
Abstract
Among primary progressive aphasias (PPAs), logopenic variant PPA (lv-PPA) is usually related to Alzheimer’s disease. Although it has been widely clinically and pathologically evaluated, the topography in LPA is still controversial. We report a patient presenting with a logopenic syndrome due to a strategic lesion located in the superior and middle temporal gyrus and compare our findings with those of a PiB-PET positive lv-PPA patient matched by age, gender, and education. We consider that our study provides new anatomical clues to better understand the cognitive mechanisms underlying the logopenic syndrome.
INTRODUCTION
Primary progressive aphasia (PPA) refers to a clinically and pathologically heterogeneous group of neurodegenerative disorders characterized by progressive language difficulty with relative sparing of memory and other cognitive functions, at least early in the disease course [1]. Based on the clinical profile, PPAs are divided into three different variants: i) semantic variant PPA (sv-PPA), ii) non fluent variant PPA (nfv-PPA), and iii) logopenic variant PPA (lv-PPA). sv-PPA and nfv-PPA are usually related to frontotemporal lobar degeneration, while lv-PPA is commonly associated with Alzheimer’s disease (AD) [2].
Clinically, lv-PPA is characterized by slow rate speech, phonemic paraphasias, naming impairment, and marked difficulties in single word retrieval and repetition. Characteristically, comprehension, grammatism, and language articulation are usually less affected [1]. Although it has been widely pathologically evaluated, the topography in lv-PPA is still controversial. On this basis, atrophy at the temporo-parietal gyrus has been documented in some patients [3]. However, what regions are critical to the emergence of the clinical manifestations, or whether these deficits appear as a result of abnormalities of single or multiple segregated regions, has not been fully and precisely elucidated [4, 5]. Many authors have described infarcts causing amnestic-multidomain cognitive deficits, as well as other aphasic syndromes [6, 7]; however, the association of a strategic stroke mimicking a lv-PPA syndrome has not been reported to our knowledge.
We report a patient presenting with a logopenic syndrome due to a strategic lesion located in the superior and middle temporal gyrus and compare our findings with those of a 11C-Pittsburgh compound B PET (PiB-PET) positive lv-PPA patient matched by age, gender, and education. We consider that our study provides new anatomical clues to better understand the cognitive mechanisms underlying the logopenic syndrome.
CASE DESCRIPTION
A 57-year-old right-handed patient with no relevant medical history apart from mild hypercholesterolemia, presented to our Dementia Clinic with progressive word finding difficulties. He reported that these deficits had begun one year earlier. Apart from some mild fixation memory difficulties, he denied other cognitive symptoms. The general neurological examination was unremarkable. Systemic exploration was also normal.
Ethics approval was obtained by the Ethics Committee. All patients included in the study signed the Informed Consent. The patient’s consent was obtained for publication.
The neuropsychological examination evidenced marked language alterations with moderate decreased spontaneous fluency and mild verbal comprehension difficulties, frequent phonological paraphasias, and very severe disability for repetition which was partially length dependent. Verbal fluencies were also decreased, particularly the phonemic one (3 “p” words in a minute). Naming was also severely impaired despite the fact that there was no evidence of “concept loss”. Regarding memory, short term memory was particularly more affected than visual or free recall memory. The rest of cognitive domains were relatively preserved with the exception of moderate executive dysfunction.
With a working diagnosis of lv-PPA, the patient was transferred to the speech therapy unit and a cranial magnetic resonance imaging (MRI) was requested. Surprisingly the MRI showed increased T2 and FLAIR signal at the left superior and medial temporal lobe associated with cortical thinning, consistent with an old embolic ischemic stroke (Fig. 1A, B). Even though the infarct itself could be responsible for the clinical picture, due to the apparent progression and the suspicion of an underlying neurodegenerative process, both an 18Fluor-fludeoxyglucose PET (FDG-PET) and a PiB-PET were performed to assess brain glucose metabolism and amyloid-β deposition respectively. PiB-PET did not demonstrate brain fibrillar amyloid accumulation (Fig. 1C). FDG-PET showed a small area located at the left temporal lobe, with absence of glucose metabolism that perfectly correlated with the MRI lesion (Fig. 1D). On this basis, a final diagnosis of strategic ischemic stroke was made. The patient was initially treated with platelet anti-aggregants and an extensive search for the stroke etiology was performed. An antiphospholipid syndrome was identified being aspirin replaced by acenocumarol. The remaining ancillary tests were allnormal.
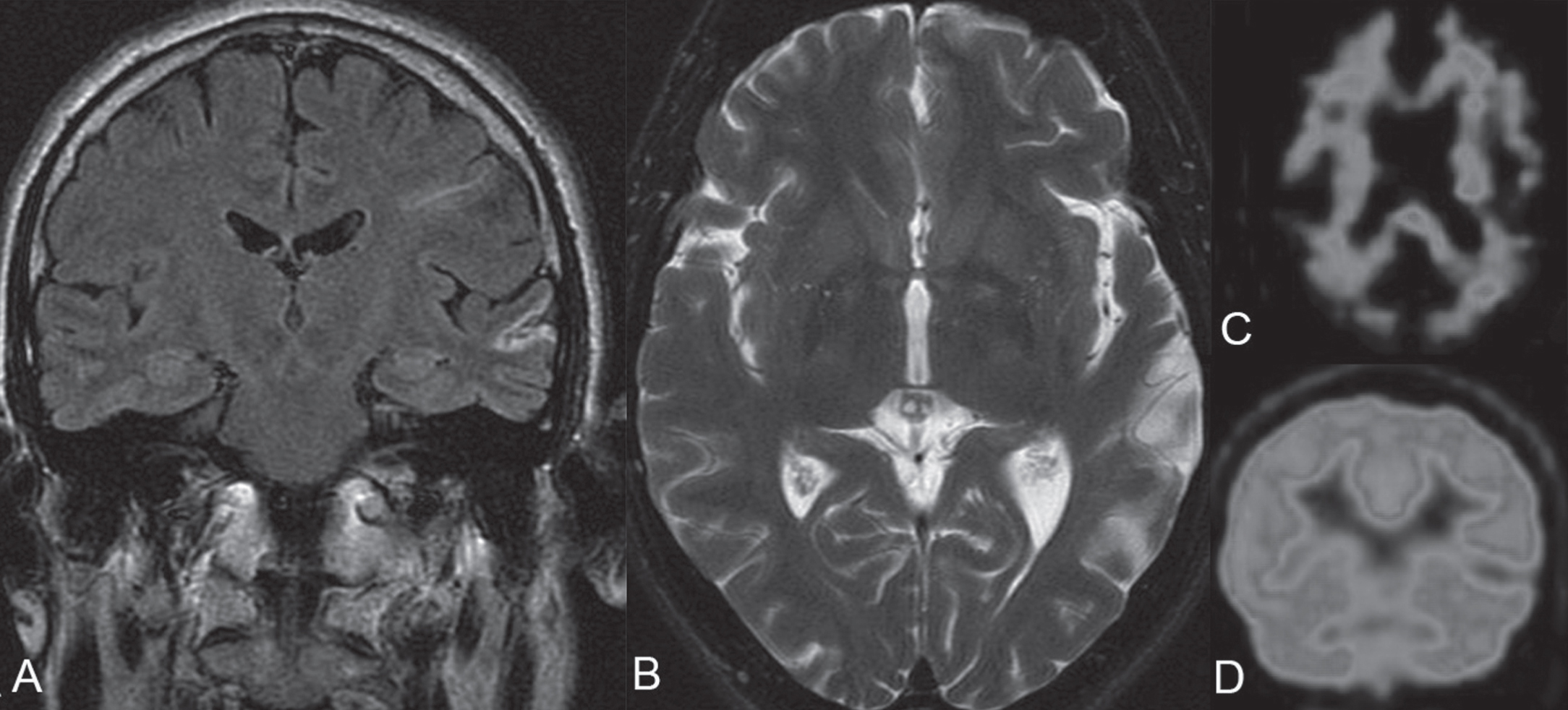
A) FLAIR cranial MRI sequence showing an ischemic cortical infarct located at the left medial and superior temporal cortex. B) T2-weighted cranial MRI sequence evidencing a hyperintense area located at the left temporal cortex consistent with an old ischemic stroke. C) 11C-PIB-PET image showing absence of amyloid-β brain deposition. D) 18Fluor-FDG-PET image demonstrating absence of metabolism at the left superior-medial temporal gyrus.
After 8 months of speech therapy, the patient demonstrated a significant recovery. A new neuropsychological exam evidenced more fluent spontaneous speaking with practically no paraphasias and marked improvement in naming and repetition. This recovery was confirmed in a new visit performed 28 months after the symptoms onset in which patient had almost come back to his basal situation.
COMPARISON WITH A TYPICAL LPA PATIENT
In order to better characterize our patient, we completed our study comparing our case with a PiB-PET positive lv-PPA patient matched by age, gender, and education. Voxel-based morphometry following standard procedures [8, 9] showed both cortical and white matter atrophy patterns mainly located at the left middle temporal and inferior parietal gyrus in the lv-PPA patient (Fig. 2). A group of 40 controls was used for the neuroanatomic comparison. Age, sex, and total intracranial volume were included as covariates. Statistical maps were thresholded at voxelwise p < 0.005, with a minimum cluster size of 200 voxels. Neuropsychological assessment showed that the lv-PPA patient and our stroke patient presented very similar cognitive performances with predominant deficits in verbal repetition, naming, verbal fluency, and digit span. By contrast, none of the patients exhibited profound episodic memory alterations (Fig. 3).
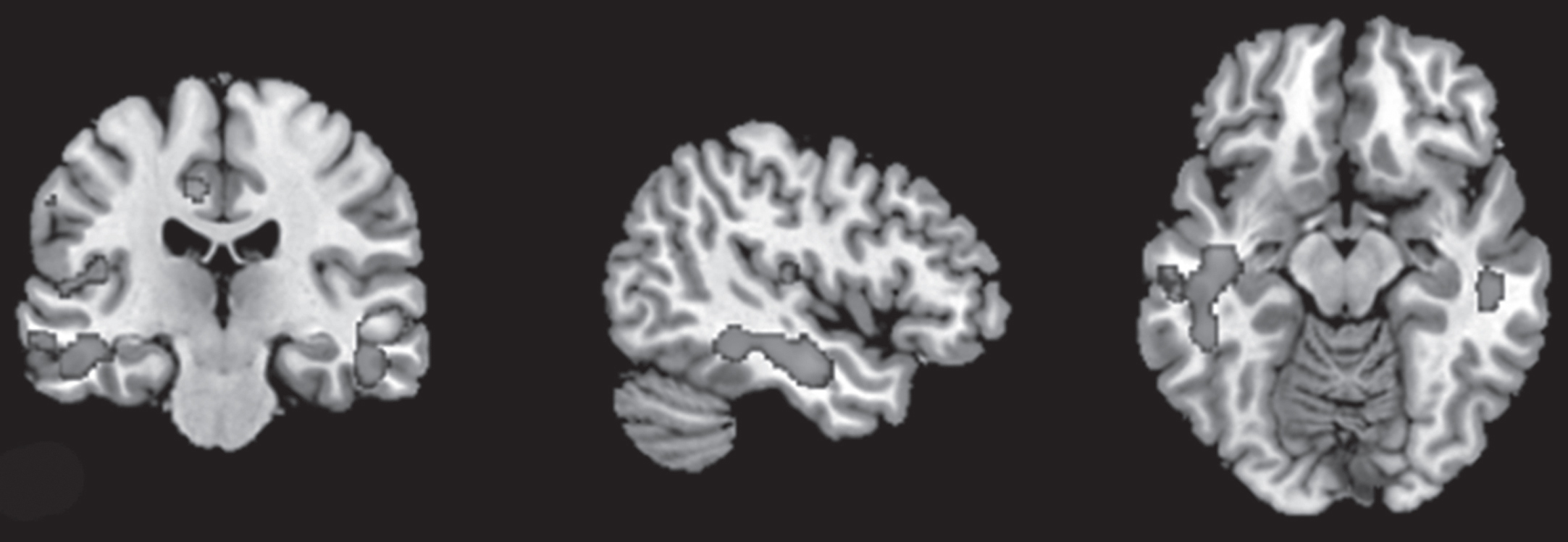
MRI analysis in a typical lv-PPA-AD patient compared with matched normative data, demonstrating both cortical atrophy and white matter atrophy.
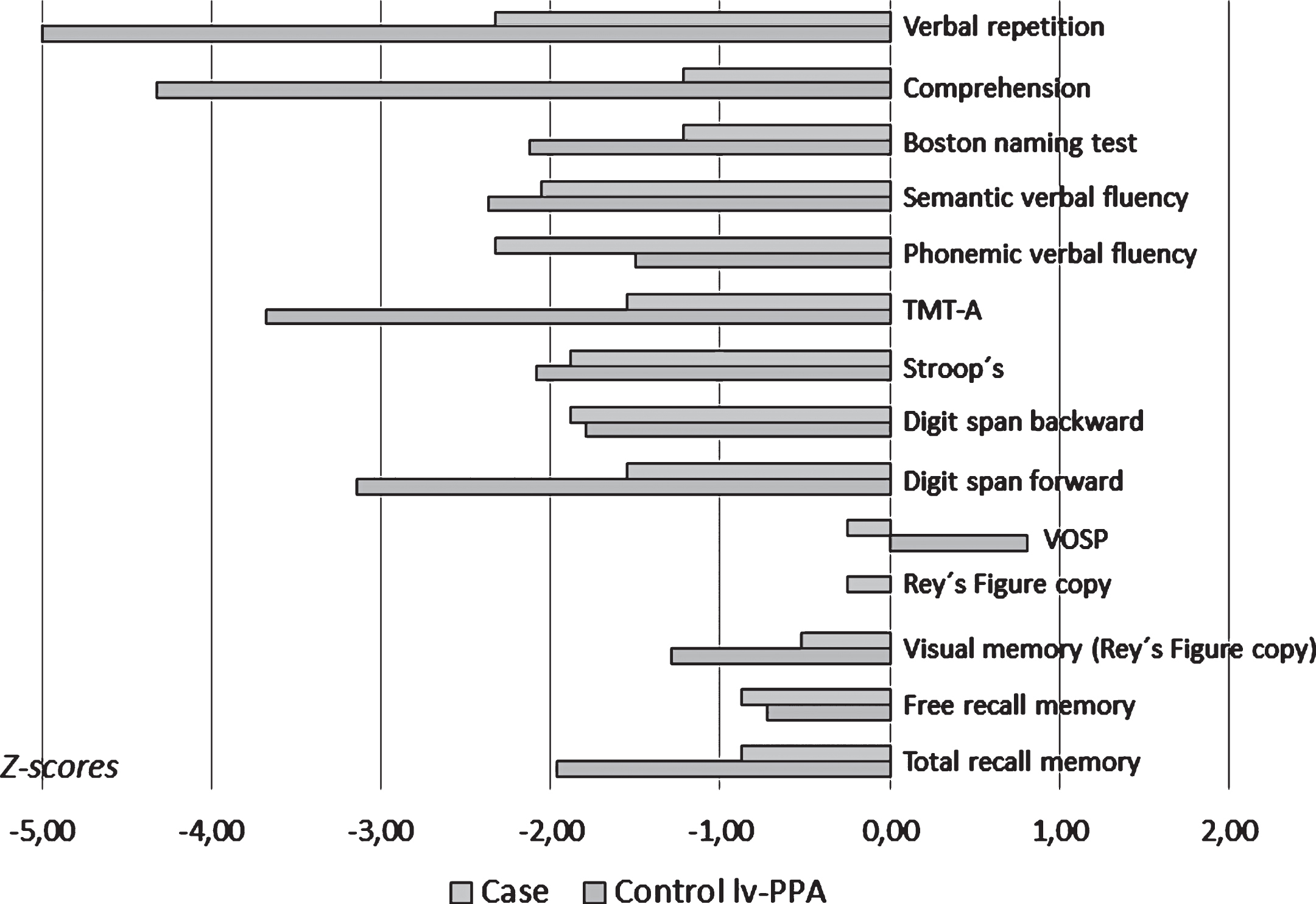
Neuropsychological profiles of the logopenic syndrome patient and a typical lv-PPA patient showing similar cognitive patterns.
DISCUSSION
Among PPAs, lv-PPA is the most common entity in AD patients. As mentioned above, lv-PPA patients are defined by slowed fluency with frequent phonological paraphasias and impaired word retrieval, naming, and repetition, with word comprehension usually less affected as occurred with our patient [1]. Regarding paraphasic disorders, semantic paraphasias are usually related to sensory dysphasia while phonemic paraphasias are commonly seen in patients as the one described in this article with motor-predominant dysphasic features.
Ischemic cerebral lesions constitute an important cause of dementia. In this context, depending on the affected region, cortical strokes can produce a wide constellation of symptoms such as executive dysfunction (medial frontal lobe), apraxia or agnosia (left parietal lobe), confusion, constructional and visuospatial difficulties (right parietal lobe), amnesia (medial temporal lobe), or language disorders [10, 11]. In addition, smaller strategic strokes located at thalamus have also been associated with several dementia syndromes. Finally, the accumulation of both lacunar infarcts and small vessel chronic ischemia affecting the deep cerebral nuclei and white matter can produce a progressive subcortical dementia syndrome [10, 11].
We consider this is a unique case of a patient with stroke presenting with a logopenic syndrome. Previously, other authors had reported patients with temporal stroke or other lesions of the temporal lobe presenting with conduction aphasia (CA) and also simulating a PPA [6]. First described by Wernicke in 1874, CA is a language disturbance characterized by relatively fluent spontaneous speech, abundant phonological paraphasias, and inability for repetition, while comprehension is usually spared [12]. Patients with CA may also have a wider constellation of symptoms such as reading and writing disturbances and others [12]. Classically, CA has been associated with damage in the arcuatus fasciculus [12, 13]. However, the possibility of several mechanisms, each of which could cause repetition disorders, has led to the postulation of two different forms of CA: suprasilvian (parietal) and infrasilvian (temporal) forms [14, 15]. The former primarily affects the phonemic organization and representation of words, whereas the latter, which involves the temporal lobe, mainly alters short-term memory and repetition [14, 15]. Although our case has some similarities with the temporal CA form, it has some features such as marked naming impairment which are not typically seen in CA. Therefore, we consider that it cannot be classified as a pure CA.
Each PPA subtype is characterized by specific deficits in language domains (grammatical and semantic processing, comprehension, fluency, and repetition). In this line, poor fluency has been associated with abnormalities of the inferior frontal sulcus and the posterior middle frontal gyrus, whereas grammatical processing (typically affected in nfv-PPA) may be the consequence of disorders of the inferior frontal gyrus. Semantic processing disorders (a key feature in sv-PPA patients) appear to be linked to anterior temporal lobes [16].
Regarding lv-PPA pathophysiology, a recently proposed theory is that deficits in word-retrieval and the repetition inability are due to damage in two different and non overlapping cortical regions [17]. Phonological skills in patients with PPA have been studied by several authors. Recently, Henry et al. confirmed the critical role of dorsal stream structures in phonological processing, demonstrating unique patterns of impaired phonological processing in patients with lv-PPA [18]. In another study, Leyton et al. studied a series of patients with lv-PPA reporting that naming deficits were associated with thinning of the left inferior parietal lobe, while sentence repetition impairment correlated with a loss of volume of the left superior temporal gyrus. The authors did not find a direct correlation between anomia and difficulties in word repetition, suggesting than the deficits were neurally independent [17]. Surprisingly, the present case differs from this conception. Although our patient only had an isolated strategic ischemic lesion located at the superior left temporal cortex, he doubtlessly manifested with impairment in both word retrieval and naming and inability for word repetition. Our findings thus support the idea that even though naming and phonological short term memory abilities are represented in different cortical regions, they are indeed interconnected, as a unique lesion impaired both of them. Future studies including larger number of participants and providing neuropathological data will be needed to confirm this hypothesis. Regarding MRI analysis, although single-subject voxel-based morphometry is not statistically ideal, it has proven to be a useful technique used in numerous studies of patients with neurodegenerative disease [19–21].
In conclusion, to our knowledge this is a unique case in the literature since it illustrates a strategic lesion that mimicked a lv-PPA syndrome, and therefore suggested the connection/relationship between phonological short term memory and naming.
DISCLOSURE STATEMENT
Authors’ disclosures available online (http://j-alz.com/manuscript-disclosures/16-1267r2).