
Abstract
Background:
Impaired cardiac function has been related to accelerated cognitive decline in late-life.
Objective:
To investigate whether higher levels of high sensitivity cardiac troponin T (hs-cTnT), a sensitive marker for myocardial injury, are associated with worse cognitive function in the oldest old.
Methods:
In 455 participants of the population-based Leiden 85-plus Study, hs-cTnT was measured at 86 years. Cognitive function was measured annually during four years with the Mini-Mental State Examination (MMSE).
Results:
Participants in the highest gender-specific tertile of hs-cTnT had a 2.0-point lower baseline MMSE score than participants in the lowest tertile (95% confidence interval (CI) (95% CI 0.73–3.3), and had a 0.58-point steeper annual decline in MMSE during follow-up (95% CI 0.06–1.1). The associations remained after adjusting for sociodemographic and cardiovascular risk factors excluding those without a history of overt cardiac disease.
Conclusion:
In a population-based sample of the oldest old, higher levels of hs-cTnT were associated with worse cognitive function and faster cognitive decline, independently from cardiovascular risk factors and a history of overt cardiac disease.
INTRODUCTION
Cardiac troponin T (cTnT) is a protein regulating the calcium-mediated actin and myosin interaction in cardiac myocytes [1]. Within hours after myocardial ischemia, blood levels of cTnT are markedly increased. Hence, a high level of serum cTnT is a clinical marker for acute myocardial ischemia and is therefore widely used in diagnosing acute myocardial infarction [2]. Recently, a high sensitivity (hs) assay for cTnT has become available for accurate measurement of concentrations below the clinical cut-off for myocardial infarction. In this range, higher levels of hs-cTnT in patients with heart failure [3, 4], renal failure [5], and acute pulmonary embolism [6], are related to worse disease-specific prognosis and increased mortality. Moreover, it has been shown in middle-aged and older community-dwelling persons without cardiovascular disease, that a graded increase in levels of cTnT are associated with cardiac events and mortality [7–9]. There is also a growing body of evidence that people with higher levels of hs-cTnT have a higher risk of non-cardiac adverse health outcomes such as stroke [10–12].
People with cardiovascular disease are at increased risk for cognitive decline and dementia [13–16]. Hence, higher levels of hs-cTnT, reflecting higher degrees of cardiac injury, may also be associated with accelerated cognitive decline and dementia. However, the available evidence on the relation between higher levels of hs-cTnT and adverse brain outcomes mainly comes from middle-aged and younger-old study populations [10–12]. It remains unclear whether in the rapidly expanding populations of very old people elevated levels of hs-cTnT associate with accelerated cognitive decline. Furthermore, the role of a history of overt cardiac disease in the relation between hs-cTnT and cognitive function has yet to be elucidated.
In this study of a population-based sample of the oldest old, we aimed to investigate whether higher levels of hs-cTnT are associated with worse baseline cognitive function and accelerated cognitive decline. Further, we assessed whether an association between hs-cTnT and cognitive function was also present in those without a history of overt cardiac disease.
METHODS
Design and participants
The design and recruitment procedure of the Leiden 85-plus Study have been described in detail elsewhere [17]. In brief, the Leiden 85-plus Study is a prospective population-based cohort study of inhabitants of Leiden, the Netherlands, who reached the age of 85 years between 1997 and 1999. No other eligibility criteria were applied. The response rate was 87% and 599 participants were enrolled. Data was collected annually during home visits. Since hs-cTnT was determined at the age of 86 years, we considered this age as the baseline measurement for our current study. The 455 participants with complete data on Mini-Mental State Examination (MMSE), hs-cTnT levels and covariates at the age of 86 were selected for our main analysis. The medical ethical committee of the Leiden University Medical Center approved the Leiden 85-plus Study, and all participants gave informed consent.
Measurement of high sensitivity cardiac troponin T
Hs-cTnT was measured from EDTA plasma using an electrochemiluminiscence immunoassay on a Roche Modular Analytics E170. The high-sensitivity assay has a detection limit of 3 ng/L and a 99th percentile cut-off of 14 ng/L. Because the Elecsys Troponin T hs assay used had a coefficient of variance (CV) of 10.38% at an hs-cTnT concentration of 10.0 ng/L, the assay was able to differentiate reasonably well at lower concentrations. For three participants with levels below the detection limit, hs-cTnT levels were set at 1.5 ng/L.
Measurement of cognitive function
Cognitive function was assessed with the MMSE at the age of 86 and then annually up until the age of 90 [18]. The MMSE ranges from 0–30 points with lower scores indicating worse cognitive function.
Demographic and clinical characteristics
Socio-demographic characteristics, smoking status, and use of alcohol in glasses per week were assessed (at the age of 85) during a face-to-face interview. Level of education was specified in eight categories ranging from no education to an obtained university degree. As a measure of income, it was registered whether an individual received state pension only or had additional pension or income. All other parameters were obtained at the age of 86. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of length in meters (kg/m2). Blood pressure was measured twice in seated position with a mercury sphygmomanometer during home visits. The average of the two measurements was used in the analyses. Serum creatinine (μmol/L) and total cholesterol (mmol/L) were measured.
Information on the participant’s medical history was obtained from their general practitioner (GP) or, in case of institutionalization, from their treating physician. Information on the use of medication was obtained from pharmacist records or, in case of institutionalization, from questionnaires filled out by the treating physician. A history of angina pectoris or heart failure was obtained from the GP or treating physician. A history of myocardial infarction was established when it was either reported by the GP or treating physician, or recorded as such on electrocardiograms (ECG) at the age of 85 or 86 using automated Minnesota coding (Code 1-1 or 1-2 excluding 1-2-8). The presence of atrial fibrillation was determined using the ECG at age 86 (Minnesota Code 8-3-1). The ECGs were recorded on a Siemens Sicard 440 (Erlangen, Germany) and were transmitted to the ECG Core Laboratory in Glasgow Royal Infirmary.
A history of overt cardiac disease was defined as having either a history of myocardial infarction, angina pectoris, atrial fibrillation on ECG, or heart failure.
Statistical analysis
Data are presented as number (percentage), mean (±standard deviation, SD) or median (interquartile range, IQR) when appropriate. Demographic and clinical characteristics were compared between groups of lower, middle and higher levels of hs-cTnT according to gender-specific tertiles. Gender-specific tertiles were used because levels of hs-cTnT are gender-dependent [7]. p-values for linear trend were calculated with Pearson’s Chi-square tests for categorical variables and analysis of variance (ANOVA) for normally distributed continuous variables. To test differences between the highest and lowest tertiles of hs-cTnT, ANOVA was used.
The distribution of hs-cTnT was skewed to the right and natural log-transformed (ln) hs-cTnT levels were used in the analyses. Linear regression analyses were used to calculate beta coefficients (β) per unit increase in ln-hs-cTnT with 95% confidence interval (CI) and p-values for the cross-sectional association between hs-cTnT on the one hand and MMSE on the other hand. The annual change in cognitive function for each participant was determined by calculating the beta (β) for the change in MMSE per individual per year, thus making optimal use of all available data during follow-up. Linear regression analyses were used to assess the longitudinal association between hs-cTnT and the annual change in MMSE.
First, a crude analysis was performed (model 1). In model 2, we adjusted for gender, level of education, and serum creatinine levels as these factors could confound the association between hs-cTnT and cognitive function. To assess whether the associations between hs-cTnT and measures of cognitive function were independent of sociodemographic and cardiovascular risk factors, in model 3 we additionally adjusted for income, alcohol use in glasses per week, history of smoking, history of diabetes, history of hypertension, systolic and diastolic blood pressure, BMI, total cholesterol levels, the use of antihypertensive medication, use of statins, and the use of vitamin K antagonists. All longitudinal analyses were adjusted for the baseline MMSE scores.
To assess whether the association between hs-cTnT and cognitive function depended on the presence of a history of overt cardiac diseases, we repeated the cross sectional and longitudinal analyses of model 3 in a series of restricted samples. First, we excluded participants with a history of myocardial infarction, then those with a history of angina pectoris, then those with atrial fibrillation, and then those with a history of heart failure, allowing us to assess the effect of each of these individual cardiac diseases. As a next step, we excluded all participants with any history of the aforementioned cardiac diseases to assess whether higher levels of hs-cTnT associated with cognitive function in participants free from any history of overt cardiac disease. Additionally, we excluded participants with a history of stroke at baseline.
All analyses were performed using SPSS statistical software (SPSS for Windows, version 20, SPSS Inc., Chicago, IL) and figures were made in GraphPad Prism 6 (GraphPad Software, Inc., La Jolla, CA).
RESULTS
Demographic and clinical characteristics
In the entire study population, the median level of hs-cTnT was 14.0 ng/L (10.0-22.0). Table 1 shows the characteristics of the study participants in three groups of hs-cTnT. Participants in the highest tertile (n = 164) had a lower level of education, and more often had a history of cardiovascular disease and diabetes than those in the middle (n = 166) and lowest tertile (n = 125). Diastolic blood pressure and total serum cholesterol were lower in participants in the highest tertile of hs-cTnT, while serum creatinine levels were higher.
Comparison of participant characteristics in gender-specific tertiles of hs-cTnT at the age of 86 (n = 455)
Data are presented as number with percentage or as mean with standard deviation. Ranges of tertiles men: lowest ≤14 ng/L, middle 15–23 ng/L, highest ≥24 ng/L. Women: lowest ≤10 ng/L, middle 11–18 ng/L, highest ≥19 ng/L. ap-value for linear trend; bn = 4 missings for income; cn = 1 missings for myocardial infarction; dn = 4 missings for angina pectoris; en = 4 missings for atrial fibrillation; fn = 1 missings for history of heart failure; gn = 2 missings for stroke. hs-cTnT, high sensitivity cardiac troponin T.
Hs-cTnT and cognitive function at baseline and during follow-up
Figure 1 graphically shows the mean unadjusted MMSE scores in tertiles of hs-cTnT from the age of 86 to 90. At baseline, participants in the highest tertile of hs-cTnT had a 2.0-point lower MMSE score than participants in the lowest tertile (95% CI 0.73 to 3.3, p = 0.002).
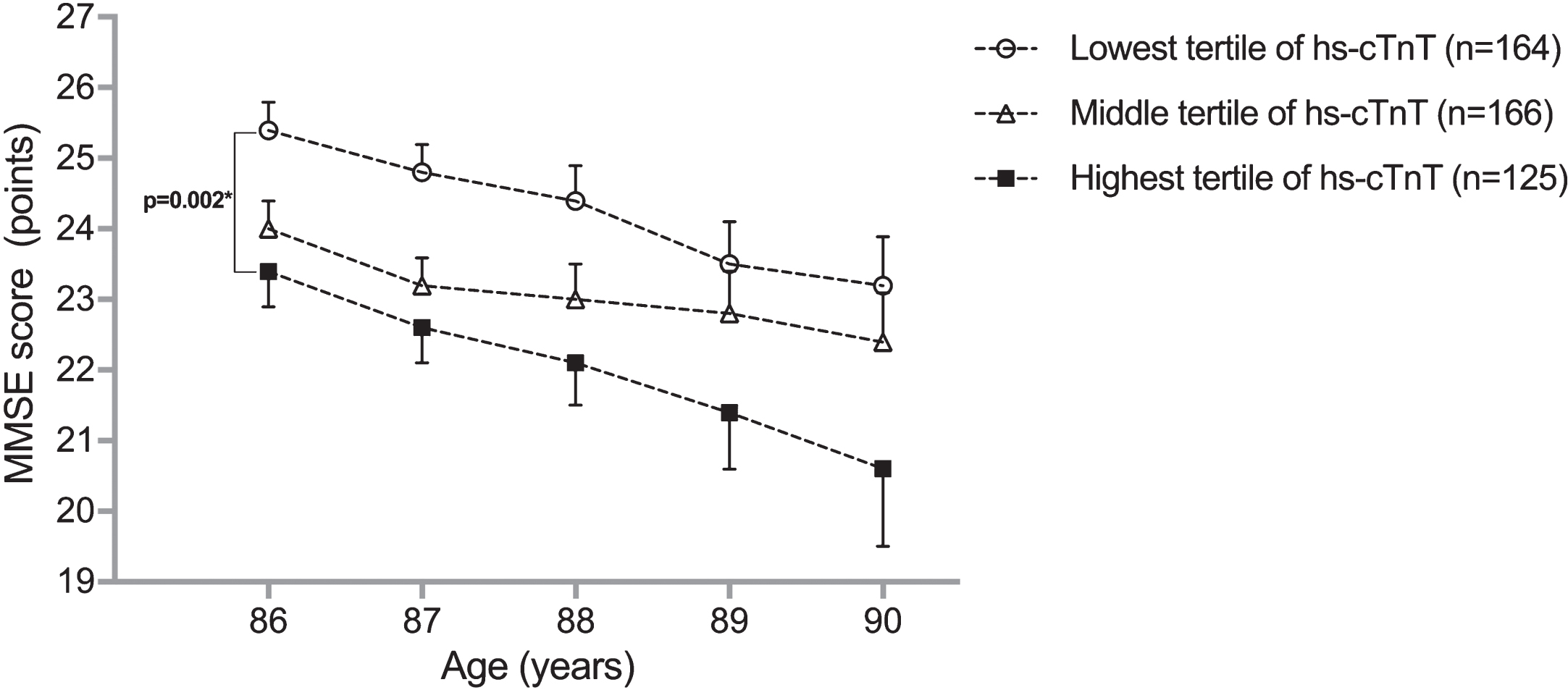
MMSE score from age 86 to 90 years in gender-specific tertiles of hs-cTnT. Data points represent unadjusted means with standard errors. *p-value for mean difference between lowest and highest tertile at baseline (mean difference 1.1 point). Numbers in lowest tertile: age 86, n = 164; age 87, n = 153; age 88, n = 139; age 89, n = 126; age 90, n = 113. Numbers in middle tertile: age 86, n = 166; age 87, n = 153; age 88, n = 144; age 89, n = 127; age 90, n = 111. Numbers in highest tertile: age 86, n = 125; age 87, n = 102; age 88, n = 81; age 89, n = 59; age 90, n = 43. MMSE, Mini-Mental State Examination; hs-cTnT, high sensitivity cardiac troponin T.
Table 2 shows the different models for the cross-sectional and longitudinal relation between hs-cTnT and MMSE score. During follow-up, participants in the highest tertile of hs-cTnT had a 0.58-point steeper annual decline in MMSE compared to participants in the lowest tertile (95% CI 0.06 to 1.1, p = 0.03). The estimates for the relation between higher levels of hs-cTnT and both lower baseline MMSE score and a steeper annual decline on the MMSE remained similar in model 2 and model 3. Participants in the highest tertile were more likely to have less follow-up measurements (Supplementary Table 1).
Cross-sectional and longitudinal relation between hs-cTnT and (change in) MMSE scores
Numbers in the three gender-specific tertiles represent mean scores and mean annual change with SE. aβ, SE, 95% CI, and p-value calculated with linear regression with log-transformed hs-cTnT levels as the continuous determinant and the (annual change in) MMSE score as continuous outcome measures. All longitudinal analyses were adjusted for baseline MMSE scores. Model 1: crude. Model 2: adjusted for gender, level of education in eight sub groups, and serum creatinine. Model 3: adjusted for gender, level of education in eight sub groups, income, alcohol use in glasses/week, serum creatinine, former smoking status, body mass index, total cholesterol, systolic blood pressure, diastolic blood pressure, history of hypertension and history of diabetes, use of antihypertensive medication, use of statins, and use of vitamin K antagonists. hs-cTnT, high sensitivity cardiac troponin T; MMSE, Mini-Mental State Examination β, beta; SE, standard error; CI, confidence interval.
Association between hs-cTnT and cognitive function in participants without a history of overt cardiac disease
Figure 2 shows the results from the analyses restricted to those participants without a history of myocardial infarction, angina pectoris, atrial fibrillation, and heart failure. Estimates for the relation between hs-cTnT and MMSE remained similar for both the cross sectional and the longitudinal analyses, also when all 253 participants with any of the mentioned cardiac diseases were excluded.
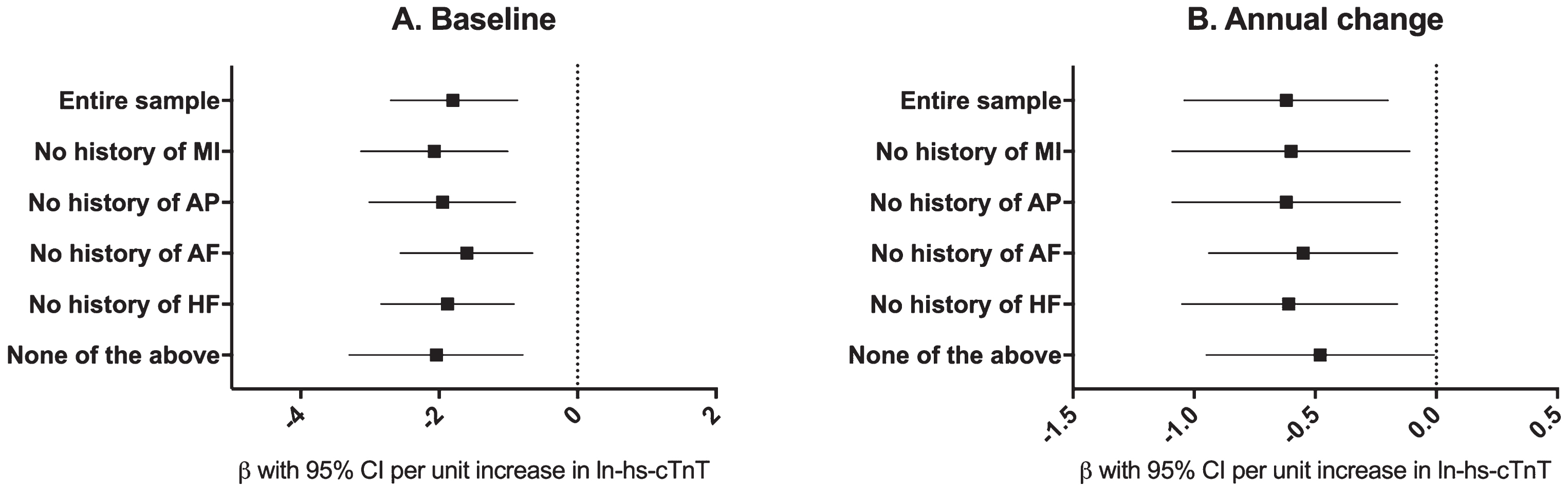
Cross sectional (A) and longitudinal (B) relation between hs-cTnT and MMSE score according to history of cardiac disease. β with 95% CIs were calculated with linear regression with log-transformed hs-cTnT levels as the continuous determinant and MMSE score as a continuous outcome variable. All analyses were adjusted for gender, level of education in eight sub groups, income, alcohol use in glasses/week, serum creatinine, former smoking status, body mass index, total cholesterol, systolic blood pressure, diastolic blood pressure, history of hypertension and history of diabetes, use of antihypertensive medication, use of statins, and use of vitamin K antagonists (model 3). β, beta, 95% CI, 95% confidence interval; (ln)-hs-cTnT, (log-transformed) high sensitivity cardiac troponin T; MMSE, Mini-Mental State Examination. Numbers in the different groups: entire sample: n = 455, no history of myocardial infarction (MI): n = 377, no history of angina pectoris (AP): n = 362, no history of atrial fibrillation (AF): n = 396, no history of heart failure (HF): n = 389. None of the above: n = 253.
Additional sensitivity analyses excluding those with a history of stroke at baseline showed similar results as in the entire sample (data not shown).
DISCUSSION
In a population-based sample of the oldest old, people with higher levels of hs-cTnT had worse cognitive function at baseline and a faster annual cognitive decline during 4-years follow-up, independently of cardiovascular risk factors and a history of overt cardiac disease. As expected in this age group, those with the highest hs-cTnT levels were more likely to have fewer follow-up MMSE measurements, due to mortality [19]. Despite this, a greater cognitive decline was observed in this group. This might suggest an underestimation of the reported association, since cognitive decline is associated with increased mortality, even in the absence of dementia [20].
To date, few studies have investigated the relation between hs-cTnT and cognitive function, and, to the best of our knowledge, ours is the first to do so in the oldest old. Our findings are in line with results from the Atherosclerosis Risk In Communities (ARIC) study, demonstrating that higher levels of hs-cTnT were associated with worse baseline cognitive function and incident dementia, in community-dwelling participants aged around 65, without coronary artery disease, heart failure, or stroke [21]. Additionally, a recent study among older persons (mean age 75 years) with a high burden of vascular diseases (coronary, cerebral or peripheral) or risk factors, found higher levels of hs-cTnT to be associated with worse cognitive function and steeper cognitive decline [22]. In contrast, another study among memory clinic patients aged around 70, reported that only in patients with cerebrovascular disease, higher levels of hs-cTnT were related to cognitive impairment and dementia [23] which suggests a role particularly for vascular brain pathologies in the relation between hs-cTnT and cognitive function. In light of other findings in the literature, our study adds that the relation between higher levels of hs-cTnT and worse cognitive function is also found in the oldest old, independently of the presence of cardiovascular risk factors and a history of overt cardiac disease. It is an important finding that the direction of the effect is the same as in younger populations, since several other conventional (cardiovascular) risk factors and markers such as blood pressure [24] and serum cholesterol [25, 26], show inverse predictive associations in the oldest old people. This might suggest that the mechanisms involved in the relation between hs-cTnT and cognitive decline are not changing over age.
Several explanations can be given for the finding of an association between higher levels of hs-cTnT and worse cognitive function. First, cardiovascular risk factors, impaired kidney function, and cardiac diseases may lead to both higher levels of hs-cTnT and worse cognitive function. To address this, we adjusted our analyses for cardiovascular risk factors and kidney function, which did not change our results. Moreover, even when we excluded those participants with a history of overt cardiac disease, higher levels of hs-cTnT were still associated with worse cognitive function. Second, not only clinically overt but also microvascular coronary artery disease may cause elevated levels of hs-cTnT [8]. A study comparing non-ischemic heart failure patients with non-heart failure patients, demonstrated that the presence of coronary microvascular dysfunction was associated with an increased release of cTnT from the myocardium [27]. Since it has been shown that even subclinically reduced cardiac function is related to worse cognitive function [28], this may underlie our findings of an association of higher hs-cTnT and worse cognitive function. Third, the independent association between higher levels of hs-cTnT and worse cognitive function could also imply that higher levels of hs-cTnT not only indicate microvascular coronary disease, but rather reflect a global microvascular disease including cerebral small vessel disease. Indeed, higher levels of hs-cTnT have not only been linked to overt adverse brain outcomes such as stroke [11, 12], but also to subclinical vascular brain abnormalities [29], which in turn predispose individuals to an increased risk of accelerated cognitive decline [15, 30]. In the current study, results remained similar after exclusion of participants with a history of myocardial infarction as well as stroke, which may suggest a role for subclinical vascular damage in the association between higher levels of hs-cTnT and worse cognitive function. Our findings support the notion that cardiac function (and cardiac biomarkers) are of importance for brain aging and cognitive decline [31–33]. Hs-cTnT may be a marker of microvascular coronary artery disease or global microvascular disease underlying processes of cognitive deterioration in older people. Future studies may provide insight into the role of (micro) vascular brain pathologies in the association between hs-cTnT and cognitive function. Besides mechanistic insights, combined with the findings in younger study populations, these results warrant future studies to investigate the added value of hs-cTnT to predict cognitive decline and potentially dementia [34, 35].
Strengths of our study include the well-defined population-based sample of the oldest old, the annually repeated cognitive assessment and availability of detailed clinical information to evaluate the potential role of overt cardiac diseases. However, when interpreting these results, certain limitations of our study must be taken into account. First, in the Leiden 85-plus Study, no echocardiographies were performed at the baseline for this study. We therefore did not have a direct measure of cardiac function available, such as left ventricular ejection fraction or cardiac output, and had to approximate this using cardiac diseases. Additionally, neuroimaging data is not available to investigate the potential role of subclinical cerebrovascular damage in the relation between hs-cTnT and cognitive decline. Furthermore, because of the observational design and despite adjustments for sociodemographic and clinical characteristics as well as cardiovascular risk factors, there might still be residual confounding. Last, the MMSE is a broad measure of global cognitive function and does not cover all cognitive domains, nor does it ascertain the presence of dementia.
In conclusion, in a population-based sample of the oldest old, people with higher levels of hs-cTnT had worse cognitive function and a faster decline in cognitive function over time, independently of cardiovascular risk factors and a history of overt cardiac disease.