
Abstract
INTRODUCTION
The motoric cognitive risk syndrome (MCR) is characterized by cognitive complaints and slow gait in older individuals [1–3]. MCR increased risk of developing cognitive impairment and dementia in elderly cohorts based in USA and Europe [1, 2]. Few studies based in Japanese cohorts have investigated prevalence and etiologies of MCR [4, 5], but the risk of incident dementia associated with MCR in Japan has not been reported [1]. Due to potential biological differences between races, e.g., genetic pattern related to dementia [6], it is important to examine the etiology of MCR and its association with dementia in different countries to obtain biological insights and to develop global dementia preventive strategies.
The increasing elderly population in Japan is projected to be accompanied by higher rates of dementia [7] and disability [8]. It is plausible that MCR may be associated with increased risk of health-related outcomes among older adults given that its cognitive and motoric components are individually associated with increased risk of disability. If MCR was shown to be contributing to risk of not only dementia but also disability, this clinical construct that does not require extensive neuropsychological tests or biomarkers would acquire further importance from a public health perspective. Hence, to further elucidate the epidemiology of MCR in Japan, we conducted a prospective study to establish the relationship of MCR with risk of dementia and disability.
METHODS
Study design
Participants eligible for this study were selected from older Japanese adults enrolled in a population-based cohort study: the Obu Study of Health Promotion for the Elderly (OSHPE) [9] that was part of the National Center for Geriatrics and Gerontology – Study of Geriatric Syndromes [10]. Recruitment was conducted via a letter sent to 14,313 individuals aged 65 years or older living in Obu city; 5,104 of these individuals participated in the OSHPE in 2011–2012 at baseline. Exclusion criteria were not using Japanese National Health Insurance or Latter-Stage Medical Care (that provides medical insurance coverage for about 87% of older adults in Japan), diagnosis of dementia of any subtype at baseline (recorded in the insurance system medical records or diagnosed at the baseline study clinical interview), certification by long-term care insurance (LTCI), requiring assistance or unable to do independently basic activities of daily living (ADL), or history of cardiovascular disease, Parkinson’s disease, or depression. These diseases had specific impacts on incident of dementia and disability [11, 12]. In addition, 14 participants with missing data on MCR and other study variables were excluded. Hence, 4,235 participants (82.9%) were eligible for this study. All participants provided written informed consent, and the ethics committee of the National Center for Geriatrics and Gerontology approved this study.
MCR criteria
MCR was defined as having subjective cognitive complaints and slow gait in older adults without dementia or mobility disability [2]. MCR criteria builds on operational criteria for mild cognitive impairment (MCI) syndrome [13], described elsewhere [1–4]. In our study, the presence of subjective cognitive complaints were elicited from the standardized question about memory loss on the 15-item Geriatric Depression Scale (GDS): “Do you feel you have more problems with memory than most?” [14]. The same operational definition of subjective memory complaints was used in 8 out of the 22 cohorts included in the worldwide MCR prevalence study [1]. Gait speed at normal pace was measured over a 6.4 m level course in a well-lit area, and 2 m at either end of the course was not included in the measurement to account for initial acceleration and terminal deceleration. Participants were instructed to walk at their normal comfortable pace. The walking time over the 2.4 m middle portion of the course was converted to speed (m/s) [9]. Slow gait was defined as gait speed at normal pace that was 1.0 standard deviations or below age- and sex-appropriate mean values established in this cohort, according to established protocol [1]. In prior studies, MCR was shown to have improved predictive validity for dementia compared to its individual components of subjective cognitive complaints or slow gait [1]. Strengths of the MCR construct are that slow gait is defined objectively, independent of clinical gait evaluations that may be prone to variable sensitivity and specificity as well as being examiner dependent. Though gait dysfunction is multifactorial in nature, previous studies have shown that slow gait predicts cognitive decline irrespective of the underlying etiology [15]. Subjective cognitive complaints do not require formal cognitive testing, but have been reported to be associated with reduced cognitive function and increased risk of dementia [16, 17].
Incident dementia
Incident dementia was defined when a participant who was non-demented at baseline was given a new diagnosis of dementia on follow-up based on data collected by the Japanese Health Insurance System. In Japan, all adults aged 65 years or older have public health insurance that is composed by following insurances: 1) employee’s health insurance for employed individuals (Employees’ Health Insurance), 2) national health insurance for self-employed individuals and those out of employment that covers individuals aged 65–74 (Japanese National Health Insurance), and 3) the healthcare system for later-stage elderly for the people aged 75 years or older (Later-Stage Medical Care) [18, 19]. Participants were tracked monthly in our study for new diagnoses of incident dementia (AD or the other subtypes of dementia) recorded in the Japanese National Health Insurance and the Latter-Stage Medical Care System for the elderly. Dementia status was assigned to be based on diagnosis by medical doctors according to International Classification of Diseases-10 [18, 19]. We have utilized the similar approach to report incidence of dementia in previous studies [20]. While the Japanese medical records system provides a comprehensive coverage, limitations of relying on diagnostic coding have been noted [21]. Hence, we did not examine or report associations of MCR with subtypes of dementia. During follow-up, moving out of Obu city and death was treated as censoring events for the survival analysis. Given the relatively short follow-up period from the baseline examination in 2011 to 2014 (mean follow-up duration: 29 months), our focus was on the short-term prediction of dementia. Nonetheless, the approximately two-year follow-up period is a practical window for making predictions and instituting interventions in clinical settings.
Incident disability
During the follow-up period, we tracked incident disability, which was operationally defined as receiving LTCI certification. The process of certification in LTCI has been described elsewhere [22]. A medical doctor of primary care evaluated the need of LTCI and a trained local government healthcare official evaluates needs for nursing care using a questionnaire that assesses current physical and mental status (73 items) and using information about medical conditions (12 items) (e.g., treatments received or medication regimes). The results are entered into a computer to calculate the applicant’s standardized scores for the seven dimensions of physical and mental status, estimate time of care, and assign a care-needs level based on the total estimated care minutes. The Nursing Care Needs Certification Board (physicians, nurses, and other experts in health and social services appointed by a mayor) reviews whether the initial assessment is appropriate in each assessed individual, considering the applicant’s primary care physician’s statements and notes written by the assessor during the home visit. In this study, the outcome of disability was defined as a new requirement of LTCI service certified at any support or care level over study follow-up. Several previous Japanese studies including from our cohort have used the same approach to define disability using LTCI certification [23, 24]. We tracked the disability status information, which was updated monthly. During follow up, moving out of the city and death was treated as censoring events. Similar to the dementia analysis described above, we focused on short-term prediction of disability from the baseline examination in 2011 to 2014 (mean follow-up duration: 29 months).
Covariates
Based on previous studies of risk factors related to MCR and dementia [3, 25], we selected several potential modifiable risk factors at baseline. We selected specific medical diseases [3, 25], depressive symptoms [3, 25], and falls that have been related to both mobility and cognitive impairment in previous studies [4]. Participants were interviewed by nurses about the presence or absence of selected chronic diseases (hypertension, diabetes, heart disease, and hyperlipidemia) and medications (total number). Major depressive symptoms (15-item GDS scores >5) [14] and occurrence of any falls over the previous year were recorded at baseline. We also assessed the following lifestyle factors that were associated with dementia risk in previous studies [3, 25]: obesity, physical inactivity, smoking, and alcohol consumption. Based on height and weight, body mass index (BMI: kg/m2) were calculated, and obesity was defined as BMI value of 25 kg/m2 and over as previously described in the Japanese elderly population [26]. Physical inactivity was defined by two questions used in a previous study [9]: (1) “Do you engage in moderate levels of physical exercise or sports aimed at health?” and (2) “Do you engage in low levels of physical exercise aimed at health?”. The moderate or low level was based on subjective reports by participants of the intensity of effort on physical activities. Physical inactivity was defined as not engaging both low and moderate levels of activity, responding “no” to both these questions. Current smoking and alcohol consumption were also noted.
Statistical analysis
At baseline, characteristics including covariates were compared between ‘no MCR’ and ‘MCR’ groups using unpaired-t-test or χ2 test. To examinethe association of MCR with incident cases of dementia and disability, Kaplan–Meier survival risk assessments were used to plot survival curves, and the results for each group were compared using log-rank tests. Cox-proportional hazards regression models were used to determine the risk of incident dementia and disability associated with MCR, and reported as hazard ratios (HR) with 95% confidence intervals (95% CI). Prevalent cases of dementia and disability were excluded from the respective analyses. Model 1 was the crude unadjusted model. Model 2 added the following covariates based on prior MCR and dementia studies [3, 25]; age, sex, educational history, chronic diseases (hypertension, diabetes, heart disease, and hyperlipidemia), number of medications used, previous falls, major depressive symptom, obesity, alcohol consumption, current smoking, and physical inactivity. As a sub-analysis, cox-proportional hazards regression analysis was also conducted to compare individual groups (MCR, slow gait alone, cognitive complaints alone) with control group (both no slow gait and no cognitive complaints). In addition, we examined the competing risk of incident dementia on the association between MCR and disability, because dementia can cause disability [27]. We stratified participants by incidence of dementia during follow-up into the following groups; no MCR without dementia, no MCR with dementia, MCR without dementia, MCR with dementia. The association between these groups and incident disability was analyzed using cox-proportional hazards regression models that adjusted for the same covariates as in Model 2. All analyses were performed using SPSS statistics software, Version 20 (IBM Corp., Chicago, IL, USA). Statistical significance was set at p < 0.05 in all analyses.
RESULTS
Of the 4,235 participants (50% women, mean age: 72.0 years), 265 (6.3%) were classified into MCR and 3,970 (93.7%) as No MCR. Table 1 summarizes baseline characteristics by MCR group. Among the variables examined, education, obesity, physical inactivity, diabetes, depressive symptom, previous falls, medication numbers, and gait speed showed significant group differences with worse performance, as expected, in the MCR group.
Characteristics in subjects between No MCR and MCR groups
MCR, motoric cognitive syndrome. Values are mean (SD) or proportion.
During the study follow-up (mean duration: 29 months), there were 138 incident cases of dementia (3.3%). Kaplan–Meier survival curves inFig. 1 showed that the presence of MCR at baseline was a significant risk factor for dementia (p < 0.001). The Cox-proportional hazards regression models also showed significant hazard ratio of MCR for dementia compared to the No MCR group (Table 2). In sub-analysis, MCR was a better predictor of dementia (model 1: HR 4.29 [95% CI 2.57–7.16], p < 0.001; model 2: HR 3.18 [95% CI 1.83–5.54], p < 0.001) compared to its individual components of slow gait alone (model 1: HR 1.37 [95% CI 0.67–2.80], p = 0.385; model 2: HR 1.19 [95% CI 0.58–2.45], p = 0.641) or cognitive complaints alone (model 1: HR 1.96 [95% CI 1.31–2.93], p = 0.001; model 2: HR 1.58 [95% CI 1.03–2.42], p = 0.034).
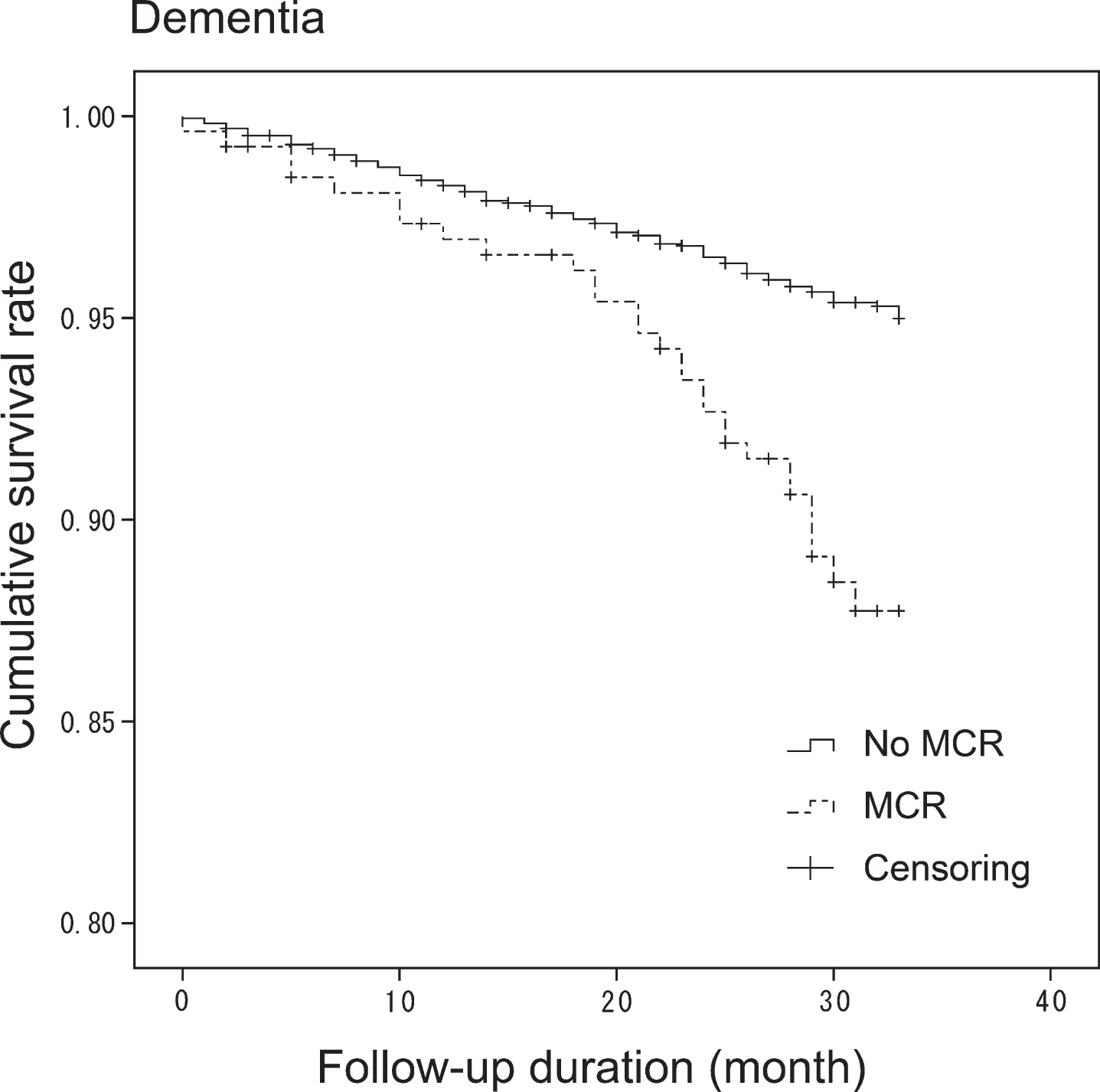
Kaplan-Meier survival-curve for dementia in MCR. Cumulative survival rates were plotted in No MCR and MCR groups for dementia. Log-rank test showed that MCR was significant risk for dementia (p < 0.001).
MCR and incident outcome
HR, hazard ratios; CI, confidential interval. Adjusted Model was analyzed individually adjusted for age, sex, education, life style (obesity, smoking, drinking alcohol, physical inactivity) and medical conditions (diseases, medication numbers, depressive symptom, fall).
During follow-up (mean duration: 29 months), 207 (4.9%) incident cases of disability were diagnosed. Kaplan–Meier survival curves showed in Fig. 2 that the presence of MCR at baseline was a significant risk factor for disability (p < 0.001). In Cox-proportional hazards regression analysis, MCR was significant risk for disability (Table 2). In sub-analysis, MCR was a better predictor of disability (model 1: HR 3.31 [95% CI 2.11–5.21], p < 0.001; model 2: HR 2.25 [95% CI 1.39–3.67], p = 0.001) compared to cognitive complaints alone (model 1: HR 1.61 [95% CI 1.15–2.26], p = 0.006; model 2: HR 1.32 [95% CI 0.92–31.89], p = 0.128), and had similar predictive validity for disability compared to slow gait alone (model 1: HR 3.46 [95% CI 2.30–5.19], p < 0.001; model 2: HR 2.86 [95% CI 1.89–4.35], p < 0.001).
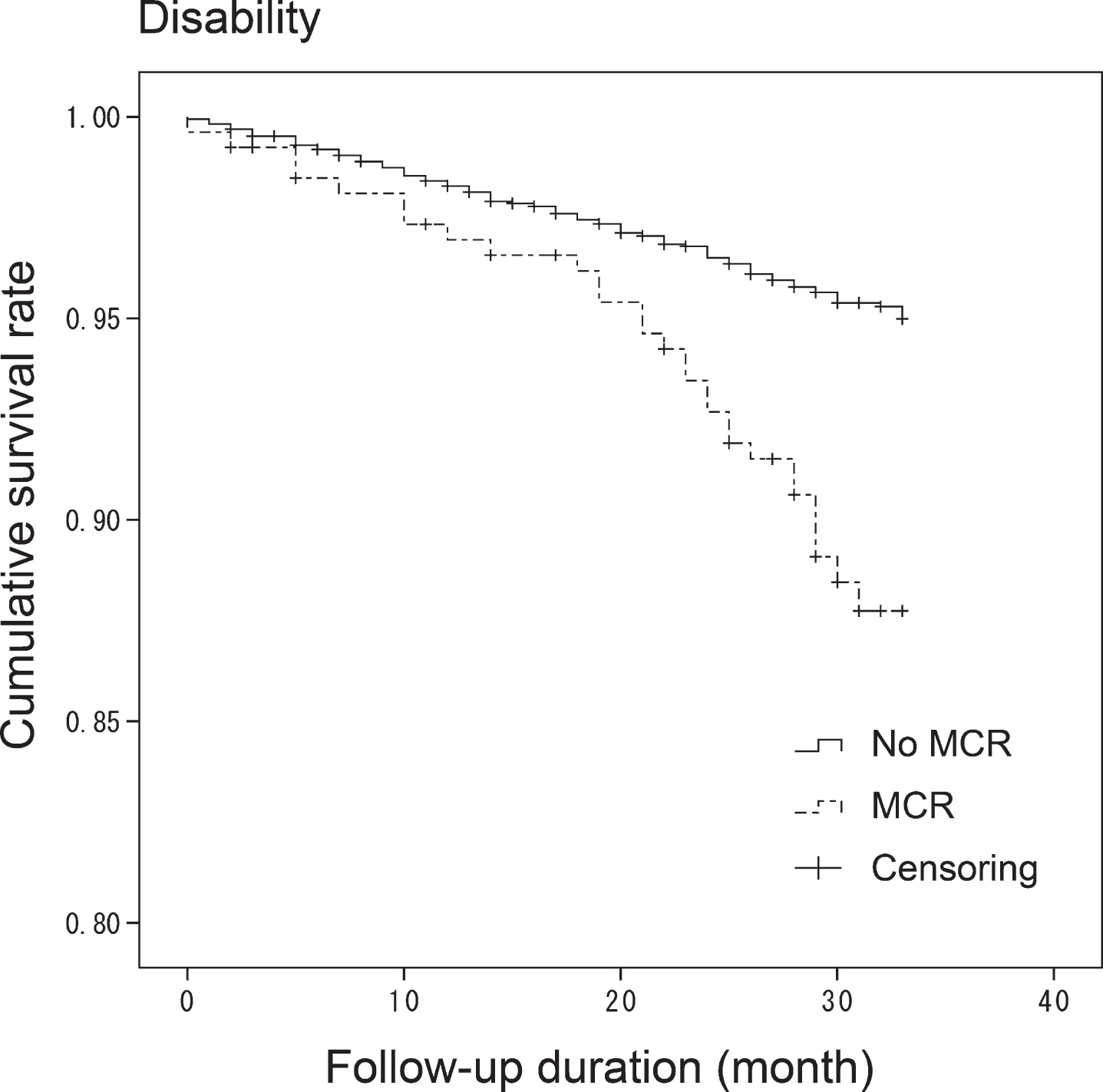
Kaplan-Meier survival-curve for disability. Cumulative survival rates were plotted in No MCR and MCR groups. Log-rank test showed that MCR was significant risk for disability (p < 0.001).
The secondary analysis stratified by incidence of dementia to account for the competing risk of dementia on disability showed that the no MCR with dementia (model 1: HR 13.22 [95% CI 8.95–19.5], p < 0.001; model 2: HR 6.33 [95% CI 4.22–9.47], p < 0.001) and MCR with dementia (model 1: HR 30.61 [95% CI 17.51–53.51], p < 0.001; model 2: HR 11.88 [95% CI 6.50–21.71], p < 0.001) were significant risks for disability referred to no MCR without dementia, while MCR without dementia (model 1: HR 1.72 [95% CI 0.92–3.19], p = 0.088; model 2: HR 1.24 [95% CI 0.66–2.35], p = 0.503) was notsignificant.
DISCUSSION
This study revealed that MCR was a strong short-term predictor of risk for dementia and disability in Japanese community-dwelling older adults. The relationship of MCR with dementia and disability remained even after adjustment for several established dementia and disability related covariates. The mean follow-up interval was 29 months; this two-year interval is a practical and useful window for risk assessment for clinicians seeing patients in clinical or community settings. Furthermore, given that MCR does not require detailed cognitive testing or equipment to diagnose, the clinical utility of this clinical prognostication approach is further confirmed.
Our findings are in line with the results of the few prior studies based in Western populations, which showed that MCR was a risk factor for all cause dementia [1, 2]. Our estimates for the risk for developing incident dementia associated with MCR at baseline (adjusted HR 2.49) were in accord with the results of the previous multi-country study (HR 1.93–2.72) [1, 2], despite differences in follow-up duration and geographical locations. It is likely that a longer follow-up would strengthen the predictive validity of MCR in our cohort. MCR was a better predictor of dementia than either slow gait or cognitive complaints, confirming findings in other population based cohorts [1]. MCR was a better predictor of disability than cognitive complaints. However, MCR had comparable predictive validity for disability as slow gait. This finding is not unexpected as slow gait may capture other non-cognitive pathways leading to disability [28]. Interestingly, other studies have also expanded the clinical utility of MCR into predicting non-dementia outcomes such as mortality [29] and falls [30].
Previous studies based in Japan and elsewhere have shown that MCR is related to several risk factors including lifestyle (physical inactivity, obesity), depressive symptoms, and medical conditions (hypertension and diabetes) [3, 4]. These modifiable factors overlap with reported risk factors for dementia [25, 31]. For example, physical inactivity is risk for MCR and dementia [3, 25], as well as brain atrophy [32]. Clinical trials to enhance physical activity using exercise programs have shown improvements in cognition in healthy older adults and with MCI [33, 34]. Hence, these results raise the possibility of developing common strategies to prevent conversion of MCR to dementia. Furthermore, the dementia risk associated with MCR may be related to underlying pathological changes of dementia. Previous studies have linked the individual components of MCR to dementia pathology [35, 36].
To our knowledge, this study is the first to report that MCR is also a risk factor for disability in older adults. Declines in physical and cognitive function have been independently recognized as risks for disability [37–39]. Hence, it is plausible that the combination of cognitive and physical impairments could further increase the risk for becoming disabled. The co-occurrence of MCI and slow gait, which may overlap with the MCR definition, was reported to be associated with higher risk of disability compared to only MCI or only slow gait [40]. Our results in the planned sub-analysis revealed that the disability risk of MCR is possibly explained by the risk of disability associated with incipient dementia. The risk of incident disability was higher in individuals with and without MCR at baseline who then developed dementia compared to individuals without MCR who did not develop incident dementia. Another explanation for the contribution of MCR to risk of disability may be due to its associated risk factors. For example, physical inactivity and depressive symptoms are risk factors not only for MCR [3, 4] but also disability [41, 42]. Rist et al. suggested modified these factors related to delay for disability even among dementia [27]. Thus, MCR was useful for early detection of risks for disability and preventive strategies for disability.
The strength of our study included a large well-characterized cohort, prospective design, and reliable outcomes. As MCR does not required neuropsychological tests and gait speed is commonly used in health assessment in older adults without requiring elaborate equipment, it was highly feasible to apply and diagnose MCR in our Japanese clinical and community settings. Some limitations need to be noted. The prevalence of our study (6.3%) were relatively lower compared to the worldwide study (9.7%) [1]. The difference of prevalence was also observed in the other Japanese cohort (11.1%) [5]. These differences were partly due to differences of subjects’ characteristics. The participants in our study were younger and more robust compared to the other cohorts. In addition, samples in our study were relatively large compared to the other cohorts [1, 5]. These differences may affect results. Further study should elucidate the difference of MCR prevalence between cohorts. Then, the diagnostic procedures for our study outcomes of dementia and disability were based on a systematic methodology implemented by medical doctors, and introduced by the Japanese government [18, 19], and employed and reported in other Japanese studies of dementia and disability [23, 43]. Information on incident dementia was derived from data from the Japanese national health insurance system and disability diagnosis was based on the LTCI certification. While medical records have been used to define the incidence of diseases including dementia [18, 19], it is a limitation. More systematic assessments and longer follow-up might have revealed additional cases of dementia and disability, and our reported associations may be an underestimate of the risks associated with MCR. Future studies utilizing systematic prospective assessment protocols are needed to follow up on our results and also to discriminate predictive validity of MCR for subtypes of dementia. Finally, our study selected participants according to inclusion and exclusion criteria. Although exclusion criteria included specific diseases (cardiovascular disease, Parkinson’s disease, or depression) due to the potential affecting results of dementia and/or disability [11, 12], the association between MCR and these diseases were still unclear. Further study would be required to generalize the study findings.
In conclusion, our large cohort study revealed MCR, a simple clinical risk assessment, predicted risk of developing both dementia and disability. These findings could contribute to improving current health risk assessments and to develop prevention strategies for dementia.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the Obu city office for help with participant recruitment. This work was supported by Health and Labour Sciences Research Grants (Comprehensive Research on Aging and Health); Grant-in-Aid for Scientific Research (B) (23300205); Grant-in-Aid for Young Scientists (A) (15H05369) and Research Funding for Longevity Sciences (22-16) from the National Center for Geriatrics and Gerontology, Japan.