
Abstract
The Alzheimer’s Disease Assessment Scale’s cognitive subscale (ADAS-Cog) is the most widely used instrument for screening cognitive dysfunction in Alzheimer’s disease. The aim of the present study was to develop an Arabic version of this scale (A-ADAS-Cog), examine its psychometric properties (reliability and validity), and provide normative data. The A-ADAS-Cog), an Arabic version of the Mini-Mental State Examination (A-MMSE), and a Standardized Clinical Dementia Rating Scale (CDR) were administered to three Tunisian groups: 124 normal controls (NC), 33 patients with non-Alzheimer dementia (N-AD), and 25 patients with Alzheimer’s disease (AD). The A-ADAS-Cog scores were significantly affected by age and education. A correction table was constructed to control these effects. The results showed that the A-ADAS-Cog has good internal consistency and reliability (α= 0.82 for AD). The test-retest reliability of the A-ADAS-Cog was stable over time (r = 0.97). An evaluation of the construct validity of the A-ADAS-Cog using principal component analysis led to a solution with three factors (memory, language and praxis), which explained 72% of the variance. The concurrent validity of the A-ADAS-Cog was established using the A-MMSE score (r = –0.86), CDR Sum of Boxes score (CDR-SB; r = 0.87), and global CDR score (CDR-Global; r = 0.74). Finally, the A-ADAS-Cog has an excellent discriminating power in the diagnosis of AD (ROC area = 0.92). A cut-off score of 10 (sensitivity = 84% and specificity = 91%) is indicated for the screening of the AD. Overall, the results indicated that the A-ADAS-Cog is psychometrically reliable and valid and provides promising results for screening of dementia in Arabic speaking patients.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a progressive neurological degeneration characterized by insidious onset of multiple cognitive and non-cognitive deficits, which are manifested not only as impairments in memory, language, orientation, and praxis but also depression, agitation, hallucinations, and delirium [1]. Therefore, neuropsychological assessment of AD requires evaluation of both cognitive deficits and various aspects of altered behavior. The Alzheimer’s Disease Assessment Scale (ADAS), which was developed by Rosen, Mohs, and Davis in 1984 [2], is a neuropsychological screening tool designed to meet these objectives. The ADAS consists of two parts: a scale composed of 11 subtests that evaluate the severity of cognitive impairment (ADAS-Cog) and a clinical assessment scale of behavioral disorders (ADAS-non-Cog) that consists of 10 subtests. The two parts can be used separately. Since its development, this tool has become a benchmark for assessing short- and long-term progression of the major neuropsychological symptoms of AD [2–5]. The non-cognitive part of the ADAS is more clinical, and some longitudinal studies have indicated that the non-cognitive symptoms of AD, such as agitation, depressed mood, and psychotic symptoms (delusions and hallucinations), are episodic, do not deteriorate with time and are not highly correlated with AD [6]; therefore, in this study, we will focus on the ADAS-Cog.
Several studies have concluded that the ADAS-Cog is not only beneficial for assessing the severity of AD-associated dysfunctions and monitor symptom progression during longitudinal studies [5, 7–9] but can also be used for early detection of AD [10–12], to differentiate between AD and normal aging [10, 13], and to differentiate between AD and other diseases, such as vascular dementia [6, 14] and depression [12].
The ADAS-Cog has become a widely used tool in clinical neuropsychology. It has been translated and adapted to many languages and cultures, including French [15, 16], Spanish [17], Italian [18], Greek [14], Slovak [12], Chinese [19], Brazilian [20], and Turkish [21]. However, to date, there is no Arabic version of the ADAS-Cog. A search of the major academic databases (PsychINFO, Elsevier, ERIC, Medline, PsycARTICLES, and PubMed) conducted on March 26, 2016, using the key words “ADAS” and “Arabic” returned zero publications. Therefore, there is a strong need to develop an Arabic version of the ADAS-Cog that can be used in clinical and research settings to serve the nearly 450 million Arabic-speaking individuals worldwide.
In its original version and in several adaptations, the ADAS-Cog includes subtests that involve reading and drawing tasks to assess verbal memory and constructive praxia, respectively. Despite the many advantages of the ADAS-Cog, similar to other neuropsychological assessment tools [25], performance on the ADAS-Cog is negatively affected by low levels of education [20, 26–29]. Therefore, it is essential to avoid using reading and drawing tasks in cognitive assessments to prevent underestimation of cognitive capacities [28]. Furthermore, reading and drawing are usually learned in school, but most of the ADAS target populations in Africa and Arabic countries are illiterate. In these countries, the percentage of illiterate people aged 60 and over is very high: 86.2% in 2003 for Morocco [22] and 84.9% in 2004 for Tunisia [23]. Moreover, up untill 2010, the illiteracy rate in the Arab countries for the youth population aged between 15–24 years is still high: 22.3% [24]. This suggests that the reading and drawing tasks, which are not appropriate for illiterate subjects, will be pointless once used in the detection or assessment of dementia for almost a quarter of the population for some other decades.
Although most studies agree that education affects performance on the ADAS-Cog, there is less agreement regarding the effect of age. Fioravanti et al. [18] and Graham et al. [31] reported that advancing age negatively affects performance on the ADAS-Cog. However, Hannesdottir and Snædal [32] (using the Icelandic version) and Wang et al. [33] (using the Chinese version) failed to show an effect of age on ADAS-Cog performance. In addition, no studies have examined whether gender affects performance on the ADAS-Cog.
Clinically, the ADAS-Cog is sensitive to the progression of AD and the degree of dementia severity. It is estimated that the mean change in the ADAS-Cog score is 7 to 8 points over two years. Among the subtests of the ADAS-Cog, the orientation subscale and the overall score seem to be most correlated with the severity of dementia [10].
The present study has three main aims: to present the rationale for adapting the ADAS-Cog to Arabic (A-ADAS-Cog), to examine the psychometric properties of the A-ADAS-Cog, and to provide normative data from a sample of elderly controls. This normative data can be used for clinical decisions and for cross-cultural studies in the field.
METHOD
Rationale of the Arabic version of the A-ADAS-Cog
The aim of adapting the ADAS-Cog was to respect the fundamental practical goals of the original version while meeting the specific cultural and linguistic needs of the Arab population. Because the lists of words in the memory and the naming subtests are likely to be influenced by cultural differences, special attention was devoted to select the words for these lists. In fact, for the choice of stimuli, we did not base this action on the translation/backtranslation of the items but we established our decision on the equivalence principle. While keeping the same categories of the items, the words were selected from an Arabic database [35] according to the level of the frequency in the semantic category, word agreement, and imageability. In each semantic category, the chosen words had an order of frequency ranging from 6 to 20, allowing us to avoid prototypical and infrequent items.
To control the word length variable, we frequently used bi- or tri-syllabic words with a high degree of imageability. We reduced the reading and writing components of the original ADAS-Cog to not disadvantage or exclude illiterate or low educated subjects. Therefore, during the word recall subtest, the experimenter read the items to the patient. In addition, we considered the nature of the categories during the word recall subtest. Therefore, for the 10 word categories, 5 were living objects, and 5 were non-living objects, which would allow us to detect any specific categorical impairments. Studies have shown that categorical impairments exist in AD [36–38], and these results have fueled a debate regarding the nature of semantic memory deficits in AD [39, 40]. Similar precautions were taken in the naming subtest, in which we replaced the culturally or academically loaded items while ensuring that there were real and familiar objects in the categories of living objects and non-living objects.
To minimize the risk of interference between the word recall and recognition subtests, we ensured that they did not cover the same semantic categories.
For the orientation subtest, we replaced the questions about the patient’s name (which are asked during the clinical interview), date and year (which may be a disadvantage to uneducated people) with questions regarding the governorate, city and country that the test was administered in; these questions provide additional information about the spatial orientation and temporal dimensions of autobiographical episodic memory.
To further eliminate disadvantages to illiterate individuals, the writing component of the ideational praxis subtest was replaced with a task where the subjects were asked to light a candle and put it out. We maintained the number of components to perform and their complexity. Finally, we have changed the design of the constructional praxis subtest by replacing it with a task that does not require the subject to use educational skills (the subject is asked to reproduce 4 geometric figures of increasing difficulty, using matches likewise in the Stick Test).
In total, the adaptation process was constantly guided by the five facets of cross-cultural equivalence (content, semantic, technical, criterion, and construct equivalence) described by Flaherty et al. [34].
Population
This study consisted of 182 subjects, which were divided into three groups:
A group of 25 AD patients, ranging in age between 50 and 89 years old, who were diagnosed with AD based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition [41] and the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ARDRA) criteria [42]. The AD group is composed of 13 males and 12 females with a mean age of 69.40 years (SD = 8.59) and a mean education of 6.60 years (SD = 6.65). In this group, the Arabic version of the Mini-Mental State Examination (A-MMSE) [48] mean score was 22.04 (SD = 4.19).
A group of 33 patients with non-Alzheimer dementia (N-AD), aged between 50 and 87 years old, who were diagnosed based on the DSM IV [41] and the latest consensus for the different types of dementia [42–47]. This group is composed of 18 patients suffering from vascular dementia, 9 with Lewy body dementia, and 6 patients with frontotemporal dementia. The N-AD group is comprised of 16 males and 17 females with a mean age of 69.06 years (SD = 6.27) and a mean education of 6.11 years (SD = 3.82). In the N-AD group, the A-MMSE mean score was 25.33 (SD = 2.79).
In both dementia groups, the A-MMSE scores for all cases were superior to 15 and the Clinical Dementia Rating scale (CDR) [49] scores were 0.5 or 1.
A control group that consisted of 124 normal subjects, aged between 50 and 95 years old, with no cognitive or conative complaints and completely independent in terms of their daily living activities. This group is composed of 59 males and 65 females with a mean age of 68.15 years (SD = 7.13) and a mean education of 5.44 years (SD = 5.74). The A-MMSE mean score for the NC was 28.33 (SD = 1.35). There were no statistically significant differences in age, sex, or education among the three groups. All the subjects lived in their family environment and had no neurological and/or psychiatric history. All subjects provided informed consent to participate in the study. The demographic characteristics of the study population are shown in Table 1.
Demographic characteristics of the study population
Procedure
All participants were individually examined in the neurology department at Charles Nicolle Hospital. For diagnosis, all subjects underwent a detailed history using the Neuropsychological Status Examination [50] and the Neuropsychological Questionnaire [51]. In addition, all patients underwent detailed neurological, biological and neuroimaging (CT, MRI, and/or SPECT) exams in addition to a thorough neuropsychological examination of cognitive (e.g., language, memory, praxis, and gnosis) and conative functions.
Statistical analysis
The effect of the sociodemographic variables was tested using a series of stepwise multiple linear regression (MLR) analyses for the global A-ADAS-Cog score to determine the corresponding weight of each variable on performance and make the necessary corrections to the scores.
Reliability (internal consistency) was estimated by calculating Cronbach’s alpha for the entire population and for each group separately. For test-retest reliability, Pearson Product Moment Correlation Coefficient was used to assess performance stability over time on 54 subjects who were re-tested 4 to 6 weeks after the initial assessment using the A-ADAS-Cog.
Three aspects of validity were analyzed: The construct validity was examined using principal component analysis (PCA) with varimax rotation to identify the main dimensions of the scale that explained the majority of the variance in the study variables. The concurrent validity was analyzed to assess the degree of agreement of the A-ADAS-Cog with two other dementia scales by calculating the Pearson Product Moment Correlation Coefficient: the overall adjusted scores of the A-ADAS-Cog with the adjusted scores of the A-MMSE [48] and with the CDR Sum of Boxes (CDR-SB) score and the global CDR (CDR-Global) scores [52]. Receiver operating characteristic (ROC) analysis was used to verify the clinical validity of the A-ADAS-Cog for diagnosis of AD. The results of the ROC analysis were used to determine the cutoff score for the A-ADAS-Cog. For each potential cutoff score, we calculated the 95% confidence interval for the sensitivity and specificity, the Pearson’s correlation coefficient, the kappa statistic (degree of concordance) and the p-value (McNemar’s test).
All statistical analyses were performed using the software package ‘IBM SPSS Statistics for Windows, version 23’ [53].
RESULTS
A comparison of the average A-ADAS-Cog scores among the three groups showed that this tool clearly discriminates the subjects [F(2, 181) = 64.36; p < 0.001; partial eta squared = 0.42]. The average performance of the AD group was significantly higher than that of the other two groups (p < 0.001). The control group had the best average scores, which leveled off in many of the subtests except those involving episodic memory (word recall and recognition) and to a lesser extent, constructional praxis.
A group×subtest analysis of variance (ANOVA) showed there was a significant group effect [F(2, 179) = 64.03; p < 0.001; partial eta squared = 0.41], an expected significant subtest effect [F(10, 1790) = 256.83; p < 0.001; partial eta squared = 0.66], and a significant interaction [F(20, 1790) = 8.99; p < 0.001; partial eta squared = 0.12].
Post-hoc analysis using the Tukey’s Honestly Significant Difference (HSD) test revealed that the NC group performed significantly better than the AD group in four subtests: word recall, recognition, orientation, and constructional praxis (all ps < 0.001). Furthermore, the scores of NC group was significantly different from N-AD group only in the recall subtest (p < 0.001), whereas the A-ADAS-Cog was able to clearly distinguish between the AD and N-AD groups in three subtests: recall, orientation, and constructional praxis (all ps < 0.01).
Effects of sociodemographic variables
The results of an MLR on the control group showed that the A-ADAS-Cog scores were significantly affected by age, sex and level of education (R2 = 0.19; p < 0.001). Table 2 showed that unlike sex, age, and the level of education are strong predictors of the A-ADAS-Cog global score. Hence, a correction is required in order the adjust raw scores. Table 3 was established for the A-ADAS-Cog global score based on the results of the MLR. A control MLR was performed on the entire study population to show that the corrected global score was dependent on the variables of age and education.
Effects of the sociodemographic variables on the A-ADAS-Cog global score
*MLR, multiple linear regression; **B, non-standardized coefficient, β***, standardized coefficient.
Global score correction table for the A-ADAS Cog
Analysis of reliability
The internal consistency
For the AD group (n = 25), the internal consistency of the A-ADAS-Cog was good (alpha = 0.82) and all of the subtests were significantly correlated to the total scores (Table 4). This suggests that the A-ADAS-Cog is internally consistent for assessing AD patients.
The internal consistency coefficients of the A-ADAS-Cog for AD group
The test-retest reliability
For test-retest reliability, 54 subjects (15 AD, 20 N-AD, and 19 NC) were retested by the same clinician at 4–6 weeks after the initial assessment. Test–retest correlation coefficient for each sample was calculated separately. The test-retest reliability was excellent for the AD (r = 0.97) and N-AD patients (r = 0.93) and good for the NC subjects (r = 0.87). Overall, the test-retest reliability was very high (r = 0.97). This indicates that performance on the A-ADAS-Cog is stable over time.
Therefore, the A-ADAS-Cog is a reliable scale that has good internal consistency and performance stability over time.
Analysis of the validity
Construct validity
The A-ADAS-Cog construct validity was examined using PCA with varimax rotation to highlight the dimensions of the scale that explains the variance between the variables. The analysis was conducted on a sample of 25 AD patients, and it was determined that three factors explain 72% of the variance (Table 5).
Main factors identified by the Varimax rotation in PCA on AD patients’ data
Bold values correspond to the highest saturation coefficient as generated by each factor load.
The first factor (memory) explains approximately one-third (30%) of the observed variance and includes the remembering test instructions, word recall, orientation, recognition, naming, and constructional praxis subtests (Table 6). The second factor (language) includes both expressive and receptive aspects of language. Language explains 26% of the total observed variance and includes the spoken language, comprehension and word finding subtests. The third factor (praxis) explains 16% of the total variance and includes the commands and ideational praxis subtests.
Normative data for the individual A-ADAS-Cog items and adjusted total score
S.D., standard deviation; C.I., confidence interval.
Together, these three factors perfectly define the intended measures of the A-ADAS-Cog scale.
Concurrent validity
The concurrent validity was studied by comparing the adjusted scores of the A-ADAS-Cog with the adjusted scores of the A-MMSE, the CDR-Global, and the CDR-SB. The Pearson’s correlation coefficient suggested a strong and negative correlation between the A-ADAS-Cog and the A-MMSE (r = –0.86; p < 0.001). The CDR scores were also consistent with the A-ADAS-Cog scores. The correlation coefficient was 0.87 with the CDR-SB and 0.74 with the CDR-Global.
Clinical validity
To examine the discrimination power of the A-ADAS-Cog in the diagnosis of AD and NAD, we performed a ROC analysis that showed that the area under the ROC curve was equal to 0.92 (Confidence Interval = 0.87–0.97) to correctly classify AD patients and an area under the curve equal to 0.67 (Confidence Interval = 0.57–0.76) to correctly separate NAD patients from NC. Therefore, the A-ADAS-Cog has excellent discriminating power in diagnosis of AD and a poor discriminating power in diagnosis of NAD. Figure 1 describes the relationship between the sensitivity and specificity for the adjusted A-ADAS-Cog scores to separate between AD and NAD from NC.
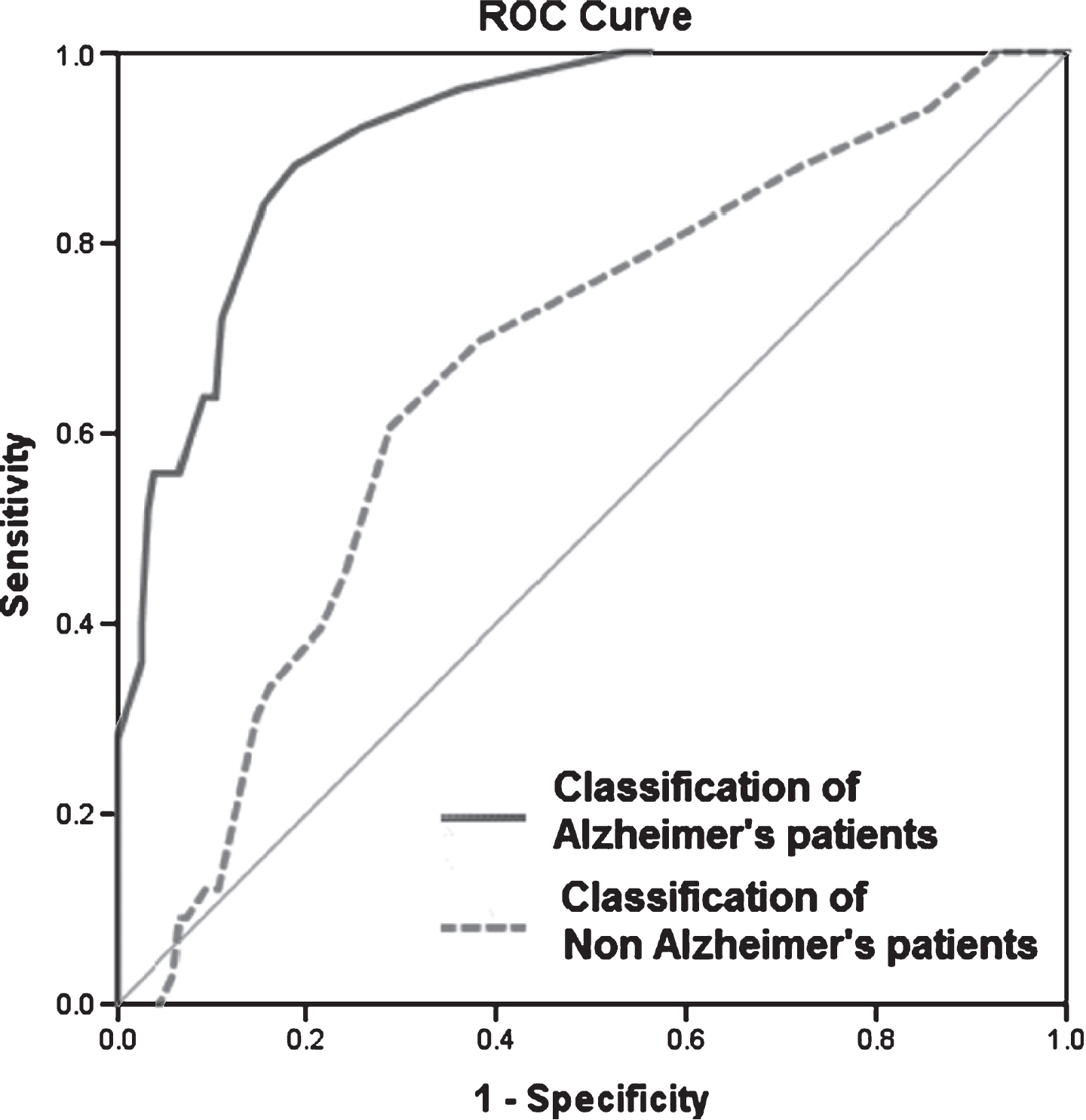
Receiver operator characteristics (ROC) curves of A-ADAS-Cog to classify Alzheimer’s and Non-Alzheimer’s from NC.
Based on ROC and diagnostic value of the different cut-offs, the most optimal cut-off point was found to be 10 and 11. A cutoff score of 11 has good sensitivity (72% ) and an excellent specificity (95% ) and a high kappa (0.28), whereas a cutoff score of 10 has good sensitivity (84% ), good specificity (91% ) and the highest kappa coefficient (0.31) showing a very good degree of concordance with the gold standard (McNemar χ2= 69.44, p < 0.001). Therefore, a cutoff score of 10 was determined to be the most useful for detection of AD.
Normative data
Once the ADAS-Cog scores were calculated and corrected using Table 2, the obtained A-ADAS-Cog adjusted to age and education scores should be interpreted based on Table 6. The latter presents normative data for the A-ADAS-Cog adjusted scores issued from the 124 elderly healthy controls constituting the HC group.
As seen in Table 6, the median score for the total adjusted A-ADAS-Cog was 5 and most of the errors on the A-ADAS-cog were made on the memory components of the scale especially word recall and word recognition. For all the other items, the median score was zero.
DISCUSSION
The ADAS-Cog is the leading tool to monitor cognitive decline during therapeutic trials of patients with AD [54]. It is also useful as an early diagnostic instrument for AD [10]. It is important for Tunisia to have tools to test, evaluate, and monitor patients with AD. Our objective in this study was to develop an appropriate, valid, and calibrated Arabic version of the ADAS-Cog for clinicians and researchers. When adapting the original ADAS-Cog, we took into account cultural factors regarding the translation of the items while still respecting and preserving the intended objectives of the various subtests, including their theoretical basis, original structure, the administration procedure, the item number, and the scoring mode for each subtest. Changes to the scale were made to improve and adjust the items to ensure understanding and automatic recognition of test stimuli to the target population as recommended by Bracken and Barona [55] and to create a sense of social and cultural familiarity with the items and the test procedure [56]. In this adaptation, we considered specific socio-cultural aspects of Arab and Tunisian individuals, particularly for word recall, naming, and recognition subtests, which are the most sensitive to cultural factors [57].
Although the A-ADAS-Cog assesses several aspects of cognition, we obtained good coefficients of internal consistency (α= 0.82 for the AD group and 0.86 for the entire study population). Coefficients ranging between 0.86 and 0.96 have been reported in the literature [19, 29].
The A-ADAS-Cog global score was stable over time, as evidenced by the test-retest reliability results. The Pearson Product Moment Correlation Coefficients was excellent for patients: (r = 0.97) for AD and (r = 0.93) for N-AD but good (r = 0.87) for NC. In the original version of the ADAS-Cog, Rosen et al. [2] reported that the correlation coefficient was 0.91 for patients with AD. In the Korean version, a correlation coefficient of 0.73 was reported for the controls, and 0.91 was observed in the AD group [58]. These results indicate the reliability of the A-ADAS-Cog test.
When comparing the global scores and the scores of the various subtests, the A-ADAS-Cog was able to distinguish between the three groups. Similar results were observed in the Slovak [12], Turkish [21], and Chinese [33] adaptations of the ADAS-Cog. The ROC analysis demonstrated that the clinical validity of the A-ADAS-Cog was excellent (area = 0.921) for diagnosis of AD. These results are similar to the results of Youn et al. [58], who observed an area under the ROC curve of 0.942. We selected two cutoff scores for the A-ADAS-Cog: 10 (sensitivity = 93% and specificity = 81%) and 11 (sensitivity = 83% and specificity = 85%). In the Youn et al. [58] study, the sensitivity was 90%, and the specificity was 82% using a cutoff score of 15/16. In the Korean version, the control group had a lower level of education than the AD patients, which is important because performance on the ADAS-Cog is negatively affected by education. In the Greek version, Tsolaki et al. [14] used a cutoff score of 13/14. In the Turkish version, the sensitivity was 90%, and the specificity of 86% using a cut-off score of 12 [21]. Our AD group had few patients with early AD (CDR-Global = 0.5), which may explain why our cut-off score (11) was lower than scores reported in the literature and suggests that this score may be useful for detecting early AD.
We established the concurrent validity of the A-ADAS-Cog with the A-MMSE and the CDR. The A-ADAS-Cog scores were negatively correlated with the A-MMSE scores (r = –0.86) and positively correlated with the CDR-SB (r = 0.87) and CDR-Global scores (r = 0.74). This strong concordance (>0.70) is in favor of the validity of our instrument. Similar results were found in other studies with correlation coefficients ranging between 0.7 and 0.9 [19, 58].
PCA performed on the AD patients grouped the 11 subtests into three factors (memory, language, and praxis), which explained 72% of the total variance. The memory factor included subtests requiring the active retention and recovery of episodic memory (word recall and remembering test instructions). It also included the naming and orientation subtests, which involve semantic and autobiographical memory and, therefore, investigate long-term memory. This factor also included the recognition subtest, which explores the storage and relatively passive recognition capacity. Finally, the memory factor included the constructional praxis subtest, which involves working memory and includes an aspect of executive function. The second factor (language) included the three subtests assessed from the interview, which involve aspects of language phrasing and reception. The spoken language subtest refers to the quality of language, its audibility, and its ability to be understood. The comprehension subtest refers to the discernment of language and the ability to find the correct word. The third factor (praxis) included the commands subtest, which assesses ideomotor praxis, and the ideational praxis subtest, which is concerned with ideational aspects of praxis. The praxis factor estimates the patient’s ability to properly perform order of operations tasks for increasingly complex gestures. This validates the rational configuration and construct of the A-ADAS-Cog compared to the original test designed by Rosen et al. [2]. To our knowledge, few studies have examined the factor structure of the ADAS-Cog, particularly in AD patients. In the Italian version, Fioravanti et al. [18] performed a factor analysis on the control group, which resulted in four factors that explained 67% of the variance; where the spoken language subtest was included in the factor structure. This suggests that the scores for the spoken language subtest showed some variance, or in a control population, speech clarity is part of the “species specific standards capacity” [59] where any deviation from the norm is pathognomonic. In our PCA of the control group, the spoken language subtest was removed because there was no variance in the scores, as is expected from a normal population.
Our results show that performance on the A-ADAS Cog was negatively affected by advancing age. This effect was not observed for the Chinese [29] or Icelandic [32] versions. However, negative effects of age have been reported for other versions, including the Italian [18] and Spanish [11, 28] versions. The effect of advancing age is typical and expected for psychometric assessments, especially because general intellectual efficiency decreases with age [60].
Zec et al. [10] and Wang et al. [33] found no negative effect of low education level on ADAS-Cog performance. However, numerous studies have suggested that education level negatively effects performance on the ADAS-Cog [18, 25–28]. In addition, Schwarb, Kobere, and Spiegel [61] noted that ADAS-Cog scores were highly correlated with general intelligence levels as assessed by the Wechsler Adult Intelligence Scale and the Raven Progressive Matrices (PM 47). Our results show a negative and significant effect of education level on the global A-ADAS-Cog score and on the orientation, word recall and constructional praxis subtests. The discrepancies among the different studies may be explained by differences in sample size, the use of extreme or close school classes and the methods used for data analysis. Prospective studies [9, 26] have shown that education level can predict the decline in ADAS-Cog performance. In addition, cross-sectional studies may not reflect longitudinal changes, especially when the subjects’ education levels are similar. We proposed that age and education level corrections should be made to the A-ADAS-Cog scores to remove the effects of age and education, which are present for neuropsychological tests. This correction will appropriately adjust the A-ADAS-Cog scores for the Tunisian population in the short- and medium-term. For example, this correction will prevent bias associated with the high illiteracy of Tunisians over 60 years old and meet the needs of a Tunisian population whose life expectancy is increasing each year [23]. In the original version and in several other versions (such as the French and Italian versions), the ADAS-Cog includes items that involve reading and graphomotor skills. In our adaptation of the ADAS-Cog, we adjusted the reading and writing components while considering the clinical and neuropsychological usefulness of their assessment.
Concerning the normative data, the median total A-ADAS-Cog score is identical to the median obtained by two different other cultures: Zec et al. [10] on 52 Chinese healthy elderly controls and Graham et al. [31] on 124 normal controls from the United States of America. The concordance of the median scores proves the equivalence of these different versions of the ADAS-Cog.
The results obtained in this study show that the A-ADAS-Cog is a reliable and valid scale that is sensitive to the specific progressive stages of AD. This study also provides normative data, which will enable the necessary corrections to the scores according to age and level of education. The A-ADAS-Cog can be used by the clinicians using the obtained normative data on the Tunisian population for early detection, evaluation, and monitoring of AD in daily clinical practice and research.