
Abstract
INTRODUCTION
Dementia refers to a broad family of disorders that affect memory, thought processes, and social interactions, indirectly leading to a disturbance in daily life [1]. In 2015, the World Health Organization estimated that almost 48 million people throughout the world are affected by dementia and that this number may potentially increase to 76 million in the next two decades [1]. In Germany, dementia is found in around 1.2 million patients, and 200,000 patients are newly diagnosed with this mental disorder each year [2].It was further discovered that in this country the average related cost exceeds euro 43,000 per individual per year.
Anti-dementia drugs can be prescribed to dementia patients in order to decrease the severity of the symptoms associated with the disorder. High adherence and persistence are important for the efficacy of these treatments [3]. Unfortunately, several studies have found that adherence and persistence remain suboptimal in individuals diagnosed with dementia [4–8]. In 2010, Kröger and colleagues discovered that approximately 31% and 59% of dementia patients who received cholinesterase inhibitors discontinued their treatment after six months and three years of prescription, respectively [4]. Brewer et al. later corroborated these findings in their study including 20,729 Irish patients, as the rate of discontinuation was 30% after six months of therapy and 44% after one year [5]. The major factors associated with anti-dementia treatment non-persistence are age, gender, race, and socioeconomic status [9]. Since anti-dementia effects are positively associated with drug doses [10], it is recommended to prescribe the highest tolerated dosage [11]. Interestingly, few authors have suggested that ineffective and low doses may increase the risk of non-persistence in individuals with dementia [4, 12]. In 2010, Gardette and colleagues discovered that ineffective doses of cholinesterase inhibitors were associated with a 7-fold increase in the risk of switching anti-dementia therapies. Although these results are important, little is known about the impact of anti-dementia drug doses on adherence and persistence in Germany.
Therefore, the goal of the present study was to analyze the association between anti-dementia treatment persistence and daily dosage of the first prescription in German patients treated in neuropsychiatric practices.
METHODS
Database
The Disease Analyzer database (IMS HEALTH) compiles drug prescriptions, diagnoses, and basic medical and demographic data obtained directly and in anonymous format from computer systems used in the practices of general practitioners (GP) and specialists [13]. Diagnoses (ICD-10), prescriptions (Anatomical Therapeutic Chemical (ATC) Classification System), and the quality of reported data have been monitored by IMS based on a number of criteria (e.g., completeness of documentation and linkage between diagnoses and prescriptions).
In Germany, the sampling methods used for the selection of physicians’ practices were appropriate for obtaining a representative database of general and specialized practices [13]. Prescription statistics for several drugs were very similar to data available from pharmaceutical prescription reports [13]. The age groups for given diagnoses in Disease Analyzer also matched well with those in corresponding disease registries [13]. Finally, the Disease Analyzer database has already been used to perform studies on dementia [7, 14–16].
Study population
This study included patients with Alzheimer’s disease (ICD-10: G30) aged 60 years or over who received anti-dementia prescriptions (galantamine, donepezil, memantine, or rivastigmine) for the first time between 2005 and 2014 in 175 neuropsychiatric practices in Germany. Follow-up lasted until December 2015. A total of 15,503 patients were available for analysis.
Study outcome
The main outcome measure was the treatment persistence rate within 12 months after the index date as a function of the daily dose of the first prescription. For each prescription, the database gives only one measure of the prescribed dosage. It is therefore not possible to assess dose escalation over the course of one prescription (although comparisons between prescriptions are feasible). Since, a dose increase over the course of the first prescription is not only possible but also likely, the daily dosages for the first prescriptions were compared with the manufacturer’s recommendations. It was found that the prescribed daily doses for the first prescription were more likely to correspond to the dosage at the end of this prescription than at its beginning. It is therefore impossible to assess whether this was the starting dose on day one of treatment or whether the patient reached this dose from a lower level onthe first treatment day.
For each prescription, the expected duration (assuming total consumption of the entire prescription) was calculated on the basis of the doctor’s dosage recommendation, package size, and number of packages in the prescription. A longitudinal medication supply dataset was thereby established for each individual patient, and non-persistence with anti-dementia drugs was further calculated. Treatment discontinuation was defined as a period of 180 days without anti-dementia therapy. All patients were monitored for one year from their index date to identify treatment discontinuation. Demographic covariables included age, gender, and type of residence (home versus nursing home).
Statistical analyses
Kaplan-Meier analyses were performed to study treatment persistence as a function of anti-dementia treatment doses. Cox proportional hazards regression models were used to estimate the relation between persistence and first prescription daily dose after adjusting for age, gender, and residence in nursing homes. p values <0.05 were considered statistically significant. Analyses were carried out using SAS version 9.3.
RESULTS
Socio-demographic data pertaining to the patients are shown in Table 1. There were 2,442, 5,669, 4,416, 642, and 2,334 patients who were prescribed galantamine, donepezil, memantine, oral rivastigmine, and patch rivastigmine, respectively. Mean ages ranged from 78.0 years (SD = 7.7 years) to 80.6 years (SD = 8.0 years). In the different groups included in the present study, between 32.4% and 58.7% of patients were men, and between 16.5% and 32.0% of patients lived in nursing homes. Kaplan-Meier curves are displayed in Figs. 1–5. After 12 months of follow-up, continuation rates were similar for individuals using different doses of galantamine (8, 16, and 24 mg; p-value = 0.079), donepezil (5 versus 10 mg; p-value = 0.113), oral rivastigmine (1.5, 3, 4.5, and 6 mg; p-value = 0.228), and patch rivastigmine (4.6 versus 9.5 mg; p-value = 0.728), but were significantly different for memantine (10 versus 20 mg, p-value<0.001). The results of the Cox regression models are displayed in Table 2. Patients using 20 mg of memantine were less likely to discontinue their treatment than patients using 10 mg (HR = 0.88, 95% CI: 0.80–0.96). No significant association was found between first therapy dose and persistence for the other drugs (HRs ranging from 0.86 to 1.15).
Baseline characteristics of the dementia patients included in this study
Association between treatment discontinuation and first drug dose: Results of the Cox regression analyses
*adjusted for age, gender, and nursing home residence.

Kaplan-Meier curves for the time to discontinuation of therapy in dementia patients treated with galantamine as a function of first dose.
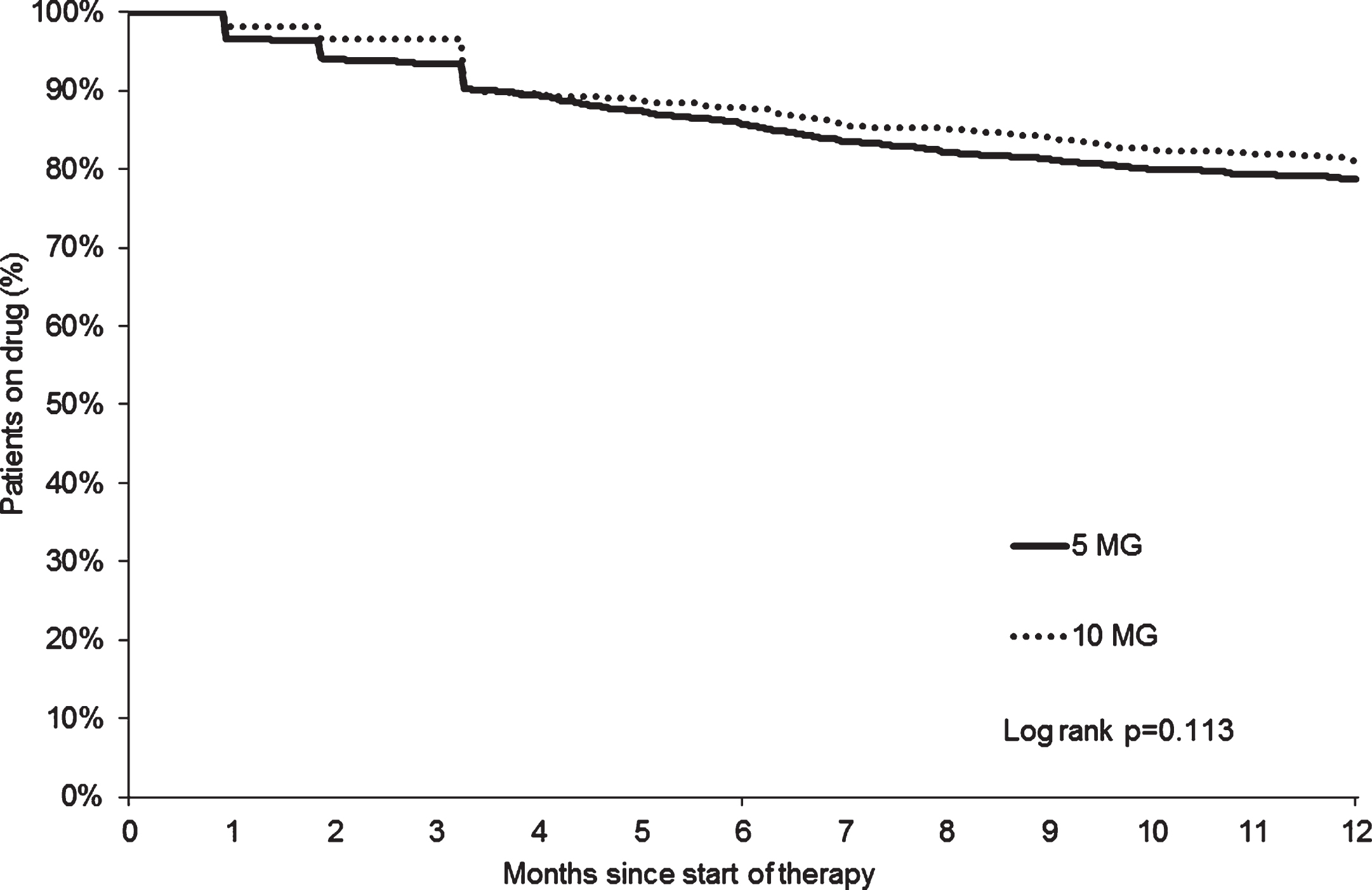
Kaplan-Meier curves for the time to discontinuation of therapy in dementia patients treated with donepezil as a function of first dose.
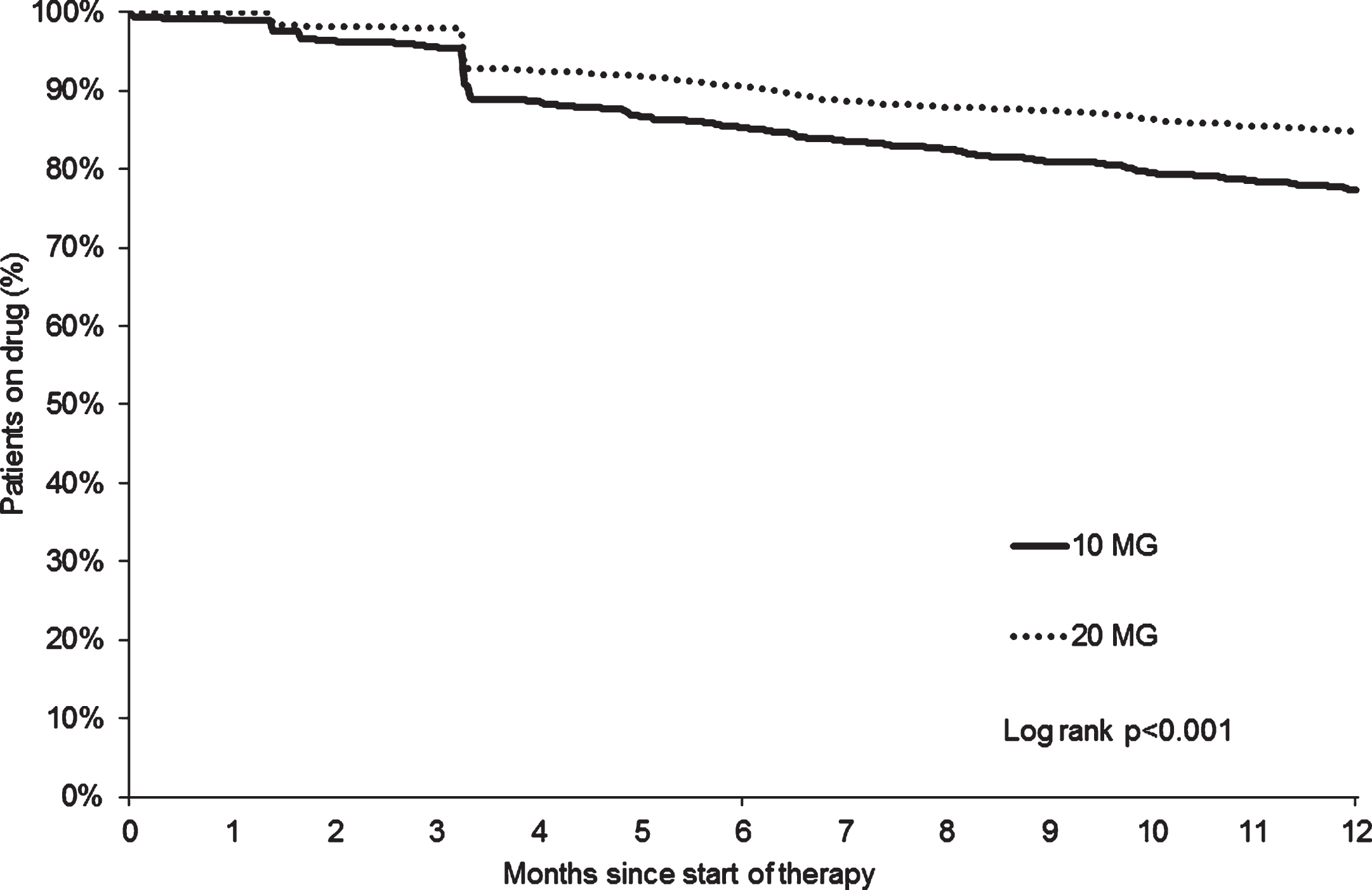
Kaplan-Meier curves for the time to discontinuation of therapy in dementia patients treated with memantine as a function of first dose.

Kaplan-Meier curves for the time to discontinuation of therapy in dementia patients treated with oral rivastigmine as a function of first dose.

Kaplan-Meier curves for the time to discontinuation of therapy in dementia patients treated with patch rivastigmine as a function of first dose.
DISCUSSION
The present German study of approximately 15,500 patients diagnosed with Alzheimer’s disease showed that persistence with anti-dementia treatments was higher than 75%–80% one year after therapy initiation. Furthermore, we discovered no significant association between persistence and first prescription daily dose in people treated with galantamine, donepezil, and rivastigmine. In contrast, individuals treated with 20 mg of memantine were at a lower risk of discontinuation than those receiving 10 mg.
Although Alzheimer’s disease is not curable, anti-dementia treatments can be prescribed to reduce the severity of its symptoms (i.e., agitation, sleep disturbance, or depression), thus improving the quality of life of individuals affected by this chronic condition. To have a positive impact on dementia, such treatments need to be taken on a long-term basis. Unfortunately, several authors have found that adherence and persistence with these molecules remain suboptimal [4–8]. In 2010, Kröger and colleagues discovered in 3,369 Dutch patients receiving cholinesterase inhibitors that 31% and 59% of them had discontinued their treatment six months and three years after initiation, respectively [4]. Interestingly, the same analysis showed that low doses of rivastigmine and galantamine were associated with an increase in the risk of non-persistence compared with regular doses of rivastigmine. In contrast, regular doses of galantamine led to a significant decrease in this risk. Finally, the authors estimated that a lower share of people treated with rivastigmine (35%) reached the WHO-defined daily dose compared with people who were prescribed galantamine (80%), potentially revealing the fact that side effects were more frequent with rivastigmine than with galantamine. That same year, Gardette et al. aimed to identify the predictive factors of discontinuation and switch of cholinesterase inhibitors in elderly people affected by dementia and living in the community [6]. The authors discovered that 100 out of 611 subjects had switched or discontinued their prescriptions after two years of follow-up. Ineffective doses of cholinesterase inhibitors were found to be the strongest risk factor for switching (HR = 6.91, 95% CI: 3.08–15.49), while hospitalization was found to be the most important factor contributing to discontinuation (HR = 9.14, 95% CI: 2.69–31.07).
Later, Brewer et al. showed that approximately 20,700 patients in Ireland received anti-dementia prescriptions between January 2006 and December 2010 [5]. A subsequent analysis of donepezil and memantine prescription patterns underlined the fact that, although most of the patients had taken these molecules at the maximum dose, such high doses were maintained in two consecutive months in only two-thirds of patients. Furthermore, the elderly and patients receiving rivastigmine were less compliant and persistent than younger individuals and those receiving donepezil. It was also discovered that non-persistence was lower in people who began therapy in more recent years and in those receiving multiple anti-dementia medications. This Irish study finally found that persistence was improved in patients who had been co-prescribed both memantine and donepezil.
More recently, in 2015, Bohlken and colleagues discovered in 12,910 outpatients in Germany affected by dementia that almost 60% of them continued their treatment after one year of follow-up [3]. It was found that individuals with donepezil or memantine were more likely to be persistent than those with rivastigmine. The same work estimated that people followed in specialist practices were at a lower risk of discontinuation than people followed in general practices. Finally, young men, patients with private health insurance, and individuals with a diagnosis of heart failure or hypertension at baseline had a higher chance of being persistent.
Contrary to the findings of Kröger et al. [4], the present German study estimated that there was no significant association between first prescription daily dose and persistence in patients receiving rivastigmine, donepezil, or galantamine. Interestingly, several authors have previously found that different doses of these molecules display similar tolerability profiles. In 2001, Wilkinson and Murray discovered that the rate of adverse outcomes was relatively similar between patients taking 18 mg of galantamine per day and those taking 24 mg [17]. These findings were later corroborated by Aronson et al., who showed that galantamine dosages of 16 mg and 24 mg per day were both well tolerated by all dementia patients [18]. In the case of donepezil, although a meta-analysis of randomized controlled trials has suggested that the rate of side effects was slightly higher with 10 mg than with 5 mg, the rates of completion were again similar [19]. When side effects were analyzed separately, the authors further found that only the minor adverse outcomes were more frequently found in individuals taking 10 mg donepezil than in those taking 5 mg. Finally, in 2013, Farlow and colleagues discovered in 716 patients diagnosed with severe Alzheimer’s disease that the share of adverse events was identical between the group receiving 13.3 mg of rivastigmine (patch) per day and the group receiving 4.6 mg [20]. In the present study, no side effect could be estimated due to missing documentation about side effects. Further result of this German retrospective analysis is that individuals treated with 10 mg of memantine were at a higher risk of non-persistence than those receiving 20 mg. Even if this last finding must be interpreted with great caution, it is possible that the use of 20 mg memantine was associated with a greater improvement of cognitive functions than the use of 10 mg memantine, indirectly improving the adherence and the persistence of the patients. In 2002, Orgogozo and colleagues estimated in a French randomized, placebo-controlled trial including patients with mild to moderate vascular dementia that the daily use of 20 mg memantine during 28 weeks significantly improved cognitive abilities [21]. Later, a 2013 study showed that the same dose of memantine led to significant benefits in terms of cognition, function, and global status in patients diagnosed with Alzheimer’s disease and already treated with a cholinesterase inhibitor (donepezil), supporting the idea that 20 mg potentially displays the most advantageous risk-benefit balance [22].
This study is subject to several limitations. First, the database does not contain information about dose escalation. The first dose analyzed in this study is the prescribed daily dose documented by the physician. As all antidementive drugs are slowly escalated according to labeling and guidelines for the treatment of dementia, we assume that this first prescribed daily dose is a function of the prescription history during the first months of prescription. However, no information about dose development in the first months is available. Another important limitation was that data regarding side effects and adverse outcomes were missing. For example, it is possible that patients at a particular risk of developing side effects with choline esterase inhibitors may not undergo drug escalation with these molecules in clinical practice without fixed excalation plans, and may drop out on lower drug dosages.
Furthermore, the assessment of the Alzheimer’s disease diagnosis was based solely on ICD codes entered by neuropsychiatrists. Data on socioeconomic status and lifestyle-related risk factors were also unavailable.
One strength of this study is the large number of patients available for analysis. Another strength is the use of real-world data in physician practices where diagnoses and prescriptions are continuously documented, allowing for unbiased exposure assessment (no recall bias).
The present German retrospective study showed that there was no association between treatment persistence and first drug dose in patients with Alzheimer’s disease who were treated with rivastigmine, donepezil, or galantamine. In contrast, higher doses of memantine had a positive impact on persistence compared with lower doses. Further research is needed to gain a better understanding of the relation between persistence and first dose in patients affected by dementia.