
Abstract
INTRODUCTION
Mild cognitive impairment (MCI) is recognized as a prodromal stage of Alzheimer’s disease (AD). Epidemiological evidence revealed that MCI converts to probable AD with a 10%–15% yearly transition rate [1], whereas healthy elderly controls progress into dementia at a 1–2% annual conversion rate [2]. Early diagnosis of MCI and effective intervention might be pivotal to prevent further progression into AD.
Event-related potential (ERP) is a non-invasive tool with high temporal resolution and is often implemented to study the brain’s synaptic function. It instantly reflects the summated excitatory postsynaptic potential and inhibitory postsynaptic potential, principally of pyramidal cells in the neocortex [3]. Due to its high temporal resolution, ERP is advantageous in quantifying the sequence of different stages of cognitive processing. Previous investigations indicated that some ERP components in MCI are sensitive to cognitive decline and convert even prior to alterations of behavioral performance [4–7]. These investigations provided evidence to support that ERP components might be early electrophysiological diagnostic biomarkers for MCI [8]. In MCI-related ERP studies, primarily used tasks included: the classic odd-ball task, n-back task, Stroop task, Go/NoGo task, learning-recognition task, and Simon task. Variation in cognitive processing is essential for different tasks. In addition, various components are elicited at different stages of cognitive processing. Middle-latency ERP components (P50, P100, N100, P200, and N200), mismatch negativity (MMN), P300, N400, and P600 are important cognition-related ERP components and are explored extensively in ERP studies on MCI [9]. Additionally, previous studies showed suspicious deficits in these components in MCI patients [10–14].
P50, a positive component elicited approximately 50 ms after the onset of the stimulus, presents reduced amplitude due to repetitive stimuli. This phenomenon is called P50 suppression, which is considered to represent a sensory gating or inhibitory process [15]. Some investigations showed reduced P50 suppression in neurological and psychiatric disorders [16–18]. Visual P100 at the occipital area is related to the global processing of visual perception [19]. Auditory N100 is composed of a component derived from the auditory cortex and some other components [20]. P200 is traditionally known as an automatically produced exogenous response, but its amplitude and latency might change with selective attention [21]. N200, a negative component ranging from 180 ms to 350 ms after stimulus onset, is related to selective pre-attentive stimulus evaluation and discrimination [22]. N2pc, a negative N2 subcomponent distributed at posterior electrodes, is associated with the attentional selection of stimuli [23, 24]. MMN, including auditory MMN (aMMN) and visual MMN (vMMN), is attained by deducting ERP elicited by standard stimuli from that elicited by deviant stimuli during the odd-ball task. It is a negative component appearing approximately 160 ms to 200 ms after stimulus onset and is likely to be produced by an automatic novelty-sensing process rather than attention tostimuli [25].
P300, composed of P300a and P300b (classical P300) subcomponents, is a positive component peaking between 300 ms and 500 ms after stimulus onset. P300a mainly distributes at frontal electrodes and is related to automatic attention processing. P300b, the classical P300, is elicited by the update of working memory and distributes primarily at parietal electrodes [26]. N400 is important to reflect semantic processing [27]. P600, also known as the late positive component, is related to memory encoding and retrieval [28]. Additionally, the old/new effect, obtained by subtracting the ERPs elicited by new items from those elicited by old items, is a more important biomarker compared to N400 and P600 in ERP studies related to semantic and episodic memory [29]. According to previous studies, the old/new effect of three major subcomponents is reported to be associated with recognition memory [29, 30]: (1) Early frontal effect, a positive subcomponent peaking between 300 and 500 ms after stimulus onset and maximal at frontal-central sites, reflects the familiarity process in recognition memory [31, 32]; (2) Parietal old/new effect subcomponent, a positive subcomponent peaking between 500 and 800 ms after stimulus onset and maximal over the left parietal-occipital scalp, reveals recollection [31, 32]; and (3) Late frontal effect, a positive slow wave peaking 800 to 1000 ms post-stimulus at right frontal sites, is related to post-retrieval processing [33].
However, over the past 30 years, ERP has not realized its full potential in diagnosing AD or MCI. In addition, comparative analysis of these components in MCI and healthy controls (HC) obtained inconsistent results in different investigations. Thus, a systematic review of these components in MCI patients is essential. In our investigation, we aim to perform a systematic review and meta-analysis of ERP studies on MCI patients to explore potential electrophysiological biomarkers on MCI. This was the first study to summarize all the MCI-related ERP investigations.
METHODS
Search strategy
We searched for articles published on the PubMed and Web of Science databases from April 1986 to August 2016. The search terms used were: (“mild cognitive impairment” OR “MCI”) AND (“event-related potential” OR R “ERP”). All publications were in English, and a total of 612 studies were retained, with the exception of duplicates.
Inclusion criteria and exclusion criteria
We retained articles that compared the mean amplitude, peak amplitude, and peak latency of ERP components between HC and MCI patients. Studies pertaining to conditions other than MCI were rejected. In addition, reviews, meta-analyses, and case studies were removed.
Data collection
Finally, 42 ERP studies were reviewed. The following data were recorded from the full texts of these ERP studies: Author, publication year, participant demographics (sample size, age, gender, year of education, and Mini-Mental State Examination [MMSE]), experimental task, ERP component and its window, and study results.
Meta-analysis for ERP studies
The standard mean difference (SMD) and 95% confidence intervals (CI) were computed as the effect size of each ERP component explored by ≥3 ERP studies. The Q test was used to estimate heterogeneity between studies, and I2 was computed to assess the amount of variation derived from heterogeneity. Random effects models were performed to generate summary effect size when the heterogeneity of these studies was invariably high (Q test, p≤0.05). Inversely, fixed effects models were performed to summarize the effect size in the absence of between-study heterogeneity. To explore heterogeneity, we regressed the SMD against publication year and subject characteristics (age, gender, educational level, MMSE) with meta-regression analysis. In addition, we performed subgroup analysis to detect the effect of heterogeneous tasks on the heterogeneity of the meta-analysis. Moreover, we applied Begg’s test, Egger’s tests, and funnel plots to assess the risk of publication bias. All these statistical analyses were implemented with STATA 12.0 software.
RESULTS
Search results
Figure 1 shows the initial research and gradual exclusion procedures. Study characteristics and results are summarized in Supplementary Table 1. We summarize the 42 ERP studies on MCI patients. There were n = 5 and n = 3 studies, respectively, that compared P50 amplitude and latency between HC and MCI. In addition, there were n = 3 studies exploring MCI-related alterations of the P100 component. n = 5 and n = 4 investigations, respectively, evaluated MCI-related alterations of N100 amplitude and latency. MCI-related P200 amplitude and latency changes were studied in n = 7 studies. MCI-related N200 amplitude and latency alterations were assessed in n = 13 and n = 15 studies, respectively. n = 3 studies explored MCI-related alterations of the N2pc component. There were n = 4 and n = 3 studies comparing MMN amplitude and latency between HC and MCI, respectively; P300 amplitude and latency changes were evaluated in n = 18 and n = 17 investigations, respectively.
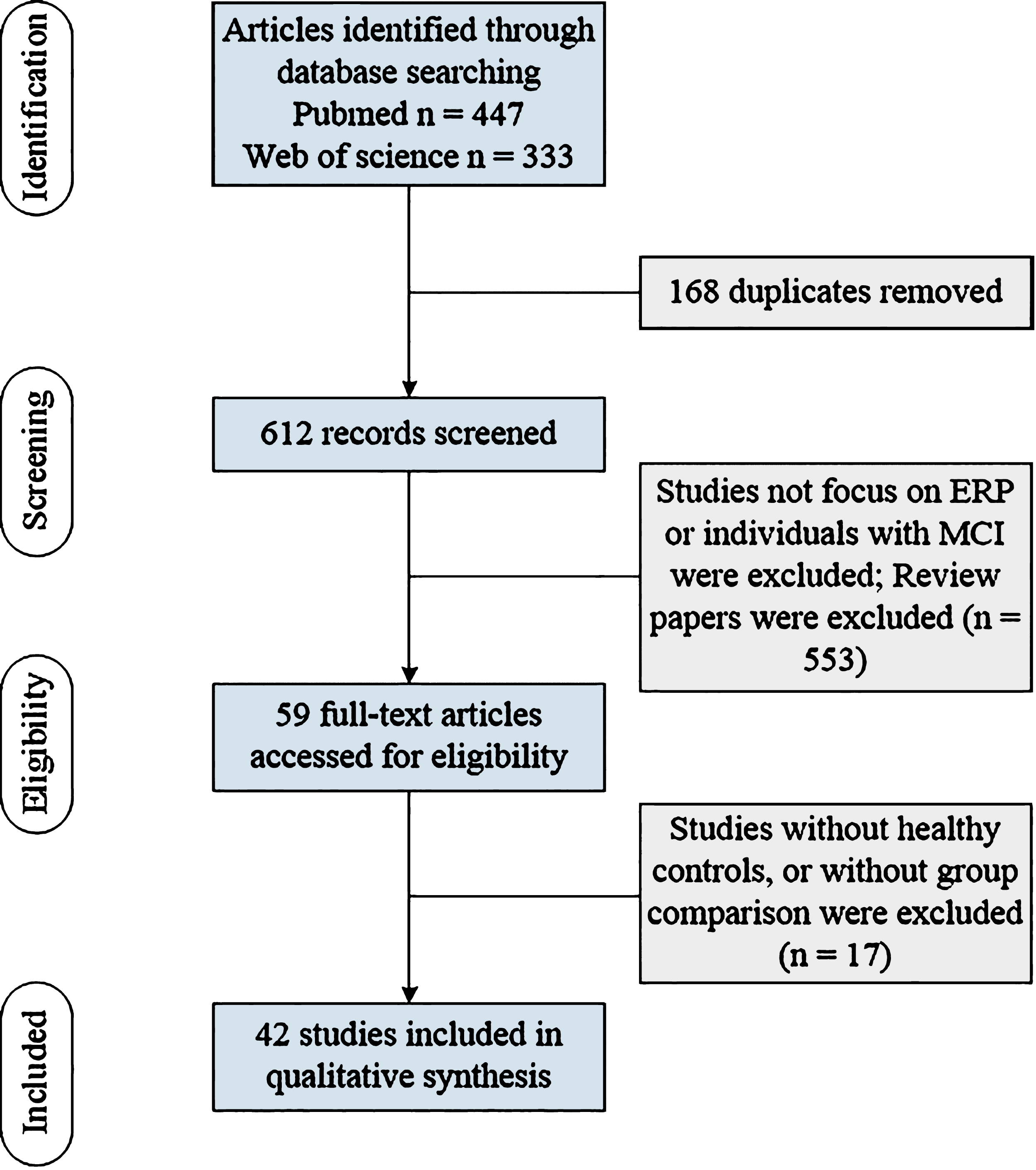
Flow of information through the different phases of a systematic review.
Meta-analysis results for ERP studies
Our meta-analysis results showed enhanced P50 amplitude at the Cz site and reduced N2pc amplitude in MCI patients compared to HC (see Fig. 2A and F). In addition, P100, N100, P200, N200, MMN, and P300 amplitudes showed no significant difference between MCI patients and HC (see Fig. 2B-E, G, H). Moreover, our study revealed prolonged P200 latency at the Cz site, N200 latency at the Cz, Pz sites, and P300 latency at the Cz, Pz sites in MCI patients compared to HC (see Fig. 3D, E, H). This study detected significant heterogeneities between ERP-related studies for P50, N100, P200, N200, N2pc, P300 amplitude and P50, P200, N200, N2pc, MMN, P300 latency. Our meta-regression study revealed that publication year and participants’ characteristics (age, gender, educational level, MMSE) did not contribute to the significant heterogeneities between different studies. In addition, Begg’s test, Egger’s tests, and funnel plots showed no significant publication bias in any ERP components.
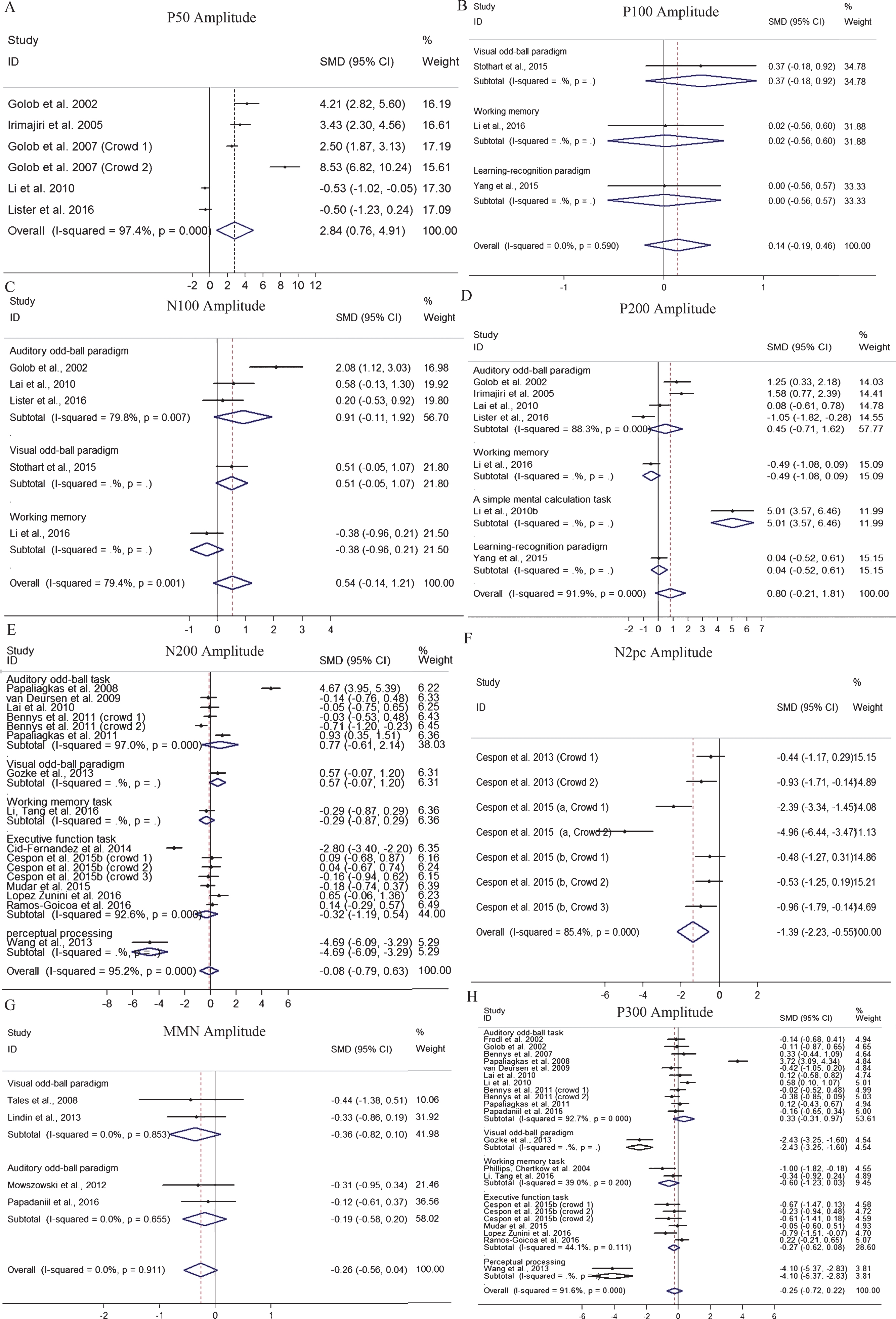
A-H) Forest plot of the P50, N100, P100, P200, N200, N2pc, MMN and P300 amplitude in MCI-related ERP studies. Diamonds denoted SMD and 95% CI; positive values indicated increased amplitude in MCI patients, while negative values indicted increased amplitude in HC. CI, confidence interval; ERP, event-related potential; HC, healthy controls; MCI, mild cognitive impairment; MMN, mismatch negativity; SMD, standard mean difference.

A-H) Forest plot of the P50, N100, P100, P200, N200, N2pc, MMN and P300 latency in MCI-related ERP studies. Diamonds denoted SMD and 95% CI; positive values indicated increased amplitude or prolonged latency in MCI patients, while negative values indicted increased amplitude or prolonged latency in HC. CI, confidence interval; ERP, event-related potential; HC, healthy controls; MCI, mild cognitive impairment; MMN, mismatch negativity; SMD, standard mean difference.
Systematic review of ERP studies during different tasks
Figure 4 shows the details for each component in each task. In 15 ERP studies with the auditory odd-ball task, consistent results reported no significant difference between MCI patients and HC in N100 amplitude and latency at the Cz site, P200 latency at the Cz site, MMN latency at the Fz, Cz, Pz, and slow wave amplitude at the Cz and Pz sites. It also reported the consistent result that MCI patients showed delayed slow wave (SW) latency at Cz and Pz sites relative to HC. In addition, the included studies showed inconsistent results in comparison in the P50 amplitude and latency, P200 amplitude, N200 amplitude and latency, MMN amplitude, and P300 amplitude and latency between MCI and HC. Meta-analysis detected elevated P50 amplitudes at the Cz site in MCI patients compared to HC (see Fig. 2A). Additionally, subgroup meta-analysis indicated that MCI patients showed delayed N200 latency at the Cz, Pz sites and P300 latency at the Cz, Pz sites relative to HC during the auditory odd-ball task (see Fig. 2E, H). However, P50 latency at the Cz site, P200 amplitude and latency at the Cz site, N200 amplitude at the Cz, Pz sites, and P300 amplitude at the Cz, Pz sites did not differ between HC and aMCI patients (see Figs. 2D, E, H and 3A, D).
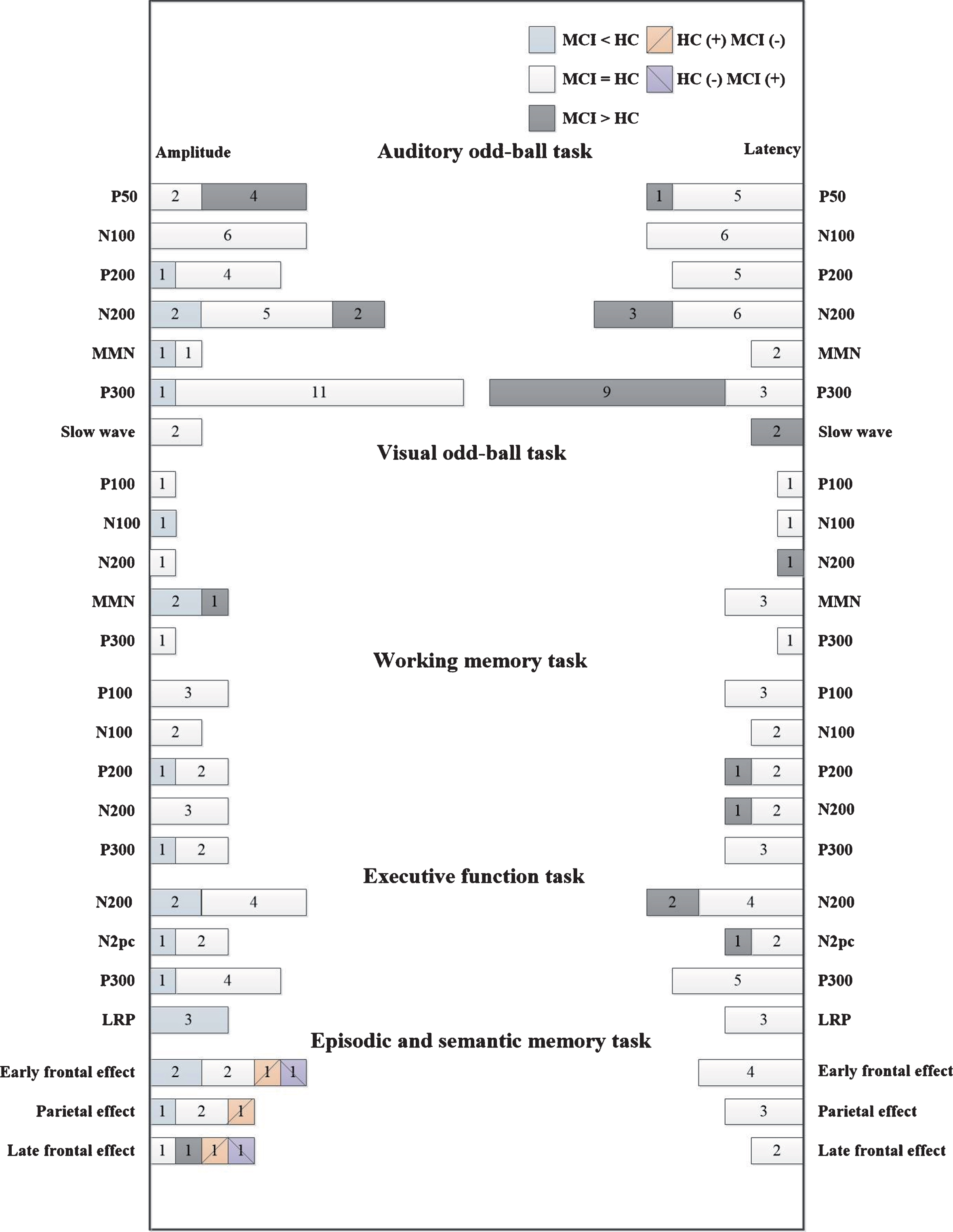
Overview of ERP studies with different tasks in MCI. Notes: MCI = HC indicated no significant difference in amplitude or latency between MCI and HC; MCI <HC indicated reduced amplitude in MCI patients, compared to HC; MCI >HC indicated increased amplitude or delayed latency in MCI patients relative to HC; HC (+), MCI (–) showed that the component was elicited in HC but not in MCI; HC (–), MCI (+) showed that the component was elicited in MCI but not in HC. ERP, event-related potential; HC, healthy controls; LRP, lateralized readiness; MCI, mild cognitive impairment; MMN, mismatch negativity.
The three ERP studies with the visual odd-ball task showed the consistent result that no significant difference was detected in MMN latency at posterior sites between MCI patients and HC. Lindin et al. and Stothart et al. revealed that MCI patients showed lower MMN amplitude at the central, parietal, and occipital sites compared to the HC group [34, 35], whereas Tales et al. reported increased MMN amplitude at occipital sites in MCI patients compared to HC [36].
In working memory-related ERP investigations, the results indicated no significant alterations in P100 amplitude and latency, N100 amplitude and latency, or N200 amplitude and P300 latency. However, these studies showed discrepant results in MCI-related P200 amplitude and latency, N200 latency, and P300 amplitude alterations. Li et al. detected decreased P200 and P300 amplitudes in MCI patients compared to HC, whereas no significant differences in P200 and N200 latencies were indicated between the two groups [37]. Missonnier et al. revealedprolonged P200 and N200 latencies in MCI-Converters compared to HC, whereas no significant differences in P200 and N200 latencies were detected between MCI-Stable and HC [38]. In addition, Missonnier et al. indicated no significant differences in P200 amplitude between MCI and HC [38]. Furthermore, Phillips et al. revealed no significant difference in P300 amplitude between MCI andHC [39].
Studies associated with executive function revealed concordant results indicating a lack of difference in P300 latency and lateralized readiness (LRP) latency between MCI patients and HC. In addition, concurrent studies indicated reduced LRP amplitude in MCI patients compared to HC. Subgroup meta-analysis reported that MCI patients displayed reduced N2pc amplitude and delayed N200 latency compared to HC (see Figs. 2F and 3E). However, N200 amplitude, N2pc latency and P300 amplitude showed no significant difference between the two groups.
Regarding episodic and semantic memory, we focused on the old/new effect between two groups for components in three time windows mentioned in the introduction. Several incompatible results were presented, but most included investigations that elicited the old/new effect in both HC and MCI patients.
DISCUSSION
To our knowledge, our investigation is the first meta-analysis to evaluate all ERP components in MCI. It showed increased P50 amplitude at the Cz site, reduced N2pc amplitude and delayed P200 latency at the Cz site, N200 latency at the Cz, Pz sites, and P300 latency at the Cz, Pz sites in MCI patients relative to HC.
Reduced P50 suppression indicates deficits in filtering out irrelevant sensory stimuli, which might derive from deficits in inhibitory processes associated with attention modulation. Previous investigations revealed that P50 amplitude at the Cz site is higher at baseline in MCI-Converters compared to MCI-Stable [10, 40]. In addition, multiple-domain aMCI (md-aMCI) showed increased P50 amplitude at the Cz site than single-domain aMCI (sd-aMCI) [40]. Moreover, a relatively recent study revealed a significantly negative correlation between P50 amplitude at Cz and amyloid-β 42 levels in cerebrospinal fluid [41]. Furthermore, Irimajiri et al. showed reduced P50 amplitude in cholinesterase inhibitor-treated MCI patients compared to untreated MCI patients [42]. Coupled with our analysis, these studies revealed the important role of P50 amplitude in recognizing MCI patients, monitoring disease progression, and predicting disease prognosis.
P200 latency is associated with selective attention or stimulus encoding processes [21]. Missonnier et al. indicated delayed P200 latency at baseline in MCI-Converters compared to MCI-Stable [38], which proves that P200 latency can predict MCI progression. Regarding N200 and P300 latencies, our result was consistent with two recent meta-analysis studies, which showed prolonged N200 and P300 latencies in AD and MCI patients compared to the HC group [43, 44]. In addition, recent studies found that N200 and P300 latencies might be two accurate and sensitive indices for predicting the progression of MCI [6, 22]. The abnormality might be attributed to deficientpre-attentive stimulus evaluation and short-term memory processing [12, 43]. However, it is notable that our meta-analysis for N200 and P300 neglected the two components in the NoGo condition in Go/NoGo task. N200 and P300 in the NoGo condition are associated with response inhibition rather than pre-attentive stimulus evaluation or short-term memory processing reflected by the two components in the Go condition and generated from different brain regions compared to those in the Go conditions [45–47]. We aimed to explore N200 and P300 associated with pre-attentive stimulus evaluation and short-term memory, respectively. Thus, our study summarized the two components just in the Go condition. In the summary of executive function-related ERP studies, MCI patients showed lower N2pc amplitude compared to HC. This revealed deficient attention, responses selection and execution in MCI patients.
Regarding the summary of semantic and episodic memory-related ERPs, it indicated the inconsistent results of three subcomponents of the old/new effect (early frontal effect, parietal effect, and late frontal effect) from different studies. The discordance might be attributed to differences in stimuli and the heterogeneity of educational levels in participants. The picture superiority effect and emotional content effect might be two key factors. The picture superiority effect refers to the status that picture stimuli are easier for the disease group to recall than word stimuli [48, 49], and emotional content has the same effect [29]. Thus, word and neutral content might be better stimuli for distinguishing the healthy and diseased groups. In addition, the educational levels of subjects are significant for recollection [50, 51]. Episodic memory is the first deficient cognitive domain in MCI. Thus, making a greater effort to find the appropriate stimuli and control the educational level of subjects might enhance the sensitivity of the old/new effect to recognize MCI patients.
Notably, our meta-analysis showed an interesting pattern of ERP component alterations with early sensory-evoked potentials typically normal in MCI (except abnormal P50), whereas potentials starting from ≥200 ms are more consistently abnormal in MCI, which is consistent with the results found in AD [9]. In addition, this pattern might be associated with the fact that AD-like neuropathology starts from the medial temporal gyrus, other limbic regions, and multimodal association cortices with the relative sparing of the unimodal sensory cortex. However, to provide more evidence for this hypothesis, we require further exploration of ERP components starting at approximately 400 ms and beyond (N400, P600, or old-new effect) during semantic and episodic memory-related tasks.
Our study detected significant heterogeneities between different investigations. However, meta-regression analysis showed no significant results. It is possible that age, gender, educational level, and MMSE equally affected these subcomponents in both groups [52]. Additionally, in the diagnosis of MCI, most researchers depend on clinical evaluation and cognitive tests. These factors might partially contribute to these heterogeneities. Moreover, differences in task might be another source of heterogeneity.
For some subcomponents, such as P50, P100, N2pc and MMN, the strongest limitation is the small sample size in the meta-analysis. Thus, these meta-analyses could not overcome the limitation of individual research studies.
In summary, our study indicated that some ERP components, such as P50 and N2pc amplitude, P200, N200 and P300 latency, might be potential electrophysiological biomarkers for MCI diagnosis.