
Abstract
Background:
Working memory (WM) problems are commonly observed in Alzheimer’s disease (AD), but the affected mechanisms leading to impaired WM are still insufficiently understood. The ability to efficiently process serial order in WM has been demonstrated to be fundamental to fluent daily life functioning. The decreased capability to mentally process serial position in WM has been put forward as the underlying explanation for generally compromised WM performance.
Objective:
Determine which mechanisms, such as order processing, are responsible for deficient WM functioning in AD.
Method:
A group of AD patients (n = 32) and their partners (n = 25), assigned to the control group, were submitted to an extensive battery of neuropsychological and experimental tasks, assessing general cognitive state and functioning of several aspects related to serial order WM.
Results:
The results revealed an impaired ability to bind item information to serial position within WM in AD patients compared to controls. It was additionally observed that AD patients experienced specific difficulties with directing spatial attention when searching for item information stored in WM.
Conclusion:
The processing of serial order and the allocation of attentional resources are both disrupted, explaining the generally reduced WM functioning in AD patients. Further studies should now clarify whether this observation could explain disease-related problems for other cognitive functions such as verbal expression, auditory comprehension, or planning.
INTRODUCTION
Alzheimer’s disease (AD) is typically characterized by cognitive impairments, and in particular memory deficits. Difficulties with episodic memory appear to be the most profound, but memory impairments also include compromised functioning of working memory (WM) and/or semantic memory [1–8]. Current treatments are limited to the deceleration of this degenerative disease to improve the quality of life of patients and their family. This requires early diagnosis and goal-directed treatment strategies, such as cognitive training (for a review, see [9]). To make progress in the development of these methods, it is crucial to understand the mechanisms underlying the dysfunction, not only episodic memory, but also for WM.
One possible mechanism for a deficient WM in AD is that WM problems are related to the dysfunctional employment of executive control, steered by the central executive [1–3]. According to the classic model of Baddeley and Hitch [9], WM can be dissociated into three components; the central executive and two slave-systems that serve to temporarily store domain-specific information (the phonological loop and the visuospatial sketchpad). The central executive serves as the attentional control center and is thought to be responsible for the allocation of attentional resources to the phonological loop and the visuospatial sketchpad, and thus plays a crucial role in the division of labor between tasks [1, 2]. Evidence for a central executive dysfunction in AD can first be observed in the performance of patients, where the attentional resources have to be divided between two demanding and simultaneous tasks. In comparison to a single-task setting, AD patients typically experience serious problems performing dual tasks, independent of task difficulty [1, 2]. Such disadvantage for dual-task settings is significantly less pronounced in the healthy elderly [1, 2]. Second, AD patients generally perform worse on a variety of executive tasks (e.g., verbal fluency test, Wisconsin Card Sorting Test, the Modified Card Sorting Test, delayed alternation, trail making test) compared to controls, where the tasks are often related to the functioning of the central executive component [3, 10]. Based on these observations, the central executive is thought to be the component of the WM system that is compromised in AD. However, this explanation has difficulty reconciling the fact that central executive functions are supported by frontal brain areas, while degenerative processes in the early-AD brain are typically observed within the temproroparietal regions, which are located towards the posterior of the brain (e.g., [7, 12–15]).
Moreover, an executive function account is not easily reconciled with the fact that WM deficits have also been reported in studies that focus on WM capacity as the critical reason for WM impairments in AD [7, 16]. For example, Stopford et al. [7] compared patients suffering from frontotemporal dementia with AD patients in their performance on attentional, executive, and WM tasks, both patient groups expressed a different pattern of impaired performance across the variety of tasks. Patients suffering from frontotemporal dementia expressed clear difficulties on the attentional and executive tasks. In contrast, AD patients performed worse on the WM tasks and expressed specific difficulties with short-term memory, as reflected in quick information overload and difficulty holding information in WM. Based on these observations, it has been argued that WM problems in AD can be assessed in terms of a reduced WM capacity [7, 16].
In sum, two different accounts have been put forward to approach WM impairments in patients with AD. On the one hand, AD patients are thought to suffer from impaired executive functioning, hindering the central executive to efficiently distribute targeted attentional resources within WM [1–3]. On the other hand, empirical findings also support the simple notion of a reduced WM capacity, where this inability to keep a sufficient amount of information online in WM has a negative impact on the patients’ daily functioning [7, 16]. Currently, there is no consensus as to which mechanisms are responsible for the unsuccessful employment of WM in AD. However, in the next section we will propose and substantiate the idea that the ability to order information in WM might be the crucial component that could reconcile the seemingly opposing ideas of a malfunctioning central executive or the reduced WM capacity underlying WM problems in AD.
Importantly, almost anything we do in daily life requires the temporary (in WM) or permanent (in long-term memory) storage of serial information, if only to memorize a grocery list, to perform a daily routine, to cook a recipe, to learn a new skill, or to formulate sentences. The functioning of the central executive encompasses many attentional tasks, such as task switching, updating the WM content, inhibition of task-irrelevant information, strategy selection, etc. Importantly, all of these tasks at least partially rely on the processing of serial order [17–21]. Furthermore, WM capacity is generally measured and evaluated by tasks that inherently contain a serial order component; e.g., forward and backward digit span tasks and complex span tasks [22–24]. The performance of the participant is evaluated based on the successful serially ordered recall of the items. When the participant recalls the correct items, but in an incorrect order, it is generally concluded that the number of to-be-memorized items may have exceeded WM capacity [22, 23]. While WM capacity has been demonstrated to correlate with other WM measures in evaluating the construction, maintenance, and updating of memory traces [24], only span tasks have previously been used to compute the size of WM capacity. In other words, the methods used to assess WM capacity and central executive functioning contain a serial order component. Therefore, the question rises whether the impaired use and processing of serial order could be the main underlying affected mechanism leading to impaired WM functioning in AD, rather than an impaired functioning of either the central executive or a reduced WM capacity.
When attempting to understand impaired WM functioning in AD, little research has been done that attempted to combine the two seemingly diverging perspectives on WM problems. Lamar and Price [25] are one of the few that reported order-specific WM problems by implementing an extended version of a backward digit span task, requiring ordered item recall. They reported that the order-specific recall performances in AD patients negatively correlated with the global degree of white matter hyperintensities observed in the brain, while such correlation with white matter alterations was not observed for the AD patients’ performance when recalling digits in any order. The difference between behavioral performances on serial order recall versus unordered item recall in AD emphasized that AD patients experienced more trouble with the ordered storage of item information compared to a non-ordered global memorization of the item itself. This discrepancy between the memory for item identity and memory for order information was the first important step toward the identification of the exact mechanism that underlies WM dysfunction. More specifically, previous studies have already highlighted the dissociation between memory for order and item information (for a review, see [26–28]; for imaging studies, see [29–32]). Therefore, in order to conclude that order processing in AD is affected, it is crucial to ascertain that poor performance is the direct behavioral manifest of impaired order processing, and not of a generally compromised memory trace.
In sum, previous studies suggest that WM problems in AD are generally a result of impaired functioning of the central executive [1–3] or of a reduced WM capacity [7, 16]. In the current study, we propose that the processing of serial order might be the main underlying problem causing WM malfunctioning. Only one study has thus far suggested a disadvantage for the memory of item order compared to a relative intact memory for unordered item identity [25]. Therefore, in the current study, we investigated the specificity of impairments observed in verbal and visuospatial serial WM, by administering an extensive battery consisting of a variety of WM tests on AD patients and their partners. We hypothesized that when comparing AD patients to their (non-AD) partners, the processing of order will be more strongly affected than the memory trace for identity. Furthermore, the findings of the various conducted tasks should clarify whether the central executive and/or reduced WM capacity can separately account for WM problems in AD— or whether the affected processing of order could explain both accounts. Three types of digit span tasks were executed, requiring forward or backward recall of item sequences. It was expected that the control group would outperform AD patients on these tasks. However, in order to answer our research question concerning impaired order processing in AD, a more fine-grained order measure had to be derived from the performances on the span tasks. This order measure was designed to mainly reflect the participants’ ability to efficiently process order while filtering out any effects due to generally worse performances. This order measure was then addressed to test the following hypothesis: if, in line with past literature reports [7, 16], a reduced WM capacity and not impaired order processing would be the main problem underlying difficulties in recalling memorized items in patients, we would expect AD patients and the control group to perform equally well on the order measure. However, if patients experience specific problems with the mental processing of order within WM, the loss of order representations will be more pronounced in AD patients compared to the control group. Consequently, we would expect the order processing deficit to impair WM span more in the backward than in the forward digit span task. More specifically, the forward digit span task simply relies on the representation and recall of items by means of inter-item associations. The backward digit span task requires the manipulation and reorganization of a mental visuospatial representation of the items and thus relies more strongly on efficient order processes [33].
Furthermore, efficient order processing does not only require the mere ordered recall of all memorized information, but also the localization of specific information stored within WM. The verbal WM position task required participant to recall position-specific item information. In the context of an expected order deficit in AD patients, we expected them to demonstrate greater difficulties with localizing item information within WM, compared to the control group. Additionally, in order to assess the comparability between the mechanisms driving errors made by AD patients and the control group, detailed error coding was performed on in the verbal WM task and the digit span tasks and submitted to exploratory analyses.
Standardized tests were implemented to assess the comparability between the AD patients and the control group (their partners). AD patients were hypothesized to perform worse on measures evaluating general cognitive functioning (a standardized measure that is typically used to assess AD severity) and a simple math task (containing a minor component of order processing). We also included a task to assess generalized frontal cognitive functioning and pre-morbid intelligence.
Data collection
The study was approved by the ethical committee of the Faculty of Psychology and Educational Sciences at Ghent University and was in agreement with the Declaration of Helsinki. All participating patients were recruited from the memory consultation of University Hospital of Ghent. Patients were selected by clinical diagnosis. The diagnosis was made on the basis of a combination of results from the following measures: performance on the Mini-Mental State Examination test, neurological examination, detailed neuropsychological testing, MRI of the brain displaying temporal atrophy, and biomarker analysis of the cerebrospinal fluid (presence of beta amyloid and tau protein). Table 1 displays which measures were obtained for each patient contributing to the diagnosis of AD.
All the types of information collected for each AD patient that contributed to the diagnosis of Alzheimer’s disease. The reported score on the Mini Mental State Examination reflects the score of the AD patient achieving during the most recent visit of the patient to the hospital prior to research participation. ‘X’s mark the availability of information provided by detailed neuropsychological assessment, known familial history in AD disease and/or the execution of biomarker analysis on cerebrospinal fluid. AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; CSF, cerebrospinal fluid; CT, computerized tomography; MR, magnetic resonance; PET, positron emission tomography; SPECT, Single-photon emission computed tomography
The control group was composed of partners of AD patients who were willing to participate. Control participants had no history of severe psychiatric conditions and never suffered from any neurological condition, cardiovascular problems, or diabetes. However, note that the final control group cannot be considered to be a ‘normal healthy aging’ group as partners of AD patients are known to be at risk for depression or anxiety disorders [34, 35].
All participants provided written consent prior to participation.
The data of 32 AD patients (average age 74.35 years, SD = 9.85; 21 females) were collected. Of these patients, 25 of their partners were additionally tested as control participants (average age = 72.50, SD = 9.22; 13 females; see Table 2 for analysis on demographics). All participants were tested at home at a table. The administration of the full test battery took 60 to 95 mins. In order to avoid the participant exhaustion and information overload, the full battery was administered during two separate home visits and if necessary, additional pauses in between the tests were implemented. Incomplete data collection occurred for the majority of the patients for various reasons like task complexity, fear of computerized tasks, time constraints, no re-test possibility, and condition of the patient during the testing.
Data displaying the demographic variables for the AD patients and control group. Results of paired t-tests are reported, indicating the absence of any group differences on following variables; average age at testing, proportion of female/male participants in each group, the average each of leaving school
METHODS
Neuropsychological tests
Several standardized neuropsychological tests were used to assess the level of functionality of specific psychological functions. Overall cognitive performance, the integrity of frontal lobe functionality, pre-morbid intelligence, and math ability were tested. The collected data were analyses in order to reveal the extent to AD patients’ performances differed from the controls.
Montreal Cognitive Assessment (MoCA)
A brief cognitive screening test evaluating the general cognitive status and severity of cognitive decline [36].
Frontal Assessment Battery (FAB)
A short screening test to assess frontal dysfunction and serve as differential diagnosis of frontotemporal dementia. The test consists of six subtests that measure different aspects of frontal lobe functions. These subtests cover conceptualization, fluency, sequential movements, opposing movements, a go/no-go paradigm, and utilization [37].
The Dutch Reading Test for Adults (or Nederlandse Leestest voor Volwassenen; NLV)
This test consists of a 50-item list of Dutch words that are derived from foreign languages (English and French). The participant’s pronunciation of the words is scored and used as a measure of pre-morbid intelligence level. This task is often used to assess pre-morbid intelligence as it has been shown to highly correlate with verbal intelligence and has demonstrated to be relatively insensitive to cerebral damage [38].
Math task
A simple paper and pencil test consisting of 32 items; 8 summations, 8 subtractions, 8 divisions, and 8 multiplications, each printed in a separate column, with an integer as the outcome. This brief test was used to assess remaining math ability in patients and order processing for a simply daily task.
Experimental tasks
A variety of experimental tasks were designed with the aim of evaluating various aspects of WM functioning and serial order coding in the participants. Along with the experimental tasks (described below), participants also performed a magnitude task [38; ca. 10 min], a number interval bisection task [39, ca. 7–10 min] and a line bisection task [40, ca. 2-3 min]. These data were collected with respect to a different research question and therefore will not be further discussed within this paper.
Long forward digit span
WM was assessed using a long forward digit task. Compared to the standardized digit span task, requiring the completion of 3 trials per span length, the current task consisted of five more trials for each span length and did not employ a discontinuation rule, hence the ‘long’ digit span task. The experimenter read out a series of numbers at a rate of 1 digit per second. The participant was instructed to immediately verbally recall the numbers in correct order. The task was constructed in such a way that 8 trials of 3-, 4-, 5-, and 6-digit span lengths had to be performed, for a total of 32 trials. All 4- and 5-span trials were constructed according to a selection procedure proposed by Lamar et al. [25].
The following dependent variables were collected for this task: Accuracy score for serial order –This score reflected the amount of correctly recalled numbers in their correct serial position, divided by the total possible recalled digits for each span length (e.g., from the original sequence “5942” the participant recalled “52”. Only one item is recalled in the correct position, i.e., “5”, the accuracy score for this sequence is thus 1 divided by 4, the original sequence length, i.e., 25%). These accuracy scores were calculated separately for each span length. Accuracy score for any order –This score reflected the amount of correctly recalled numbers of the sequence, independent of the correct recall position, divided by the total possible recalled digits for each span length. (e.g., in line with the previous example; if the participant recalled “52”, he now received an accuracy score of (2/4)×100 = 50% on the any order measure). These accuracy scores were calculated separately for each span length. The order ratio - This order measure was used to measure to what extent memory for order was lost compared to the general (non-ordered) memory trace. The order ratio simply consisted of the ratio serial order/any order. Crucially, this order measure preserved the difference between the two measures, i.e., the processing of order, but filtered out other effects, e.g., resulting from overall bad performance. For example, patient scoring 20% on the serial order measure and 25% on the any order measure would achieve the same order ratio as a control participant achieving 80% on serial order and 100% on any order (20/25 = 80/100), despite the fact that the overall accuracy is much lower in the patient compared to the control Working memory capacity – WM capacity was determined by evaluating accuracy scores on the serial order measure; selection of the largest span length with a > 80% accuracy score. On average this meant that the participant was allowed to incorrectly recall more than 1 but less than 2 out of the eight trials. As the task was quite demanding in terms of sustained attention, implementing this small buffer allowed for mistakes arising due to fatigue. Error types – Similar to the analyses performed by Lamar and Price [25], four types of errors were calculated; capture errors, transposition errors, perseverations, and intrusion errors. Capture errors reflected the sum of two types of errors; ‘within trial capture errors’ and ‘between trial capture errors’. ‘Within trial capture errors’ were recorded on 4-, 5-, and 6-digit span trials when participants grouped numbers to create a contiguous series of numbers e.g., ‘361729’ – recall of ‘6
Transposition errors occurred when the participant misplaced a recalled number in the sequence, without creating a contiguous series of numbers, e.g., ‘8492’ – recall of ‘8294’. Perseveration errors were made when the participant recalled a specific number more than once during a single trial, e.g., ‘482’ – recall of ‘484’.
Intrusion errors were made when the participant reported a digit that was not part of the current trial or the previous trial.
Long backward digit span
This task was designed and administered in the same fashion as the forward digit span. Participants were now instructed to recall the verbally presented sequences in a backward order. The backward digit span task consisted of different sequences from the forward digit span task. The same five measures were collected as in the forward digit span task, but now assessing the correct backward ordered recall.
Corsi block task
The Corsi block task assessed visuospatial WM. This task is very similar to the forward digit span task, but now participants had to recall the position of visuospatially presented blocks on a screen.
The task was administered on a 12” touch-screen of a convertible Acer laptop. The screen was put in a position of thirty degrees relative to the table. Nine grey 2×2 cm squares were presented against a white background at fixed positions. At a 1 square/s rate one of these squares lit up in black. After 1 s, this square turned back to grey, with the next square turning black. Participants were instructed to memorize the correct order in which these squares turned black. After the presentation of the last black square, all squares turned back to grey and two black lines were displayed on the left and right side of the screen. The two black lines indicated that the participant could initiate full recall. At this point the participant was asked to indicate the correct order in which the grey blocks had turned black, by pressing with their finger on the correct squares. The experimenter manually initiated the next trial when the participant indicated they were ready. Series of 3 trials consisting of 3-, 4-, 5-, and 6-digit span lengths had to be performed. Block positions could not be repeated within a single sequence. Every participant had to complete all twelve trials. A short practice phase was implemented before the start of the actual experiment, presenting an example of a single trial of a 3-block span length.
For this task, the same measures were calculated as for the forward span task, except for the evaluation of error scores. Moreover, scores were now calculated for three trials per span length (instead of eight).
Verbal working memory position task
This WM task assessed position-specific problems located in WM representations and was based on the paradigm described by van Dijck and colleagues [41]. A full trial proceeded as follows: the experimenter read out a series of letters, which had to be memorized in correct order by the participant. Finishing the sequence, the experimenter queried the participant’s memory for a specific position by posing a question in following format: “What was the second letter?”. The verbal response of the participants was then recorded by the experimenter before reading the next to-be-memorized letter sequence.
Before the start of the experimental trials, the number of letters to-be-memorized by the participant was determined by a preceding practice phase using a step-by-step selection procedure. At the beginning of the practice phase, three trials of three letters had to be completed by the participant. If the participant made no errors on any of these trials, the next sequence length was assessed by means of three trials (i.e., 4 letters to-be-memorized). The sequence increased in length until the participant reached a sequence length where he made one or two errors out of the three trials. Only if the participant made an error during the first or second trial of the three-letter trial, a practice phase for two-digit length trials was initiated. If one or two errors were made on the three trials of the two-letter sequences, this digit span length was selected for the experimental task. If the participant responded correctly to all three test items of the two-letter sequences, the participant’s understanding of the task was reassessed and the three trials of the three-digit length were repeated.
During the experimental task, all positions of the letter sequences were queried equally often. All positions were tested 8 times for the 2-, 3-, 4- and 5-digit length sequences (i.e., resulting in a total of 16, 24, 32, and 40 trials for each digit span length, respectively). If a participant was assigned to perform the task on a 6-digit sequence length, each position was queried 7 times, in case of a 7-digit sequence length only 6 times. This latter adjustment was necessary to limit the duration of the task and effects of exhaustion.
The following dependent variables were collected for the verbal WM position task: Accuracy scores – For each participant the percentage of correctly completed trials was calculated. Data for this simple measure were collected to assure that performances of AD patients equaled performances of the control group, showing that the appropriate sequence length was selected for each participant. Error types – Three types of errors were evaluated; distance errors, intrusion errors, and no-response errors. Of all incorrectly completed trials the percentage of occurrence of each type of error was calculated. Responses were categorized to be a ‘distance error’ if the participant recalled a letter that was part of the memorized sequence, but which was not the correct answer. Intrusion errors reflected the recall of a letter by the participant that was not part of the memorized sequence. If the participant did not provide a response to a specific trial, this trial was categorized as a ‘no-response’ error. Note that distance errors reflect mistakes made to the recall of serial order. Performance patterns related to this type of error were further investigated by means of ‘distance scores’. Distance scores – Distance scores were computed by calculating the distance from the recalled letter to the position of the correct letter. If the recalled number was positioned before the correct position, negative distances were counted; if the recalled letter was located further in the sequence than the correct position, positive distances were counted. Because each digit span length allowed for different possible deviation distances from the correct answer, the actual number of positions between the recalled position and correct answer was then divided by the maximum distance length for that particular digit span length. For example, if the participant was asked to recall the fourth letter of the presented series “BCDFG”, but answered with “C”, the distance of C from the correct answer (F) is – 2, which is then divided by 4 (5– 1). The averaged distance score was calculated to investigate whether participants deviated to the beginning or the end of the WM sequence when recalling an incorrect letter. The standard deviation provided an indication of the variability in the distance scores. For all participants, the averaged distance score and the standard deviation were calculated and submitted to a paired t-test, comparing performances between the control group and AD patients.
RESULTS
Neuropsychological tests
For the MoCA test, which assesses general cognitive functioning, AD patients had an average score of 17.07, while their partners scored significantly higher, with an average score of 25.90 (Table 3). The cut-off score for normal cognitive functioning is 26 or higher, while a score of 22 to 25 would indicate mild cognitive impairment [36]. The average score for the control group equaled the cut-off score for healthy functioning, indicating that this group may already be experiencing some cognitive decline. The large difference in MoCA-scores between the two groups validated further comparison of the AD patients to the control group; diagnosed patients clearly exhibited greater cognitive decline compared to the control group.
Data of the neuropsychological tasks, performance scores, statistical results of paired t-tests and sample sizes are reported for AD patients and control participants separately. AD, Alzheimer’s disease; MoCA, Montreal Cognitive Assessment; FAB, Frontal Assessment Battery; NLV, Dutch Reading Test for Adults (Nederlandse Leestest voor Volwassenen)
Scores on the FAB did not differ between both groups, indicating no group differences in terms of frontal (dys)function (Table 3).
Pre-morbid IQ was determined using the NLV task, for which no significant difference was observed between the two groups (Table 3).
Lastly, general remaining math ability was assessed using a simple math task. Patients made significantly more errors than controls (Table 3).
In sum, the MoCA test demonstrated the two groups to be significantly different from each other in terms of cognitive functioning, a crucial indicator for MCI or AD, and in terms of preserved math and order processing in a simple math task. Important for the interpretation of further results, both groups were comparable in terms of frontal functioning and pre-morbid intelligence level.
Long forward digit span
WM capacity and order measures
27 AD patients and 24 controls successfully completed the forward digit span task.
First, between-group differences in the size of the WM capacity were assessed, which showed that on average, the patient group had a WM capacity allowing for the storage of 4.41 (SD = 0.84) elements, while the control group had a WM capacity of 4.79 (SD = 0.78). This difference was not significant [t(23) = 1.75, p = 0.10].
A repeated measures ANOVA was executed to investigate whether the AD patient group made different types of errors compared to the control group. The indicated that AD patients and the control group made the same type of errors [F(3,21) = 0.86, p = 0.11, ηp2 = 0.11]. In proportion to all errors made, transposition errors represented 82.55% (SD = 0.07) of all errors, capture errors were made in 11.37% (SD = 0.10) of the cases, 2.09% (SD = 0.03) were perseveration errors and 3.99% (SD = 0.08) were intrusion errors.
A 4 (span length: 3, 4, 5, or 6) by 2 (AD versus control) mixed ANOVA was conducted for serial order and any order, followed by the same analysis for the order ratio.
For serial order, a main effect of group was observed [F(1,49) = 7.01, p = 0.01, ηp2 = 0.13], indicating an overall worse performance for AD patients (accuracy scores: AD patients = 75.62%, SD = 0.14; controls = 83.61%, SD = 0.08). A main effect of span length was also observed [F(1,49) = 218.94, p < 0.001, ηp2 = 0.82], reflecting decreasing accuracy scores with increasing span length for both groups (accuracy scores for digit spans of 3, 4, 5, or 6 digits respectively; 99.08%, SD = 0.03; 93.75%, SD = 0.12, 72.89%, SD = 0.19; 52.11%, SD = 0.24). The interaction between group and span length was significant [F(1,49) = 4.87, p = 0.03, ηp2 = 0.30], demonstrating that patient performance on the recall of order declined more strongly compared to controls as a function of digit span length (Fig. 1A). Patients’ serial order accuracy scores for span lengths of 3-, 4-, 5-, and 6-digit spans were 98.30% (SD = 0.04), 91.26% (SD = 0.16), 68.32% (SD = 0.21) and 44.81% (SD = 0.25), respectively. For controls the accuracy scores for serial order were the following: 100% (SD = 0.00), 96.29% (SD = 0.05), 77.22% (SD = 0.16), and 60.92% (SD = 0.21).
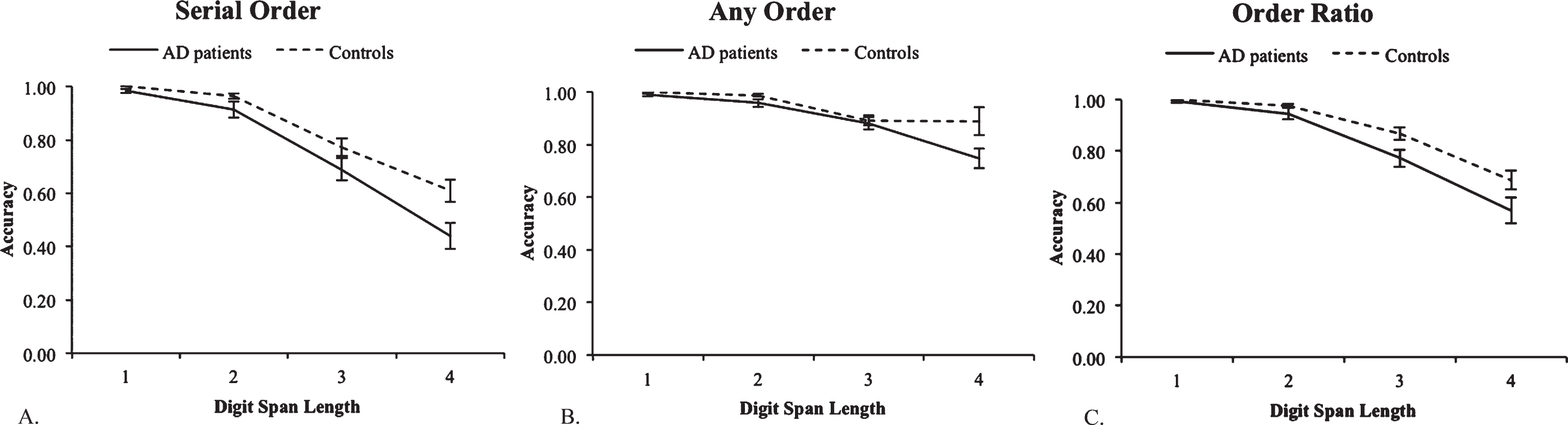
Visualization of accuracy scores on the forward digit span task, depending on the performed digit span length. A) Accuracy scores on the ‘serial order’ measure. B) Accuracy scores on the ‘any order’ measure. C) Scores on the ‘order ratio’, reflecting the accuracy scores for ‘serial order’ divided by ‘any order’.
The analysis of the any order accuracy scores showed a main effect of group [F(1,49) = 4.80, p = 0.03, ηp2 = 0.09] and of digit span [F(1,49) = 93.81, p < 0.001, ηp2 = 0.66]. The more items to be recalled, the worse the performance was on the task. Again, an interaction between group and digit span length was observed [F(1,49) = 6.09, p = 0.02, ηp2 = 0.11, Fig. 1B].
A repeated measures ANOVA on digit span length and between-subjects factor group was performed using the order ratio (accuracy serial order / accuracy any order). The results showed a main effect of group [F(1,49) = 5.411, p = 0.02, ηp2 = 0.10], demonstrating a lower order ratio of 0.82 (SD = 0.23) for patients, compared to the control group with a ratio of 0.88 (SD = 0.17). This main effect indicated that the specific memory for order is worse in AD patients compared to controls. There was also a main effect of digit span length [F(1,49) = 143.06, p < 0.001, ηp2 = 0.75], with scores on the order ratio of 1.00 (SD = 0.02), 0.96 (SD = 0.09), 0.82 (SD = 0.16), and 0.62 (SD = 0.23), for digit span lengths of 3, 4, 5, and 6, respectively. The interaction observed for group and digit span length displayed a trend toward increasing group differences with increasing span length [F(1,49) = 3.36, p = 0.07, ηp2 = 0.06; Fig. 1C].
Long backward digit span
WM capacity and order measures
Of all patients, 29 performed the long backward digit span task, along with 24 controls.
We first assessed differences in the size of the WM capacity between AD patients and the control. On average, the patient group had a WM capacity allowing for the storage of 3.12 (SD = 0.65) elements. The control group had a WM capacity of 3.75 (SD = 0.99), which was significantly different from the patients WM capacity [t(21) = 2.34, p = 0.04].
A repeated measures ANOVA was conducted to investigate whether the AD patient group made different types of errors compared to the control group. The results demonstrated that AD patients and the control group make the same type of errors [F(3,21) = 1.83, p = 0.17, ηp2 = 0.21]. In proportion to all errors made, transposition errors represented 81.90% (SD = 0.08) of all errors, capture errors were made in 9.31% (SD = 0.08) of the trials, 2.74% (SD = 0.05) were perseveration errors and 6.05% (SD = 0.11) were intrusion errors.
The same measures as in the forward digit span task were collected: accuracy on serial order and any order, the order ratio, and WM span. A repeated measures ANOVA for serial order was performed with digit span as a within-subjects factor (4 lengths) and group as between-subjects factor. Analyses revealed a main effect of group [F(1,51) = 10.61, p = 0.002, ηp2 = 0 0.17], with lower accuracy scores for the patient group (accuracy serial order = 52.97%, SD = 0.17), compared to the control group (accuracy serial order = 68.21%, SD = 0.15). Also a main effect of digit span length was observed [F(1,51) = 253.03, p < 0.001, ηp2 = 0.83], with decreasing accuracy scores for increasing digit span lengths of 83.09% (SD = 0.21), 61.82% (SD = 0.25), 48.29% (SD = 0.20) and 42.17% (SD = 0.20), for the span lengths of 3, 4, 5, and 6 digits respectively. No interaction was observed [F(1,51) = 2.67, p = 0.11, ηp2 = 0.05; Fig. 2A].

Visualization of accuracy scores on the backward digit span task, depending on the performed digit span length. A) Accuracy scores on the ‘serial order’ measure. B) Accuracy scores on the ‘any order’ measure. C) Scores on the ‘order ratio’, reflecting the accuracy scores for ‘serial order’ divided by ‘any order’.
Analyses for the any order measure revealed a main effect of group [F(1,51) = 8.53, p = 0.005, ηp2 = 0.14], with an accuracy score on any order of 79.01% (SD = 0.09) and 88.95% (SD = 0.06) for patients and controls, respectively. A main effect of digit span length was also observed [F(1,51) = 80.07, p < 0.001, ηp2 = 0.61], with accuracy scores of 97.38% (SD = 0.05), 87.81% (SD = 0.12), 76.00% (SD = 0.15) and 71.46% (SD = 0.17) for all four digit span lengths respectively. Furthermore, no interaction was observed [F(1,51) = 1.77, p = 0.17, ηp2 = 0.10; Fig. 2B].
The analysis of order ratio revealed a main effect of group [F(1,51) = 8.69, p = 0.005, ηp2 = 0.15], with a ratio of 0.63 (SD = 0.30) for patients, and 0.76 (SD = 0.22) for controls. In accordance to observations made for the forward digit span task, these results indicated a deterioration of order representational memory traces in patients compared to the controls. A main effect of digit span length was also observed [F(1,51) = 107.25, p < 0.001, ηp2 = 0.68], with decreasing order ratios for increasing digit span lengths of 0.85 (SD = 0.19), 0.69 (SD = 0.24), 0.58 (SD = 0.24) and 0.48 (SD = 0.28) for digits spans of 3, 4, 5, and 6, respectively. Also an interaction was observed [F(1,51) = 4.23, p = 0.04, ηp2 = 0.08; Fig. 2C]. Not only were patients worse at processing order than controls, the deterioration of order processing was proportionally much stronger than in controls when WM became increasingly loaded. Patients displayed an order ratio of 0.83 (SD = 0.22), 0.61 (SD = 0.26), 0.55 (SD = 0.25), and 0.49 (SD = 0.30) for span lengths of 3, 4, 5, and 6 digits, respectively. The ratios for the control group were the following: 0.88 (SD = 0.16), 0.79 (SD = 0.18), 0.70 (SD = 0.21), and 0.61 (SD = 0.21).
Corsi block test
This computerized visuospatial WM test was completed by 21 AD patients and 18 controls.
First, visuospatial WM capacity was computed for each subject. As only three trials per digit span size had to be completed, visuospatial WM capacity was assigned to the last digit span size for which a 100% performance was observed on all three trials. The average visuospatial WM span for patients resulted in the average storage of 2.91 (SD = 0.53) spatial items, while healthy controls were able to memorize about 3.89 (SD = 0.83) items [t(17) = 3.92, p = 0.001].
A repeated measures ANOVA was performed on block span length (memorization of 3, 4, 5, or 6 block positions), with group as between subject factor on serial order. The analyses revealed a main effect of group [F(1,35) = 26.77, p < 0.001, ηp2 = 0.43], indicating a general worse performance for AD patients (accuracy serial order = 58.34%, SD = 0.22) compared to controls (accuracy serial order = 81.51%, SD = 0.14). Also a main effect of block span length was observed [F(1,35) = 149.64, p < 0.001, ηp2 = 0.81], as well as an interaction between group and block span length [F(1,35) = 4.75, p = 0.04, ηp2 = 0.12; Fig. 3A]. Performance decreased with increasing block span length, but the AD patient’s decline with increasing block length was much more pronounced than for the control group. Accuracy scores on serial order for the AD patient group were 80.05% (SD = 0.26), 66.67% (SD = 0.19), 52.00% (SD = 0.22), and 34.65% (SD = 0.20), respectively, for block span size of 3, 4, 5, and 6 elements. For the control group, these accuracy scores were 94.44% (SD = 11.59), 94.44% (SD = 0.09), 76.67% (SD = 0.17), and 60.49% (SD = 0.17).

Visualization of accuracy scores on the Corsi block task, depending on the performed digit span length. A) Accuracy scores on the ‘serial order’ measure. B) Accuracy scores on the ‘any order’ measure. C) Scores on the ‘order ratio’, reflecting the accuracy scores for ‘serial order’ divided by ‘any order’.
The same analysis for the any order measure revealed a main effect of group [F(1,35) = 24.52, p < 0.001, ηp2 = 0.41] and main effect of block span size [F(1,35) = 48.43, p < 0.001, ηp2 = 0.58], but no interaction [F(1,35) = 0.78, p = 0.38, ηp2 = 0.02; Fig. 3B]. The main effect of group again indicated a worse performance for AD patients (83.81%, SD = 0.14) compared to controls (94.45%, SD = 0.06).
Analysis of the order ratio also demonstrated a main effect of group [F(1,35) = 16.46, p < 0.001, ηp2 = 0.32], showing a lower score on the measure for AD patients (order ratio = 0.69, SD = 0.27) than for controls (order ratio = 0.86, SD = 0.17). Again, a main effect of block span length [F(1,35) = 102.60, p < 0.001, ηp2 = 0.75] and interaction [F(1,35) = 6.67, p = 0.01, ηp2 = 0.16; Fig. 3C] were observed. The order ratio scores for the AD patient group for the digit spans of 3, 4, 5, and 6 blocks, respectively, were 0.93 (SD = 0.15), 0.75 (SD = 0.20), 0.59 (SD = 0.23), and 0.46 (SD = 0.25). For the control group these order ratio scores were respectively 0.96 (SD = 0.10), 0.96 (SD = 0.08), 0.82 (SD = 0.16) and 0.69 (SD = 0.15). The larger the to-be-recalled block span was, the worse both groups became at accurately recalling order relative to the recall of specific block items. Performance on order recollection decreased even more strongly in AD patients compared to controls, indicating the quick and specific loss of supportive order representations.
Verbal working memory position task
The verbal WM position task was successfully completed by 30 patients and 25 controls.
This task was meant to investigate the role of directed positional search of information stored within WM. For each participant, an adjusted digit span length was selected, in such a way that the to-be-memorized information did not exceed the participants’ WM capacity. On average, patients reached a digit span length level of 4.20 (SD = 0.76) elements, while controls had an average digit span length of 5.02 elements [SD = 0.77; t(25) = 4.87, p < 0.001]. Importantly, patients and controls made the same amount of errors for their selected digit span length [t(25) = 0.30, p = 0.77], making further analyses of performances between the groups comparable. The average accuracy score for the AD patient group was 69.92% (SD = 0.15), compared to an average accuracy score of 68.45% (SD = 0.10) in controls. Three types of errors were reported: distance errors, intrusion errors, and no-response errors. A repeated measures ANOVA demonstrated that patients and controls equally often made the same types of errors [F(2,22) = 1.39, p = 0.27]. On average, participants made 17.28% (SD = 0.10) distance errors, 8.57% (SD = 0.06) intrusion errors, and 5.02% (SD = 0.06) no-response errors.
For further analyses, paired t-test was performed to investigate the effect of group on the averaged distance scores. The results for the averaged difference scores revealed no effect of group [t(24) = 0.49, p = 0.63], with an average distance score of –0.07 (SD = 0.30) for patients and –0.11 (SD = 20) for controls.
Next, we investigated the consistency of the averaged deviation scores in AD patients and controls. First, a paired t-test was performed in order to assess a left- or right-sided mental deviation. Indeed, on average participants tended to report more earlier WM items, located before the position of the correct letter [t(54) = 2.10, p = 0.04], with an average difference score of –0.07 (SD = 0.26). Second, analyses of the averaged standard deviations observed for the distance scores demonstrated a significant difference between the both groups [t(24) = 2.46, p = 0.02], with a standard deviation of 0.50 for the AD patient group and 0.37 of the control group.
DISCUSSION
This study was designed to shed a light on the mechanisms underlying WM deficits observed in AD patients. A wide variety of tests was conducted to investigate (1) the potential role of an affected central executive attentional system or reduced WM capacity in impaired WM functioning; and (2) to what extent impaired order processing could be the underlying process explaining impairments in the functioning of the central executive/WM capacity.
First, it appeared that the simple reduction of WM capacity as a consequence of AD did not demonstrate to be the core problem located within the WM system, but that the central executive fundamentally contributes to the capacity limit of WM. The WM capacity, as determined by the long forward digit span task, was equal for AD patients and the control group. Interestingly, a reduced WM capacity in AD patients was observed once additional WM operations were required, i.e., during the backward digit span task. Furthermore, a similar observation was made for the verbal WM position task, where an adjusted digit span length was selected for each participant. The selected digit span lengths for AD patients were smaller than for the control group. As the verbal WM position task specifically relied on the allocation of attention to search through WM, one could argue that the hindered allocation of additional cognitive resources led to the observed reduced WM capacity. Overall, these findings suggest an intact WM capacity in AD patients, when tested in a non-demanding task setting. However, the increase of cognitive load, which requires the recruitment of additional (attentional) resources, seems to result in a reduction of WM span. In other words, these findings indicate that WM capacity and the central executive are functions that are at least partially dependent on each other. More specifically, their interdependency is observed in the fact that a reduced WM capacity is associated with the employment of additional cognitive resources by the central executive (e.g., by performing transformational processes or direct internal attention within WM).
Second, and crucially, compromised order processing marks the functioning of the WM system in AD patients. The serial order measure and order ratio of the forward and backward digit span tasks demonstrated that AD patients’ order performances were worse than those of controls. The order ratio specifically demonstrated that the impairment observed for the processing of order was not in proportion to the ability to store a general (non-orderly) memory trace of digits within WM. These tasks show that in AD patients memory for item order is proportionally more impaired than memory for item identity, especially when WM load increases. Moreover, it was observed that AD patients and controls make the same type of errors. This observation suggests that the differences in performances between AD patients and controls are indeed driven by differences in order processing, and not by other problems, such as difficulties with disengaging from automatic and procedural memories [25, 42]. However, note that the reported error scores also entail scores assessing position-specific errors, e.g., such as the ‘within capture errors’ and ‘transposition errors’. Both types of errors represent mistake made on item ordering (i.e., tendency to order in continuous series or tendency to misplace an item without creating a contiguous series of numbers). Intuitively, one could expect that AD patients would produce more order-specific error scores than controls. However, it should be emphasized that while the serial order measure demonstrates to be highly sensitive to the number of errors made against the ordering of items within a sequence, the specific error scores are rather insensitive to the number of order-errors within a sequence. For example, if the original sequence I “35192” and the participant recalls “12359”, we can record one within capture error (i.e., “123”) and two transposition errors (i.e., “5” and “9”), while in reality all numbers were displaced (which is correctly reflected in the accuracy score of serial order; i.e., 0% for this trial).
Furthermore, and importantly, while the previously reported results indicated that AD patients experience trouble with the recall of entire ordered item sequences, AD patients also demonstrated difficulties with the retrieval of position-specific item information within WM. More specifically, when AD patients had to recall the item at a cued location in the sequence, they demonstrated larger variability in deviations with respect to the position of the correct answer compared to controls. While AD patients were equally likely to recall an item stored in WM (and not a random non-WM item) compared to controls, they expressed greater difficulty with the localization of the correct item within WM. The observation that the variability in distance errors is much larger in AD patients than in controls is related to affected goal-directed attentional processes in WM. More specifically, it has previously been demonstrated that searching through WM during item retrieval engages mechanisms of spatial attention [43, 44]. Van Dijck et al. [43] demonstrated that the retrieval of an item from a serial sequence in WM led to the facilitated detection of spatially presented targets matching the mental location of the retrieved item in WM (i.e., item retrieval from begin of the WM sequence led to a shift of spatial attention to the left side of space; item retrieval from the end of the sequence led to an attentional shift to the right). Their findings indicated that spatial attention is crucially involved during item localization and retrieval in WM. In the current study, AD patients specifically demonstrated difficulties with the localization of position-specific item information. This observation indicated that AD patients experience problems with goal-directed search within WM, which is associated with the impaired employment of internal spatial attention [43, 44]. Problems specific to the steering of attention thus affects goal-directed search within WM, leading to the retrieval of incorrect position-specific item information, even if order and item information are properly stored within WM.
Interestingly, serial order problems were not restricted to the verbal domain but also affected visuospatial material, where a reduced WM capacity was assessed using the Corsi block task. Results of the forward and backward digit span task clearly indicated problems with the successful serial processing of information within WM, an observation that was replicated in the Corsi block test. Not only were AD patients worse at the recall of order information, memory for order suffered more strongly than the general memory trace for the visuospatial stimuli, as observed in smaller order ratios for AD patients compared to control subjects. Moreover, the deterioration of these order representations increased when WM load was increased.
However, it is important to note that all observations were made based on the comparison of performances between AD patients and their partners, serving as control group. While medical history screening of the partners did not reveal any pronounced neurological deficits, partners still represent a particular group that cannot simply be approached as a normal aging and healthy group. It has repeatedly been shown that partners of AD patients are known to be at higher risk for depression or anxiety disorders [34, 35]. Also, the average MoCA score of 25.90 in AD patients’ partners indicate that we are not dealing with an entirely healthy group (cut-off for healthy functioning is 26/30). Therefore, it could be the case that the control group of this study may already be experiencing initial stages of cognitive decline. In other words, the group of AD patients and the control group are not necessarily as different as would be the case when comparing to a healthy aging control group. Nevertheless, the current study was able to capture compelling differences between the two groups.
A topic that should be addressed in future research starts from the following observation: a better integrity and level of functioning of WM processes is often associated with the observation of slower functional decline in AD patients [45]. Cognitive training is regularly used to stimulate the development of restorative or compensatory strategies in AD patients, a method that has been shown to be effective for many, but not all, patients ([46, 47]; for a review, see [11]). In light of these observations, and combined with the results of the current study, the effectiveness of cognitive training should be addressed as a possible avenue in the development of cognitive training programs, focusing on order-specific processing problems and the directing of internal attention.
Based on the findings of the current study, we should be aware of the possible overarching impact of impaired order processing on other cognitive functions. For example, AD patients are also known to express reduced language functioning, a cognitive ability that crucially relies on the serial organization of informative components. It has previously been shown that AD patients experience difficulty with verbal expression and auditory comprehension, as well as reading and writing [48]. Moreover, when describing a target picture, AD patients need more words to communicate a similar amount of information compared to controls [49] and express difficulties in the processing of syntactic complexities [50, 51], issues that all might reflect difficulties with the organization of information within WM. Indeed, previous studies have established a link between WM and language impairments in AD [52]. However, the explanation for the observed link between the two has been hindered by a lack of clarity concerning the underlying affected WM mechanisms. Therefore, insights provided by the present study might be implemented to investigate their immediate effect on other impaired cognitive domains, such as language processing. Moreover, if the processing of serial order turns out be a determinant of the integrity of other cognitive functions, further research should investigate whether the assessment of order processing could facilitate early AD diagnosis or serve as a predictor for future cognitive decline in healthy people or patients diagnosed with mild cognitive impairment.
In sum, the current study sought to clarify the mechanisms that underlie deficient WM functioning in AD patients, and found that the reduced size of WM capacity in AD patients may not be the core problem, but that the functioning of the central executive plays a more important role in WM problems. Observations of reduced WM capacity were only observed when additional WM (order-related processing) operations were required. Moreover, the goal-directed control of attention was shown to be seriously affected, and matched more closely with the viewpoint of a dysfunctional central executive. Second, impaired performance in AD was shown to be related to the impaired processing of serial order within a spatial coordinate WM system, both for verbal and visuospatial information. Note that future research should investigate at what level of information processing order processing comes into play. Serial order processing seems to be related to the functioning of the central executive. However, we cannot exclude the fact that order might be so fundamental to behavior that order processing might occur beyond the central executive, and serves to bind the central executive to short-term storage systems.
Overall, in the context of serially organized WM, AD patients demonstrate two crucially compromised WM components: (1) difficulty with the representation and processing of order and (2) an impaired employment of internal spatial attention, marking the role of an affected central executive.