TMT-B)] in older adults allowed for the selection of an effect size of d = 0.66 for our calculations. The valid and reliable TMT-B [37] is specific to EF processes due to its requirements for switching sets and mental tracking throughout the task [37, 38] and was considered the primary outcome measure. Assuming an alpha of 0.05, 80% power, and a dropout rate of 10%, 84 participants were required for this study [39].
Baseline variables
Participant medical history and demographics were collected at baseline, and included: age, sex, ethnicity, years of formal education, body mass index, global cognitive functioning, the presence of subjective cognitive complaints, and estimated cardiorespiratory fitness [i.e., predicted maximal oxygen uptake (VO2max)]. Global cognitive functioning was assessed using the Montreal Cognitive Assessment (MoCA) [40]. Predicted VO2max was estimated using the Step Test and Exercise Prescription (STEP) tool [41].
Cognition
EF was assessed using TMT-A and B [37]. For the purposes of this study, TMT-B served as a surrogate of EF and the primary cognitive outcome, while TMT-A served as an index of information processing speed and a secondary cognitive outcome [37]. Similarly, the valid and reliable [42] Digit-Symbol Coding (DSC) from the Wechsler Adult Intelligence Scale [43] was also used as an index of information processing speed.
Semantic (animal naming) and phonetic (Controlled Oral Word Association Test) fluency tasks were used to evaluate lexical verbal fluency [44]. Memory was assessed using the Auditory Verbal Learning Test (AVLT) [45]. Responses from the immediate and delayed recall trials in the AVLT were tallied separately and served as the memory outcomes.
Mobility (gait)
Spatiotemporal gait characteristics were collected using a valid and reliable [46] portable electronic walkway system (GAITRite® System, Software version 4.7.1, CIR Systems, Peekskill, NY, USA). In order to avoid capturing acceleration and deceleration phases of the gait cycle, participant start and end points were placed 1.5 meters before and after the gait mat. Participants were required to complete two usual and DT walking trials at a comfortable pace. The serial sevens (serial 7 s) task was used as the DT condition in the current study (i.e., counting backwards by 7 s from 100) [29], and there was no instruction to prioritize either gait or responses to the cognitive tasks during the DT trials. Gait performance over two walks were averaged and used for analysis and gait speed (m/s), step length (cm), and stride time variability (CoV, %) were used as outcomes.
Vascular health
24-h ambulatory BP and carotid ultrasonography were used to evaluate vascular health. Following the gait assessment, participants were fitted with an appropriately sized, valid, and reliable [47] ambulatory BP cuff and monitor (SpacelabsTM 90207 Ambulatory Blood Pressure Monitor, SpaceLabs Inc.). Measurements were recorded two times an hour during the daytime (i.e., 06:00 to 22:00), and once an hour during the nighttime (i.e., 22:00 to 06:00) over the subsequent 24-h period, and mean 24-h systolic and diastolic BP were considered as outcomes.
Carotid arterial diameters were measured following previously published techniques [48]. Briefly, after 10 min of supine rest, a 10 MHz linear array B-mode ultrasonography transducer (Vingmed, GE Ultrasound A/S, Horton, Norway) was used to collect a longitudinal two-dimensional image of the cephalic portion of the right common carotid artery, 1-2 cm proximal to the carotid bifurcation. Arterial diameters were measured leading-edge-to-leading-edge at peak systole and end diastole and averaged across three cardiac cycles. Following the acquisition of the arterial diameters, carotid arterial pulse pressure was inferred through the collection of a single measure of resting supine brachial pulse pressure obtained using automated oscillometry (BPTru, Coquitlam, BC, Canada). Anatomical land marking ensured accurate comparisons over time. Carotid arterial compliance (CAC) was determined using the following equation: CAC = [π · (Dmax/2)2 –π · (Dmin/2)2]/ΔP, where Dmax was the systolic carotid arterial diameter, Dmin was the diastolic carotid arterial diameter, and ΔP was resting brachial pulse pressure [48]. cIMT was determined by subtracting the carotid arterial lumen diameter from the outer arterial diameter at end diastole.
In an attempt to control for external factors, vascular assessments were performed in a quiet, temperature controlled room (∼23°C), and participants were asked to refrain from the consumption of alcohol or participation in moderate-vigorous intensity exercise 24 h, and the consumption of caffeine 12 h, prior to the assessments [49].
Intervention: Laboratory-based DT gait and AE training program
Exercise training utilized a Biodex GaitTrainer2 treadmill (providing visual-spatial feedback related to the user’s step length on a screen fixed atop of the treadmill) under the supervision of research personnel. During each session, participants worked through a 5-min warm-up period, one 15-min stage of DT gait training, one 15-min stage of moderate intensity AE (i.e., 75–85% maximal heart rate determined using the STEP test protocol) [41], and a 5-min cool down stage. During the DT gait training stage, participants walked at a self-selected pace while receiving visuospatial step-length feedback and answering cognitively challenging questions (i.e., verbal fluency and arithmetic). The variable priority DT training was used during DT gait training portion of the exercise sessions [26]; for the first 7-min, participants prioritized providing correct responses to the verbal fluency and arithmetic tasks, and after a 1-min break (walk without answering questions), participants prioritized modifying their step length to achieve or surpass an individualized step length goal (for the remaining 7-min). Following the DT gait training component, the visuospatial step length feedback was removed and participants performed 15-min of moderate intensity AE. The incline and speed of the treadmill was increased until training heart rate was achieved, and the training intensity was monitored every 5-min throughout the 15-min of AE using a 10-point modified Borg Rating of Perceived Exertion (RPE) scale and the built-in handgrip heart rate monitor on the Biodex treadmill. The intervention was conducted 40 min per day, 3 days/week for 26 weeks.
Analysis
All analyses were performed using IBM® SPSS® Statistics for Windows, Version 20.0 (IBM Corp, Armonk, NY). Demographic variables at baseline were summarized as means and standard deviations or medians and interquartile ranges, where applicable. To determine the efficacy of the 26-week intervention on EF and whether changes in TMT-B scores were maintained after the no-contact follow-up, changes in TMT-B scores (time to complete test in seconds) were compared from baseline (V0) to 12-weeks (V1), 26-weeks (V2) and 52-weeks (V3) using a one-way repeated measure analysis of variance (ANOVA) using time as a main effect and post hoc tests that employed Bonferroni alpha adjustments. Using similar approaches, we further investigated changes in the secondary outcomes: information processing (DSC and TMT-A), verbal fluency [semantic (animal naming) & phonemic (COWA) fluency], memory (AVLT immediate and delayed recall), usual and DT gait (speed, step length and stride time variability), and 24-h systolic and diastolic BP, CAC and cIMT at V2 and V3. Outliers for each outcome were identified and removed prior to analyses, and Greenhouse-Geiser epsilon adjusted degrees of freedom were interpreted from the omnibus ANOVA tests. Friedman tests with alpha adjusted Wilcoxon sign ranked tests were used when violations of normality were encountered.
RESULTS
Participants
Figure 1 describes participant flow through the intervention. A total of 109 participants were assessed for eligibility, and 30 were excluded from participation (n = 17 did not meet the inclusion criteria; n = 13 declined to participate, primarily due to the time commitment required for the intervention). This left 79 participants who enrolled in the study, 56 of whom completed the entire 52-week study. There were no study-related adverse events experienced by any of the participants throughout the intervention and follow-up period. Participant characteristics are reported in Table 1. Participants [mean (SD) years: 70.4 (6.2)], were mostly women (61%), primarily Caucasian (95%), highly educated [mean (SD) years: 14.7 (3.2)], and just over half reported that their memory has deteriorated over the past five years. Furthermore, the participants had relatively preserved objective cognition [MoCA score, mean (SD): 25 (3.2)] and did not display any indications of the presence of unidentified dementia [MMSE score, mean (SD): 29 (1.3)].
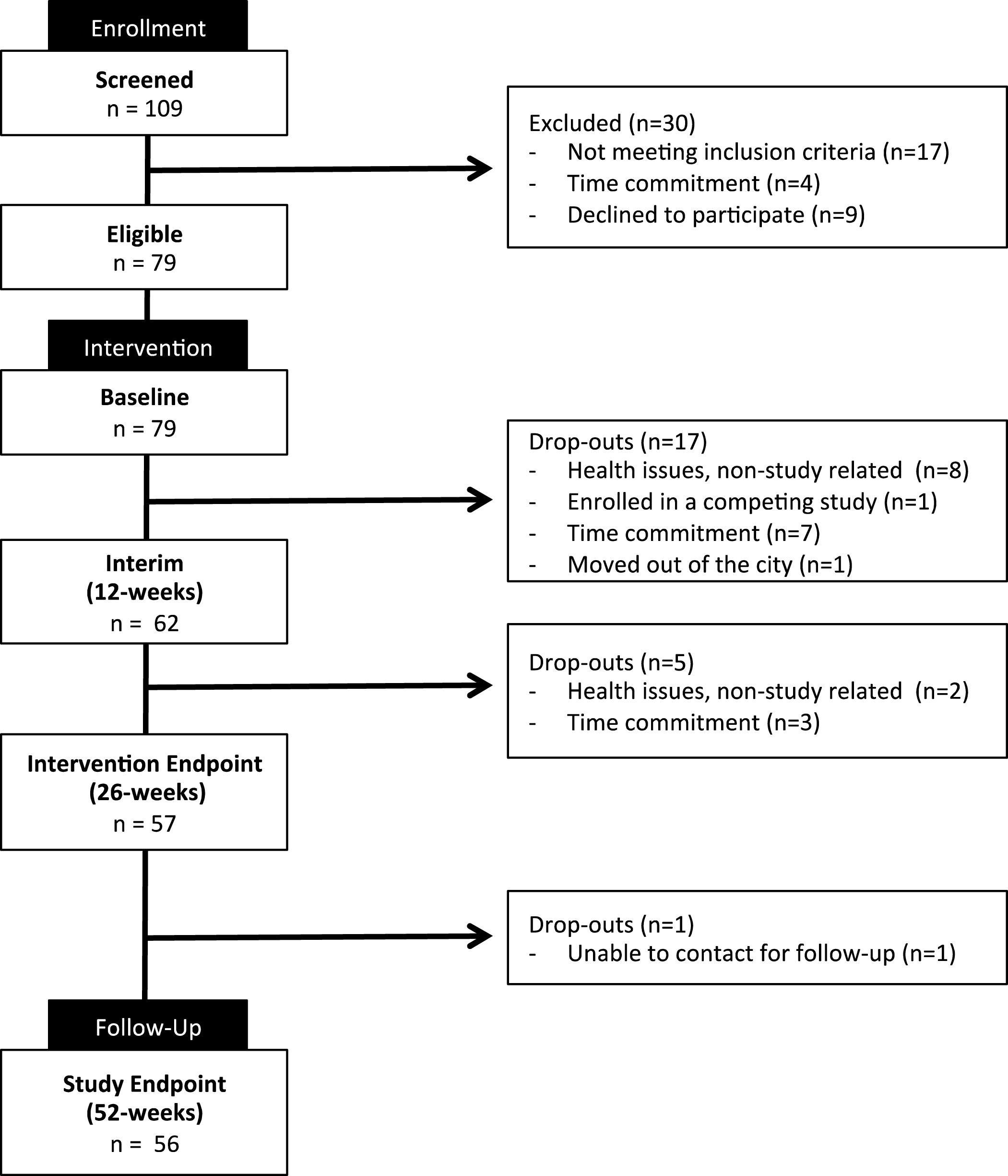
Participant flow through the dual-task and aerobic exercise intervention and follow-up period.
Baseline participant demographic and clinical characteristicsa
SD, standard deviation; BMI, body mass index; MMSE, Mini-Mental Status Examination; MoCA, Montreal Cognitive Assessment; CES-D, Centre for Epidemiological Studies Depression Scale. aData presented as either mean (standard deviation) or no. (%). bBody Mass Index measured in kg/m2. cVO2max was determined using the Step Test and Exercise Prescription tool. dParticipants rated their memory on a scale of 5 (1 = much better, 5 = much worse). eRange from 0 to 30; lower scores indicate greater cognitive impairment. fScores above 15 indicate clinical depression.
Cognition outcomes
Baseline cognitive scores are summarized in Table 2. The effects of the 26-week DT gait and AE training on the primary and secondary cognitive outcomes are reported in Table 2. The observed change in TMT-B performance from V0 to V1, V2, and V3 is shown in Fig. 2. A significant difference between TMT-B scores was observed (χ2 (3) = 19.49, p < 0.001). Post hoc tests with Bonferroni corrections (significance set at p < 0.008) revealed significant reductions in the time to complete TMT-B from baseline to intervention endpoint (p = 0.002), and a significant difference from baseline was maintained through the no-contact follow-up period [median (IQR): V3: 55.8 (41.6 to 74.5), p < 0.001]. There were no significant differences in TMT-B scores at any other time points.
Observed changes in study outcomes from baseline (V0) to intervention endpoint (V2)a
TMT, Trail Making Test; DSC, Digit Symbol Coding; VF, verbal fluency; COWA, Controlled Oral Word Association test; AVLT, auditory verbal learning test; BP, blood pressure; CAC, carotid arterial compliance; cIMT, carotid intima-media thickness. aData presented as either mean (standard deviation) or median (interquartile range). bThe removal of outliers results in differing sample sizes for the outcomes. cLower time to completion indicates greater performance. dScores range from 0 to 144; higher scores indicate greater performance. eScored as the correct number of unique responses provided in 60 seconds. fRange from 0 to 15; higher scores indicate greater performance.
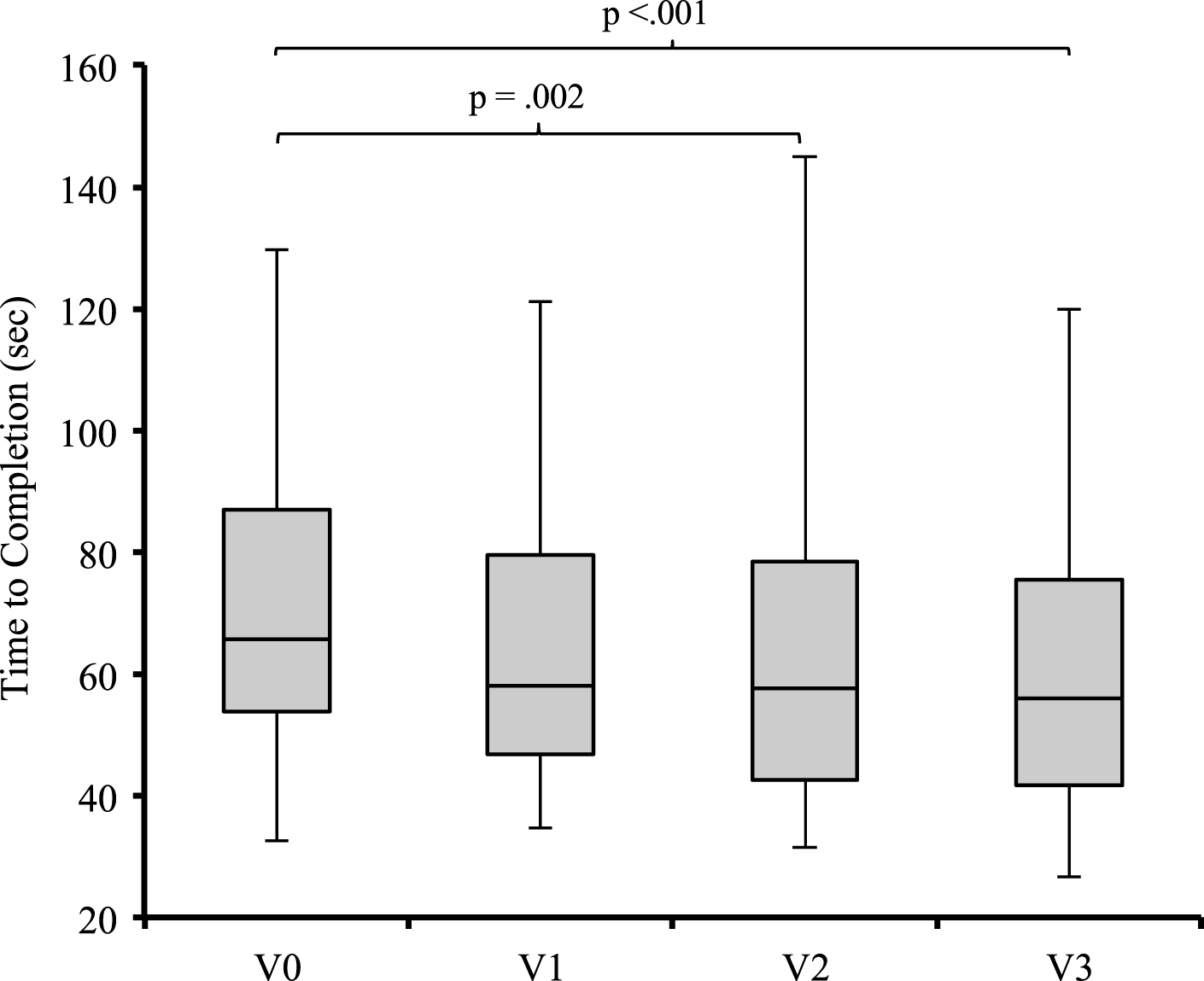
Trail Making Test (TMT) Part B performance at baseline, interim (12-weeks), intervention endpoint (26-weeks), and study endpoint (52-weeks).
The observed changes in the secondary cognitive outcomes from V0 to V2 are summarized in Table 2, and presented in Fig. 3. Significant reductions in TMT-A scores were observed following the 26-week exercise intervention (p < 0.001), and these changes were maintained over the 6-month follow-up [median (IQR): V3: 25.8 (22.3 to 29.8), p = 0.005]. At 26-weeks, the participants showed significant improvements DSC scores (p = 0.001), phonemic verbal fluency (p < 0.001), and immediate (p < 0.001) and delayed recall (p < 0.001), but not semantic verbal fluency. Compared to baselineperformance, the observed improvements DSC scores, phonemic verbal fluency, and immediate and delayed recall following the exercise intervention were maintained after 6-months of follow-up (all ≤0.001).
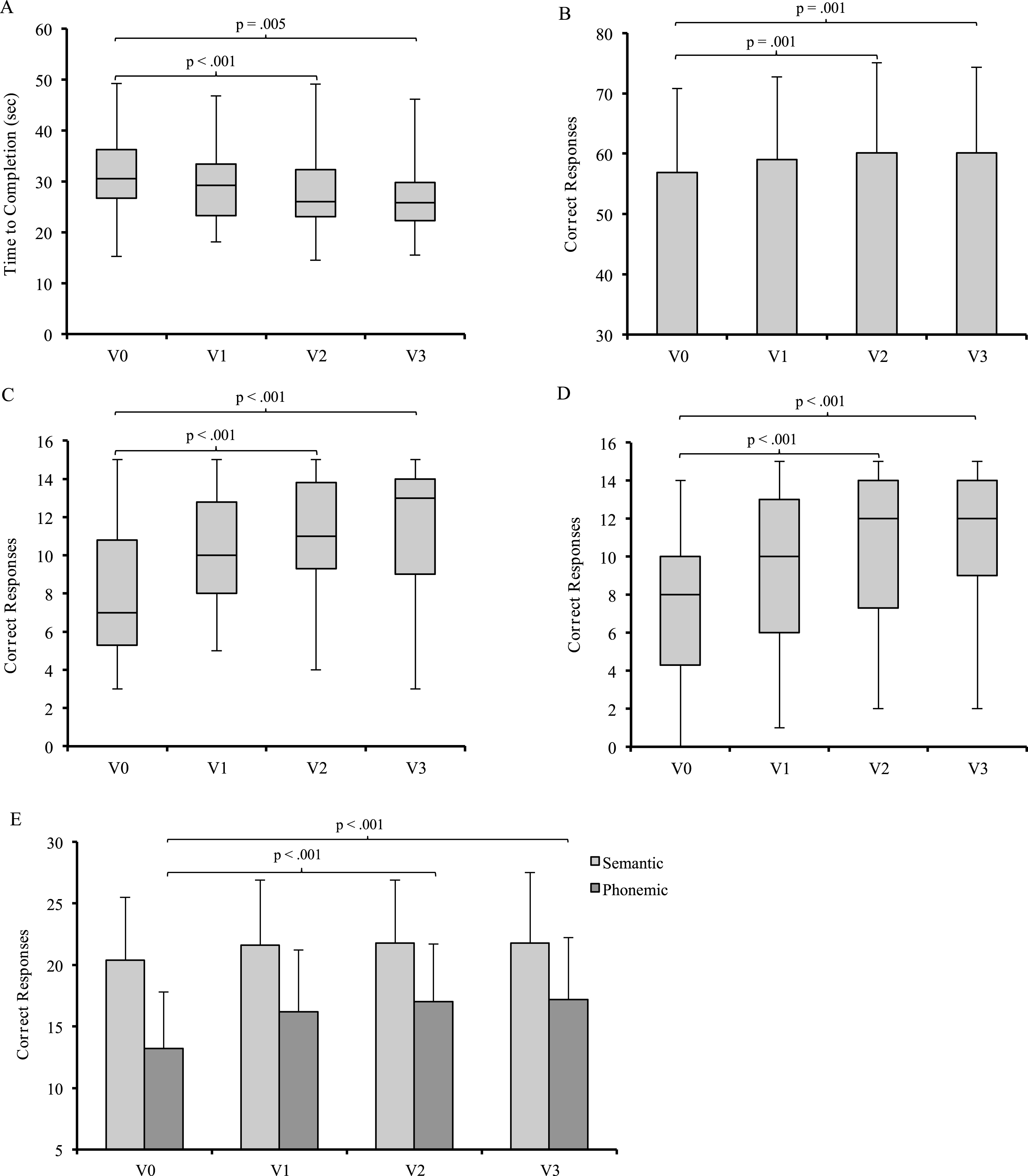
Performance on secondary cognitive outcomes at baseline (V0), interim (V1: 12-weeks), intervention endpoint (V2: 26-weeks), and study endpoint (V3: 52-weeks). A) Trail Making Test Part A; B) Digit Symbol Coding; C) Auditory Verbal Learning Test immediate recall; D) Auditory Verbal Learning Test delayed recall; E) Semantic and Phonemic verbal fluency.
Usual and dual-task gait outcomes
Changes in usual and DT gait speed, step length, and stride time variability from V0 to V2 are summarized in Table 2. Changes in usual and DT gait and stride-time variability from V0 to V1, V2, and V3 are presented in Fig. 4.
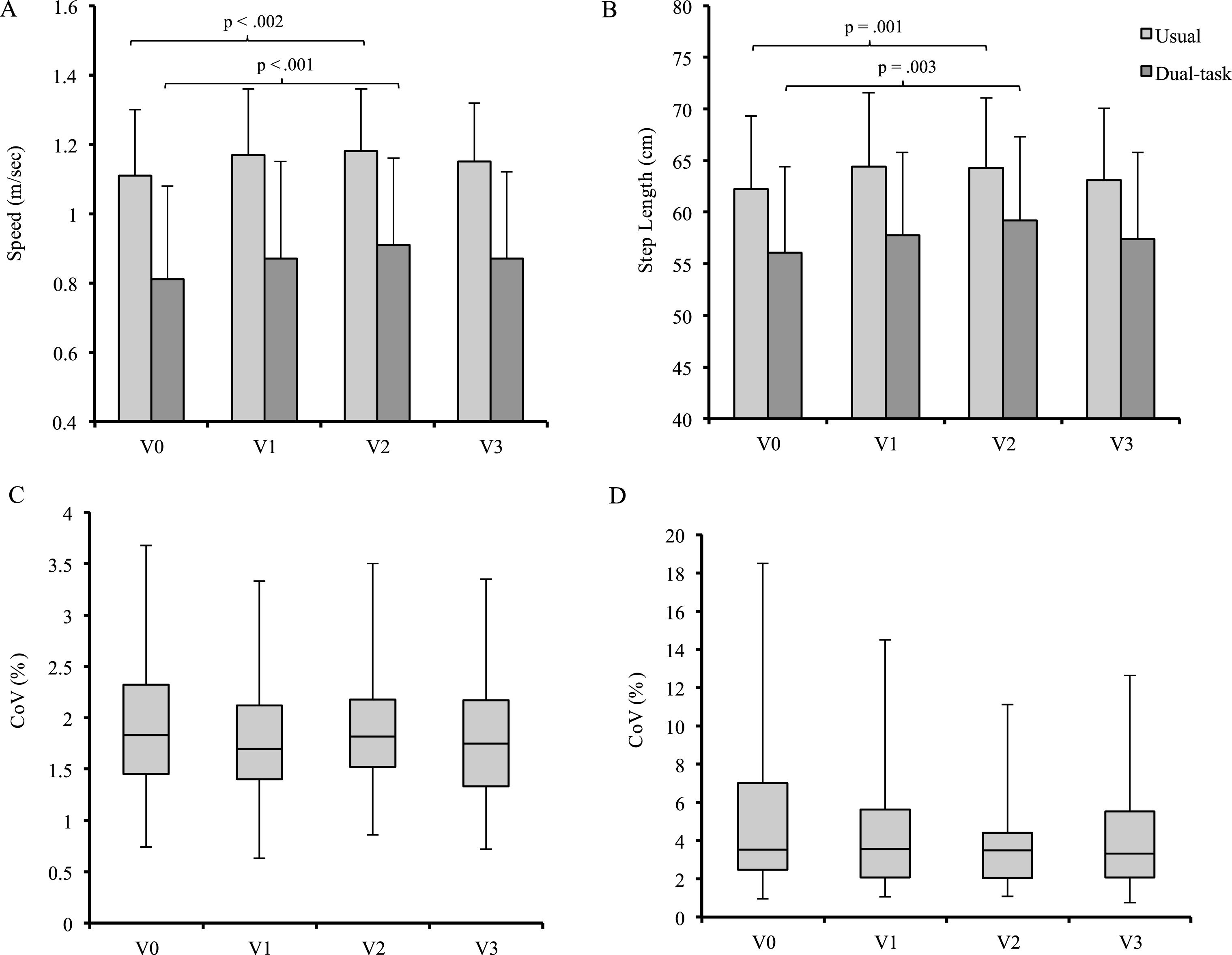
Changes in usual and dual-task (serial 7 subtraction) gait speed, step length, and stride time variability from baseline (V0), interim (V1; 12-weeks), intervention endpoint (V2; 26-weeks), and study endpoint (V3; 52-weeks). A) Usual and dual-task gait speed; B) Usual and dual-task step length; C) Usual gait stride time variability; D) Dual-task gait stride time variability. CoV, coefficient of variation.
Increased usual gait speed (p = 0.002) and step length (p = 0.001) were observed following the exercise intervention; however, after the 6-months of follow-up the improvements in usual gait speed and step length no longer remained [mean difference (95% CI) gait speed: 0.41 (0.90 to –0.078) m/s, p = 0.15; step length: 0.96 (2.5 to –0.54), p = 0.51]. Increased DT gait speed (p < 0.001) and step length (p = 0.003) were observed following the 26-week exercise intervention. After the 6-month follow-up, the improvements in DT gait speed and step length no longer remained [mean difference (95% CI) gait speed: 0.63 (0.13 to –0.08) m/s; step length: 1.3 (3.6 to –1.1) cm, all p > 0.05]. There were no observable reductions in usual and dual-task stride time variability following 26-week exercise intervention.
Vascular health outcomes
Differences in 24-h systolic BP, diastolic BP, CAC, and cIMT from V0 to V2 are summarized in Table 2. Changes in vascular health outcomes from V0 to V1, V2, and V3 are presented in Fig. 5. There were no significant changes in 24-h systolic BP, 24-h diastolic BP, or CAC following the 26-week exercise intervention (all p > 0.05). Compared to baseline, cIMT was higher after the 26-week exercise intervention (p = 0.002), but not after the 6-month follow-up.
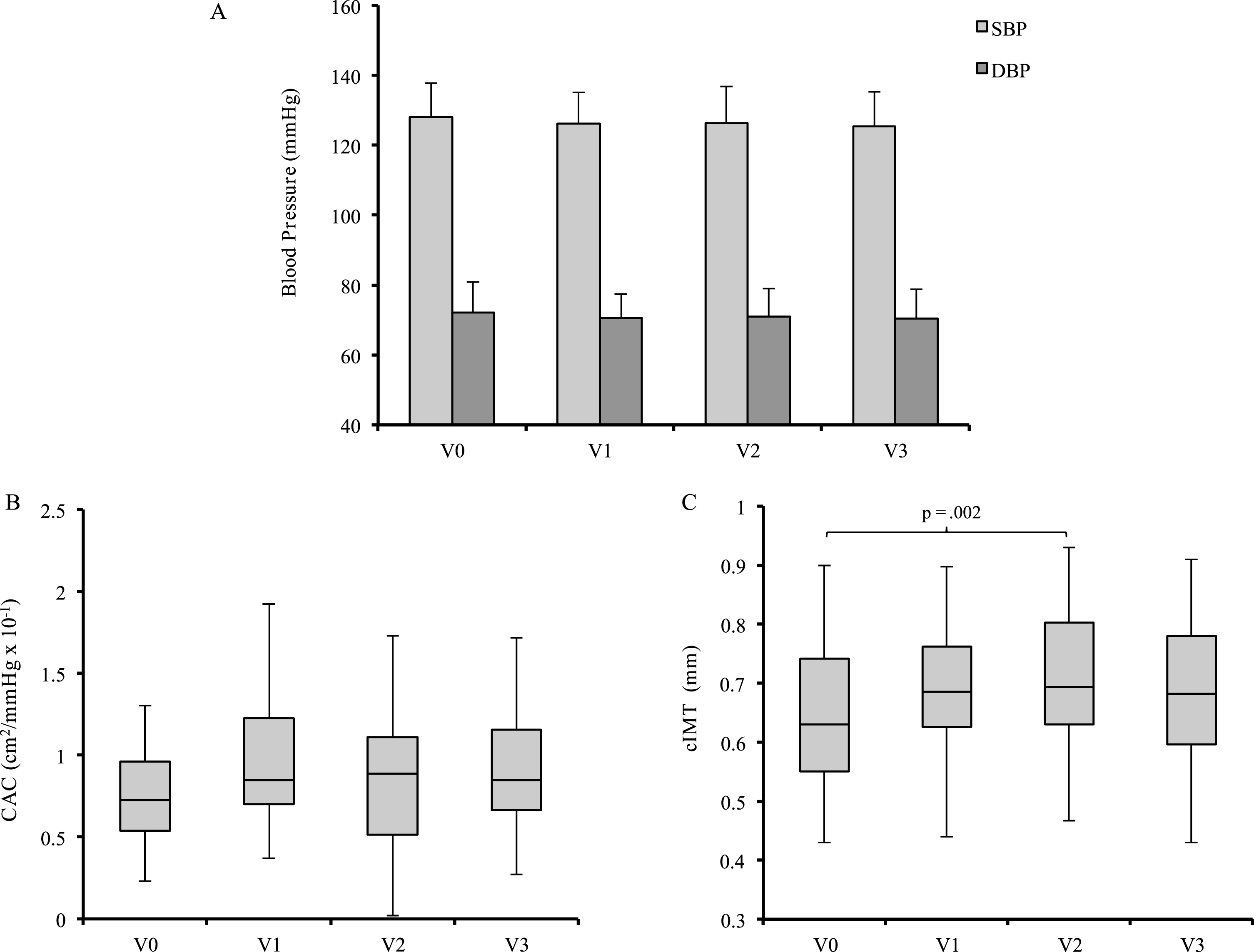
Changes in 24-h ambulatory systolic and diastolic blood pressure (A), carotid arterial compliance (B), and carotid intima-media thickness (C) from baseline (V0) to interim (V1; 12-weeks), intervention endpoint (V2; 26-weeks), and study endpoint (V3; 52-weeks). SBP, systolic blood pressure; DBP, diastolic blood pressure; CAC, carotid arterial compliance; cIMT, carotid intima-media thickness.
DISCUSSION
The effect of DT gait and AE training on cognition
Compared to age- and education-matched normative data, the study participants demonstrated on average better baseline performance on TMT-A and -B [50] and semantic verbal fluency task (letters starting with “C”) [51], comparable performance on the DSC [45] and the AVLT [45], and poorer performance on the phonemic verbal fluency task (naming animals) [51]. Following 26 weeks of treadmill-based DT gait and AE training for older adults without dementia, improvements in EF were observed and maintained over an additional 26 weeks of follow-up. Improvements in other cognitive processes, including information processing speed, verbal fluency, and memory were also observed following the 26-weeks exercise intervention, and these improvements were maintained for at least 26 weeks following the completion of the intervention. Performance on the semantic verbal fluency task was the only outcome that remained unchanged following the intervention, as well as the 26-week no contact follow-upperiod.
Evidence continues to suggest that AE training alone [54–56], or in combination with cognitive or DT training [27] can benefit brain health and improve cognition in cognitively healthy older adults, and even among those with objective cognitiveimpairment [35, 58]. Although recent meta-analyses have suggested that there is limited high-quality evidence to support the use of AE training alone as a method to improve cognition in older adults with [13] or without [17] cognitive impairment, recent observations suggest that combined cognitive and physical exercise training interventions may provide the greatest cognitive benefit [59].
The results from the current study expand our understanding of the influence of combined physical and cognitive exercise training on cognitive functioning in older adults. The 26-week exercise intervention combined moderate intensity AE with a DT gait training component that required participants to actively modify their step length using real-time biofeedback while simultaneously responding to a variety of verbal fluency and arithmetic tasks. Although this is the only study that the authors are aware of that has investigated the cognitive effects of such a unique DT stimulus in combination with an AE intervention, previous studies have investigated the cognitive benefits associated with other combined cognitive and physical exercise training interventions [60–64]. Although a number of exercise training modalities can benefit the brain, previous observations together with those from the current study collectively suggest that the cognitive response to these interventions appear to be unique and is likely dependent upon several key factors: i) the duration of the intervention, ii) the exercise intensity, and iii) the specific task requirements of the cognitive training components of each intervention. In contrast to several previous shorter duration studies [60–64], improvements in cognitive functioning following the exercise intervention were not apparent after 12 weeks of training, and did not emerge until the completion of the 26-week intervention. In lieu of these observations, several methodological differences may have contributed to the delayed cognitive response to the DT gait and AE training, specifically: i) the cognitive and functional status of the participants in the current study was relatively preserved and exercise-related improvements may have required more time to manifest; ii) the AE component was relatively short; iii) the use of a moderate intensity AE component, which was gradually progressed over the first two weeks of the intervention until the proper training intensity could be comfortably performed; and iv) the evaluation of cognition using different neuropsychological tests where performance may be more responsive to exercise training. For instance, Dorfman et al. [29] observed significant reductions in TMT-B scores following 12 weeks of treadmill-based DT exercise training for older idiopathic fallers. Although the participants in both studies were of similar age, education, and cognitive status (i.e., MoCA scores), the participants did differ on their previous falls history. Cognition, especially EF, is highly associated with the control of gait, balance, and falls prevention [65, 66]; thus, when compared to those without a history of falls, older adults with a history of falls may have a greater degree of underlying executive dysfunction, which would be more sensitive and responsive to interventions directed toward mitigating falls risk. Differences in baseline TMT-B scores between the participants in the Dorfman study [29] and the present study [mean (SD): 148.8 (65.3) versus 69.9 (24.7) s] suggests greater executive deficit among the idiopathic fallers of the former study, which may have allowed for a more immediate EF response to training.
The observations presented herein are also aligned with previous work that investigated the additional cognitive benefit that is provided by including a DT training component to a standardized senior’s fitness program [27]. In example, a previous study reported by our group [27] employed a 26-week randomized controlled trial whereby participants performed a standardized senior’s fitness program and mind-motor exercise (i.e., square stepping exercise) in isolation, or with the addition of a cognitive task (i.e., verbal fluency or arithmetic). Following the intervention, improved global cognitive functioning was observed among those who performed the standardized fitness program followed by square-stepping exercise with simultaneous cognitive tasks, compared to those who exercised without additional cognitive tasks. In contrast to the results of the present study, Gill et al. [27] observed that improvements in global cognition were driven by increased performance on verbal fluency and memory tasks, but not EF. The differences in the executive cognitive response between these studies may be in part due to discrepancies in the DT requirements and differences in design of the interventions. For instance, participants in the previous study [27] were subject to an a group-based intermittent DT training (i.e., square stepping exercise plus cognitive tasks) stimulus during 15 min, whereas in the present study, participants exercised individually and continuously as part of a 15-min DT gait training component. Although DT training can benefit cognition, and specifically EF [27, 29], questions regarding which type of DT stimulus and the intensity of that stimulus are best suited to improve cognition, still remain. The relationship between EF and the control of gait may have allowed for the current intervention to more directly influence EF than those that employ an unrelated DT condition during training.
The longitudinal observation of the decay of the cognitive benefits that are obtained through exercise training has received little attention [5]. Recently, Rahe et al. [62] observed the maintenance of improved attention up to 1 year of follow-up, while the LIFE trial [67] did not detect any maintenance and suggest that the cognitive benefits of exercise training dissipate after 2 years of follow-up. Findings from the present study suggest that the cognitive benefits garnered through the participation in the exercise intervention persist for up to 26-weeks following the cessation of the intervention. Taken together, it appears that mid- to long-duration (i.e., 12- to 26-weeks) exercise training interventions can provide cognitive benefits that persist for 26- to 52-weeks post-training; however, sustained participation in exercise training programs may be required to prevent the decay of any cognitive benefits that are achieved. In the current study, we did not track participants’ levels of physical activity following the study endpoint, which limits our understanding with regards to the longevity of exercise-driven cognitive improvements. Therefore, further work is required to determine the trajectory of the decay in the cognitive benefits garnered through exercise training.
The effect of DT gait and AE training on usual and dual-task gait
Compared to age-matched data, the study participants demonstrated on average comparable usual gait speed, step length and stride time variability [52], and dual task gait speed, step length, and stride time variability [48].
Improvements in usual and DT gait speed and step length were observed following 26 weeks of DT gait and AE training, yet stride time variability remained unchanged. Despite the beneficial effect of training, the improvements in usual and DT gait speed and step length were not maintained after 26 weeks of no contact follow-up. Recent meta-analyses have identified increased gait speed as the primary mechanism by which exercise benefits gait performance [68, 69]. Indeed, these suggestions are aligned with the results of the current study and those from previous works, which observed increased usual and DT gait speed following 12 weeks of treadmill-based DT training [29] and DT gait speed following 26 weeks of standard senior’s fitness training combined with single or DT mind-motor exercise training [48]. The influence of exercise training on usual and DT step length is less definitive, as improvements in step length have not been consistently found [29, 48]. In contrast to results reported from Gregory and colleagues [48], observations from treadmill-based training interventions suggest that these programs can increase usual and DT step length [48]. Compared to other novel cognitive-motor interventions, treadmill-based interventions involve a repetitive stepping requirement that is readily comparable to the demands of usual gait, and thus provide benefits that are more readily translatable to daily locomotion. Differences in the motor requirements of the DT between these studies (i.e., treadmill-based versus square-stepping exercise) likely contributed to the discrepancies in the effect of the interventions on usual gait performance.
Stride time variability under usual and DT conditions was not influenced by the DT gait and AE intervention. Increased gait variability has been identified as a falls risk factor [70, 71] and is a common characteristic of mild cognitive impairment [72, 73]. Participants in the present study were, on average, cognitively healthy and functionally independent community-dwelling older adults. Furthermore, these individuals demonstrated relatively preserved stride time variability at baseline [CoV (%), median (IQR): 1.8 (1.5 to 2.3) % ]. Beauchet et al. [74] determined that only those with the greatest variability at baseline (i.e., >4.4%) experience reductions in stride time variability following exercise training. The relatively preserved cognitive and functional status of the participants in the current study likely contributed to the lack of observed change in the gait variability outcomes following the exercise intervention.
The effect of DT gait and AE training on vascular health
Compared to age-matched data, the study participants demonstrated on average lower cIMT [53], and similar 24-h systolic BP, 24-h diastolic BP, and CAC [48].
Following 26 weeks of DT gait and AE training, 24-h ambulatory systolic and diastolic BP, and CAC remained unchanged, while cIMT increased. After 26 weeks of no-contact follow-up, 24-h systolic and diastolic BP, CAC, and cIMT were not significantly different from baseline. CVD risk factors, specifically hypertension [75] and the associated exacerbations in age-related arterial stiffening [76], have been implicated as mechanisms that drive neuropathological changes (i.e., reduced brain volume, white matter hyperintensities, and silent cerebral infarct) in the aging brain and the establishment of dementia [77]. However, recent reductions in the incidence of cognitive impairment have been attributed in part to increased efforts to prevent and manage CVD risk factors [78]. Exercise training is a cornerstone lifestyle modification used for CVD risk factor management, and increasing evidence suggests that exercise can benefit cognition [5]. Although exercise-induced adaptations to vascular structure and function and improved neurovascular coupling have been suggested as primary mechanisms that drive improved cognition post-training [79], the cognitive benefits that were observed within the current study emerged without concurrent changes in vascular health.
The lack of an observed change in ambulatory BP and CAC within the current study may be attributed to the level of baseline fitness of the study participants and the lack of change in predicted VO2max following the intervention. There was no requirement for a history of recent sedentary living within the inclusion criteria, nor was habitual exercise participation quantified upon entry to the study; the blunted vascular response to training could have occurred as a result of participants substituting previously performed exercise training with the DT gait and AE intervention. In addition, although aerobically based exercise training imparts both cardiovascular and cognitive benefits, very little is known about whether these benefits occur alongside one another. Other mechanisms, such as elevations in circulating growth factors, cortical volume, neurogenesis, neural efficiency, or cerebral glucose metabolism, and reductions in oxidative stress, and beta amyloid burden, that are able to act in a manner independent to changes in vascular physiology, remain under investigated and may be equally as important to consider [80–84].
Observational studies have identified cIMT as an index of vascular stiffness, and elevations in cIMT over time have been associated with adverse cardiovascular events (i.e., myocardial infarction) [85], the development of white matter hyperintensities [86] and stroke [87]. Although exercise training has consistently been shown to benefit traditional indices of vascular health (i.e., BP and arterial compliance), its influence on cIMT remains equivocal. Reductions in cIMT have been observed, but this response has only been found following high-intensity and long duration exercise training [88]. In the current study, due to baseline fairly high fitness levels and lack of change in predicted VO2max post-training, we did not expect to see significant changes in cIMT. The observed elevations in cIMT post-training are likely the result of normal age-related changes to vascular wall structure that occur in order to maintain intra-arterial pressure and flow homeostasis [89]. Furthermore, these observed elevations in cIMT are well within what is considered the “normal” range for older adults without established CVD [89]. Taken together, these observations suggest that the intensity of the DT gait and AE intervention was insufficient to prevent the natural progression of age-related elevations in cIMT.
Limitations
The majority of the participants in the current study were Caucasian (95%) and highly educated, and nearly two-thirds were women, all of which should be considered when interpreting and generalizing these findings. The current investigation followed a case study design, and there were no controls or comparison groups included. The omission of a comparison group does not allow for the determination of whether or not the changes in cognition that were observed during the study occurred as a result of other extraneous factors (i.e., increased socialization). There were also limitations associated with the specific outcomes used in this study. Cognition was assessed using traditional pen and paper-based neuropsychological outcomes, which may have contributed to the occurrence of practice effects. However, as previous observations suggest, the likelihood of encountering practice effects on cognitive testing is significantly diminished if assessment sessions are spaced at least 12 weeks apart [90]. Also, we acknowledge that since a similar pattern was observed for TMT-A and DSC (i.e., measures information processing speed), improvement in TMT-B performance may not necessarily reflect changes in EF, but rather be driven by ameliorated performance in information processing speed. Furthermore, environmental and contextual cues can also serve as a primer for cognitive performance. For instance, Hupbach et al. [91] found that memories could be automatically reactivated when an individual returns to an original learning context. The participants in the current study performed the cognitive assessments in a small clinical room that was not used for any other study-related purposes, and this unique assessment environment may have served to subconsciously prime cognitive performance. The possibility for contextually cued cognitive performance during follow-up assessments and the absence of an inactive control group for appropriate comparisons of cognitive performance over time must be considered when interpreting these results. Several limitations related to the DT gait assessments must also be identified, including i) the task delivery was not randomized (i.e., usual gait followed DT condition), ii) the starting point for the serial subtraction DT was not modified between visits, and iii) performance on the secondary tasks within the DT gait assessment was not methodologically controlled (i.e., performance on serial 7 s subtraction in isolation, without the walking task). Finally, although ideal vascular testing conditions and the associated participant responsibilities were outlined and verbally communicated 24 h prior to the vascular assessments [49], adherence to these requirements was not evaluated or enforced.
Conclusions
Numerous studies continue to support the use of cognitive and physical exercise training as an effective non-pharmacological intervention to mitigate CVD risk factor burden, improve physical function, and benefit cognition [92]. During pathological cognitive aging, EF and memory are often the first cognitive domains affected [93]; therefore, identifying interventions that aim to prevent incipient cognitive decline through the simultaneous targeting and training of these cognitive domains is of considerable importance. Treadmill-based DT gait and AE training may be an attractive choice, as the cognitive requirements of this exercise program (i.e., DT control of gait while providing responses to the verbal fluency task) targets and trains both EF and memory processes. Results from this study indicate that 26 weeks of DT gait and AE training can improve functioning within a number of diverse cognitive domains and benefit usual and DT gait performance, but not influence vascular health, in community-dwelling older adults without dementia. These observations support the notion that combined exercise training interventions impart diverse cognitive and motor benefits, and that DT gait training may be an effective method to directly target and train EF and memory. Future work is required to determine whether the cognitive benefits that are associated with DT gait and AE training are greater than what can be achieved following other exercise training modalities, and whether these observations can be replicated in a community-based setting.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the study participants and the staff at the Parkwood Research Institute, in affiliation with Lawson Health Research Institute in London, Ontario. In addition, we would like to thank the following research staff: Noah Koblinski, Ashleigh De Cruz, Lee Gonzalez, Heather Morton, Stephanie Muise, and Tina Felfeli.
This study was supported by a Team Grant from the Canadian Institutes of Health research (Grant number: 201713), and by the Fellowships in Care of the Elderly Research and Rehabilitation, a training award offered through the Parkwood Research Institute in partnership with St. Joseph’s Health Care Foundation. The funding sources had no involvement in this study, including data collection, analysis, or interpretation of data.