
Abstract
Background:
Subjective cognitive decline (SCD) may be a very early symptom of Alzheimer’s disease (AD) and may be associated with a cognitive decline in a cognitively normal population. The McNair and Kahn Scale was used to assess memory complaints in the GuidAge study.
Objective:
Our objectives were to examine if the McNair and Kahn Scale can predict cognitive decline and to screen which (if any) of the question(s) of this scale would better predict this cognitive decline.
Methods:
The GuidAge study was a phase III, multicenter, randomized, double blind, placebo-controlled study. Individuals aged 70 years and older, without cognitive impairment (Clinical Dementia Rate (CDR = 0)) at baseline who had spontaneously reported SCD were included in this study. The 20-item version of the McNair and Kahn Scale was used to assess SCD and a standardized neuropsychological assessment was used to assess the cognitive status.
Results:
1,307 patients with SCD and with CDR = 0 at baseline were included. During the 5 years of follow-up, 519 patients showed cognitive decline. Incidence of aggravation score of CDR was 13.40% person years (95% CI [12.24–14.56]). Results showed a significant relationship between the McNair and Kahn Scale score and decline in cognitive performance (HR 1.012; 95% CI [1.002–1.021]; p = 0.0156). Among the 20 items, 5 were statistically significant to predict cognitive decline after adjustment.
Conclusion:
SCD is a promising indicator of memory impairment. Our study found that using the McNair and Kahn scale can predict cognitive decline. A 5-item version of this scale could be used to screen patients in clinical practice and in clinical research.
Keywords
INTRODUCTION
A memory complaint, also called subjective cognitive decline (SCD), is a subjective disorder and appears to be relatively common, especially in elderly persons. The reports of its prevalence in various populations range from approximately 10% [1] to as high as 88% [2], although it is generally thought that the prevalence of everyday memory problems lie within the range of 25% to50% [3].
Memory complaints are more often unspecific. Some cognitive and non-cognitive factors may influence SCD. Depression is the most important predictive factor of cognitive complaints [4 –11], but other emotional or affective factors, such as anxiety [5 , 8], education, and physical functioning may also play a role, but results across different studies are sometimes conflicting [2 –8].
It has been suggested that SCD may be an early indication of cognitive decline at a very early stage of a neurodegenerative disease, i.e., preclinical stage of Alzheimer’s disease (AD) [13], that is undetectable by standard testing instruments [7 , 15]. SCD may represent the first symptomatic manifestation of AD in individuals with unimpaired performance on cognitive tests. However, studies on the relationship between SCD and cognitive performance have also given inconclusive results. A few cross-sectional studies have shown that SCD does not necessarily correlate with objective cognitive impairment [1 , 16–23].
Other longitudinal studies have found SCD to be associated with future AD or dementia [24 –31] and to be linked to future cognitive decline [7 , 33], one of these found that the association was only revealed in subjects with normal baseline cognition [34 –36]. On the contrary, others studies have found no association between SCD and future cognitive change [4 , 8–10] or future dementia [11].
Results of current studies on SCD are highly variable probably because: The assessment of memory complaints lacks a common standard, methods varying from simple questions [4
, 34], to visual analog scales, to specific instrumentaltests [37]. Studies populations at baseline are heterogeneous and are studied in different research environments [38, 39]. Non-cognitive factors, in particular anxiety and depression, are not always assessed. The duration of follow-up is not always sufficient to assess subsequent cognitive decline or incident dementia. Many studies use questions specifically related to episodic memory, without assessment of others cognitive domains. And, finally, there is an absence of common terminology and viable research concepts on this topic [40, 41].
Thus, an overview of the link between SCD and the rate of cognitive decline and the risk of conversion to AD dementia is missing. To address this need, the Subjective Cognitive Decline Initiative (SCD-I) was started with the aim of facilitating the development of a common SCD research concept [12]. SCD-I defined terms of pre-MCI SCD and proposed a system for coding essential features of SCD in studies. In addition, SCD-I listed specific features associated with SCD which increase the likelihood of preclinical AD (SCD plus).
The McNair and Kahn Scale or Cognitive Difficulties Scale (CDS) [13, 43] was employed to define and characterize cognitive complaints in the GuidAge study [14, 44], involving a population of more than 2800 individuals aged 70 years or older having spontaneously complained of memory problems to their general practitioner (GP). It contains items which are related to difficulties in attention, concentration, orientation, memory, praxis, domestic activities and errands, facial recognition, task efficiency, and name finding [15, 45].
It therefore provides an opportunity to thoroughly describe the cognitive functions of a large group of patients with spontaneously reported mild subjective memory loss to their GP. To our knowledge, no previous study has attempted to demonstrate a relationship between cognitive complaints in the McNair and Kahn Scale and future decline in cognitive performance in a population with Clinical Dementia Rating (CDR) of 0 (that we may consider as “normal” subjects).
In this paper, the objective is twofold: 1) to examine if the McNair and Kahn Scale global score can predict decline in cognitive performance and 2) to screen which (if any) of the question(s) in this scale would better predict this decline in a cognitively normal elderly population with self-reported memory complaints.
METHODS
Study design and participants
The GuidAge study protocol has been published previously [46, 47] and was approved by the Independent Ethics Committee of Toulouse University Hospital, Toulouse, France. To sum it up, it was a phase III, multicenter, randomized, double blind, placebo-controlled study comparing treatment with ginkgo biloba extract or placebo for 5 years, in France.
In the GuidAge study, all individuals aged 70 years or older who lived in the community and consulted one of the GPs or memory center for problems related to memory were eligible for screening. The initial screening visit was done by the GP or memory center investigators, and participants meeting the following selection criteria were retained: an identified caregiver and a Mini-Mental State Examination (MMSE) [48] score of more than 25/30, a Covi anxiety scale [16] score of less than 6/12, and a Geriatric Depression Scale (GDS 30-items) [49, 50] score of less than 15/30. The caregiver had to be available to accompany participants to memory center visits, or at least be able to be contacted by telephone to provide information about the participant for the Instrumental Activities of Daily Living (IADL) [51] and CDR assessments [52]. To determine a disability with the IADL scale, 4 items were used: ability to use phone, to use mode of transportation, to handle finances, and to be responsible for own medications.
The exclusion criteria were as follows: major objective memory impairment (Free and Cued Selective Reminding Test (FCSRT) [17] score <10th percentile for age, sex, and sociocultural level); CDR of more than 0.5; a diagnosis of dementia (according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) and National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [18] criteria); major depression (DSM-IV criteria) [19]; or generalized anxiety (DSM-IV criteria).
All participants provided written informed consent at enrollment.
Memory complaints and cognitive assessment
SCD that was spontaneously reported to family physicians, was assessed at baseline with visual analogue scales measuring memory function and impairment in everyday life (score range 0–100, with highest scores meaning worst function or most impairment) and with the McNair and Kahn Scale [20], a short self-report questionnaire assessing cognitive difficulties in everyday activities. The version of the McNair and Kahn scale used in this study contains 20 items. Subjects rate how often they have experienced the situations described in each statement during the previous month, using a 5-point scale (ranging from 0 for never to 4 for very often). The total score, which is the sum of all item responses, ranges from 0 to 80, with higher scores indicating more frequent and severe subjective cognitive difficulties.
We also assessed the age of onset of memory complaints as recommended by the SCD-I. We assessed cognitive, functional, and depressive statuses every year during 5 years with the following tests: MMSE, CDR, FCSRT, trail making test (TMT) parts A and B [21], verbal fluency (Controlled Oral Word Association Test (COWAT) and Categorical Naming Test (CNT)) [22], visual analogue scales, IADL, and GDS [23].
Statistical analyses
Two groups were used for the analysis. To define the groups, we studied only participants of the GuidAge study with CDR = 0 at baseline: Group 1 “no cognitive decline”: CDR = 0 at baseline with no aggravation during the follow-up; and Group 2 “cognitive decline”: CDR = 0 at baseline with aggravation to CDR≥0.5 during the follow-up.
We compared clinical characteristics and McNair and Kahn scale between group 1 “no cognitive decline” and group 2 “cognitive decline”.
Descriptive statistics were performed using means and standard deviations (SD) for the quantitative parameters or frequencies and percentages for the qualitative parameters. Each item of the McNair and Kahn scale was analyzed as a dichotomous (≥2 versus <2) time-constant variable to calculate the incidence (% person-year) of our event (cognitive decline) over 5 years of follow-up.
Each item of the McNair and Kahn scale and the total McNair and Kahn score was also analyzed to assess whether the McNair and Kahn scale was an independent predictor of decline in cognitive performance using a Cox proportional hazard models with hazard ratios (crude HRs and adjusted HRs) and their 95% confidence intervals (CIs). Cox models with discrete times were performed because decline in cognitive performance occurs during a period of time, not on a specific date. “Available data” means the total “n” available for each analysis.
Each Cox model was controlled for potential confounders: intervention group, gender, age, education level, COVI, and GDS. GDS score was analyzed as a time-dependent covariate (based on the last measure available before the event).
Participants were followed up to the event (onset of first cognitive decline) or the censor date (dropout or closeout visit date). Tests based on interaction with time were used to assert the proportional hazards assumption for time-constant variables. All statistical analyses were performed using SAS 9.4 software (SAS Institute, Inc., Cary, NC).
RESULTS
Baseline characteristics of the study population
Two thousand eight hundred twenty patients were enrolled in the GuidAge study. Patients with a CDR≥0.5 and patients with missing CDR at baseline were excluded. A total of 1307 patients presenting with SCD to their family physician and with CDR = 0 at baseline were included in our study (Fig. 1). Table 1 describes the characteristics of those subjects. In the study population, the mean age of patients was 75.84±4.27 years and 32.21% were male. The mean MMSE score was 28.16±1.58 and 642 patients (49.12%) received ginkgo biloba extract. The mean total McNair and Kahn scale score was 24.12±11.34. During the 5 years of follow-up, 519 patients showed decline in cognitive performance. Incidence of aggravation score of CDR was 13.40% person years (95% CI [12.24–14.56]).
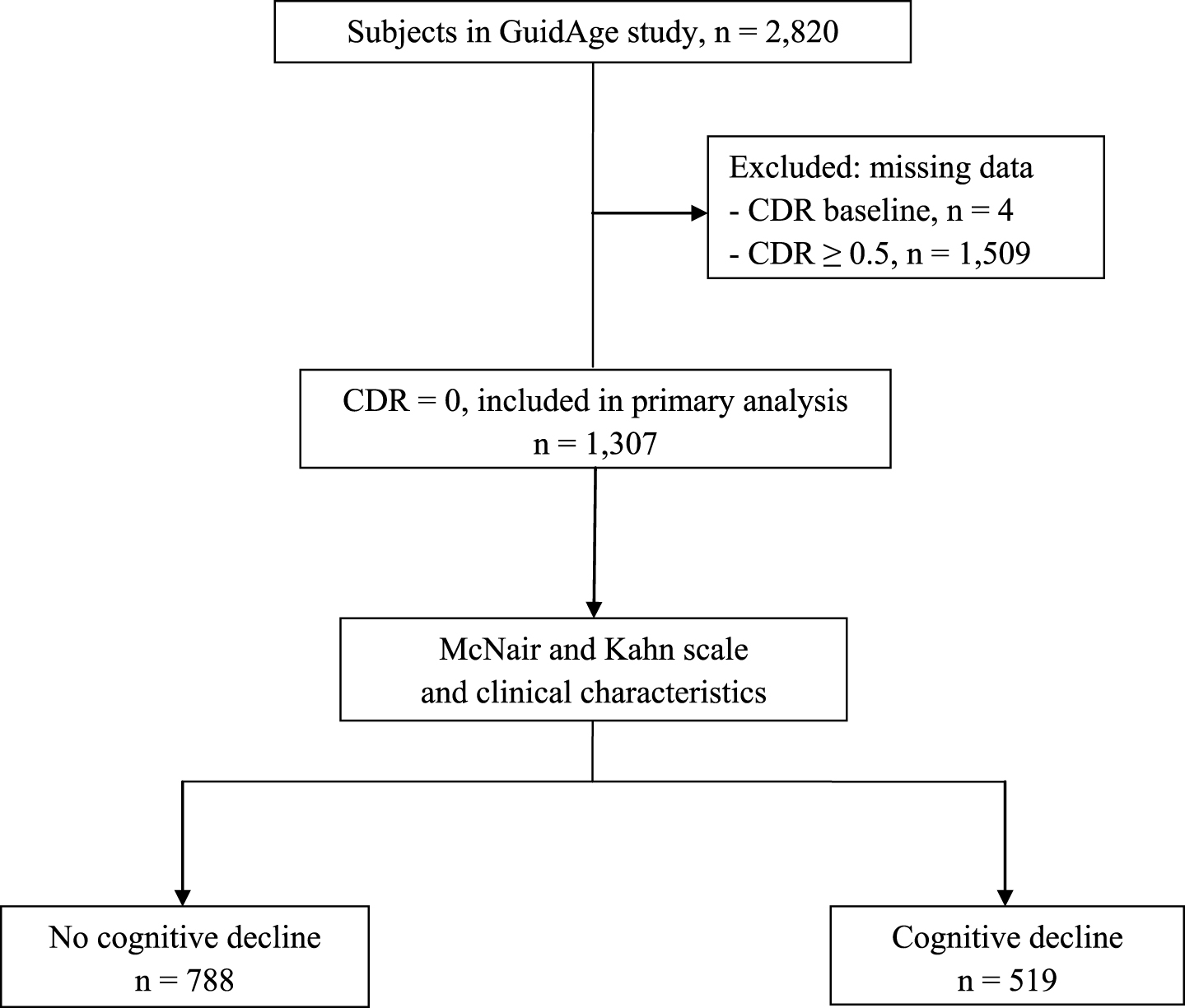
Flow chart of study. CDR, Clinical Dementia Rating.
Baseline characteristics of the study population (n = 1,307)
SD, Standard Deviation; SCD, Subjective Cognitive Decline; MMSE, Mini Mental State Examination; CDR, Clinical Dementia Rating; FCRST, Free and Cued Selective Reminding Test; TMT, Trail Making Test; COWAT, Controlled Oral Word Association Test; CNT, Categorical naming testing; Visual Analogue Scale 1, Visual Analogue Scale, memory functioning; Visual Analogue Scale 2, Visual Analogue Scale, consequences in everyday life; GDS, Geriatric Depression rating.
Sociodemographic and cognitive data
In bivariate analysis, predictors of decline in cognitive performance were age (HR 1.06; 95% CI [1.04–1.09]; p < 0.0001), history of hypertension (p < 0.0270), and diabetes (p < 0.0340). As concerns education, there is also a positive association in the population without any diploma. Depressive symptoms, as assessed by the GDS, are also significantly predictive of decline in cognitive performance (HR 1.06; 95% CI [1.03–1.08]; p < 0.0001) (Table 2).
Factors associated with decline in cognitive performance (excluding Mc Nair and Kahn scale; bivariate analysis)
CI, Confidence Interval; HR, Hazard Ratio; CDR, Clinical Dementia Rating; MMSE, Mini Mental State Examination; FCRST, Free and Cued Selective Reminding Test; TMT, Trail Making Test; COWAT, Controlled Oral Word Association Test; CNT, Categorical naming testing; Visual Analogue Scale 1, Visual Analogue Scale, memory functioning; Visual Analogue Scale 2, Visual Analogue Scale, consequences in everyday life; GDS, Geriatric Depression rating.
Incidence of decline in cognitive performance was not significantly different in placebo and intervention groups (p = 0.3019). The associations with sex and hypercholesterolemia were not significant. Our analyses also found a link between the presence of the APOE ɛ4 genotype and decline in cognitive performance (HR 1.45; 95% CI [1.13–1.86]; p = 0.0030) (Table 2).
All cognitive parameters to assess neuropsychological performances including MMSE, FCSRT, TMT, COWAT, CNT, and visual analogue scales were significantly predictive of decline in cognitive performance (p < 0.0001) (Table 2).
Primary outcome
For the primary outcome, results showed a significant relationship between the McNair and Kahn Scale global score and decline in cognitive performance (HR 1.02; 95% CI [1.01–1.03]; p = 0.0002; adjusted p = 0.0156).
Table 3 shows the relationship between 20 items of the McNair and Kahn Scale and decline in cognitive performance. There are 9 significant items in bivariate analysis.
20-item version of the McNair and Kahn Scale: association with decline in cognitive performance
CI, confidence interval; HR, hazard ratio; CDR, Clinical Dementia Rating; / *p adjusted for intervention group, gender, age, education level, COVI, GDS score.
In multivariate analyses, when results are adjusted for intervention group, gender, age, education level, COVI, and GDS score, 5 items are significant: “I hardly remember usual phone numbers”, “I forget appointment, dates, where I store things”, “I forget to call people back when they called me”, “I forget the day of the week”, “I need to have people repeat instructions several times” (Table 3).
DISCUSSION
Nowadays, it seems necessary, in both clinical research and clinical practice, to screen people at risk for developing AD at a preclinical stage. Indeed, characterization of at-risk states and detection of early disease are crucial to promote dementia prevention [53 –59]. Memory complaints could be a very early symptom appearing even before the onset of objectively detectable MCI and may represent the self-experience of subtle cognitive decline.
The results of this study suggest that the assessment of cognitive complaint spontaneously reported to primary-care physicians and as determined by the McNair and Kahn scale can predict a decline in cognitive performance, as 5 items out of 20 were statistically significant.
It is interesting to note that the items of this tool assess a variety of cognitive domains. Among those items, the predictive items for cognitive decline included the areas pertaining to memory with delayed recall (item 5 and 6) and the areas pertaining to temporal orientation (item 10).
Our results confirm those of a study carried out in 2005 by Dufouil et al. [7], which reported similar findings based on data from a large population cohort using the same scale (39-item version) to assess cognitive complaints. The authors have shown that more cognitive complaints predict faster cognitive decline in subjects with no apparent previous cognitive decline. However, in this study, the follow-up duration was only 2 years, voluntary participants were younger than our population (aged 59–71), and did not initially present SCD.
To assess cognitive complaints, some studies have used simple questions or other scales. With a similar population at baseline (participants aged 65–84 and with normal baseline cognition), one longitudinal study [34], with an average follow-up period of 3.2 years, the use of a single question could demonstrate that SCD was associated with an increase in the risk of developing AD. Other studies which used a single question showed an association with SCD and cognitive decline, incident AD or dementia, but the baseline population was not without cognitive impairment but only non-demented or free of dementia [11 , 30].
As in the GuidAge study, other studies have used scales to assess SCD and its relationship to cognitive decline. For example, Caselli et al. [60] used the Multidimensional Assessment of Neurodegenerative Symptoms (MANS) Questionnaire completed by participants and informants, comprised of 87 questions (scores ranging from 0–344, with higher scores indicating more frequent and severe symptoms). This study had subjects aged 21 to 87 years who were cognitively healthy at baseline and analyzed longitudinal trajectories of test scores between APOE subgroups (homozygotes, heterozygotes, and non APOE ɛ4 carriers). The authors showed that both self and observer-based subjective cognition changed more in APOE ɛ4 homozygotes than in APOE ɛ4 heterozygotes or noncarriers. Wang et al. [31] used a different scale: the Subjective Memory Rating Scale (SMRS), which is made up of 5 specific questions with a total score ranging from 5 to 25. For a 5-year follow-up, authors reported that SCD in cognitively normal subjects at baseline was linked to a cognitive decline (with a drop in the Cognitive Ability Screening Instrument score to 86 or lower; OR = 2.7; CI 95%, [1.45–4.98]). Moreover, this study highlighted the fact that SCD at baseline was associated with incident dementia during follow-up and that age modified this association. Indeed, for persons reporting SCD at the ages of 70, 75, and 80, the hazard ratios of developing dementia were 6.0 (95% CI [2.1–18]), 3.2 (95% CI [1.6–6.2]), and 1.6 (95% CI [0.86–3.1]), respectively. It may mean that subjective memory complaints by younger adults also are more predictive of future cognitive decline. Donovan et al. [61] used the CDR items to classify older individuals with clinically normal cognition at baseline into two groups: without SCD and with self or informant reported cognitive concerns. They found that those with a SCD diagnosis at baseline had a fourfold greater risk of progression to MCI compared to those without SCD.
All of these studies confirm our results, but their populations at baseline, unlike ours, did not have a spontaneous cognitive complaint. It is only once included that the participants are questioned in relation to their SCD. It is in this sense that our study is unique and interesting, because our recruitment is based on a spontaneous cognitive complaint reported to their GP, and our two study groups included patients with SCD.
There are several strengths in this study. One of the strengths is that the study population was made up of more than 1,300 individuals aged 70 years and older, who were free of dementia at baseline, without cognitive impairment (CDR = 0) and who had spontaneously reported subjective memory complaints to their primary-care physician. Moreover, our population included subjects who had neither anxiety nor depression. Therefore, our population at baseline respected the research criteria established by the SCD-I to define the SCD [42]. Also, according to the SCD-I, the 519 patients whose cognition declined during the follow-up, and who had an aggravation of CDR≥0.5, were probably at a pre-MCI stage. SCD of these participants is related to a probable underlying neurodegenerative disease, while the other participants who did not develop cognitive decline during the 5 years of follow-up had an isolated SCD. Some of the further strengths of our study is its multicenter design and a long follow-up period. Indeed, participants were followed-up for 5 years by primary care physicians and in expert memory centers. At each visit, the global cognitive status of each participant was assessed with the CDR and a complete and standardized neuropsychological assessment. The duration of this follow-up is much longer than other studies which only followed participants between 1 to 3 years [4 , 29].
It must also be noted that there are some potential limitations to the present study. The main limitation is the fact that our study population included participants who received standardized ginkgo biloba extract. However, this randomized placebo-controlled trial concluded that long-term use of standardized ginkgo biloba extract did not reduce risk of progression to AD compared with placebo [46]. Furthermore, the analyses were adjusted to the intervention group. Moreover, we included in this study a very specific population which can limit us in terms of generalization of the study. Another limitation lies in the fact that memory complaints were assessed at baseline but not during follow-up. However, some studies suggest that memory complaints may evolve over time. SCD may persist, disappear or appear during the follow-up and hence association between SCD and cognitive decline may also change [29, 62]. The last limitation is that there was no questioning of the informal caregiver or informants about the memory complaints of the subjects. Indeed, Gifford et al. [63] showed that among cognitively normal older adults, a combination of both self and informant cognitive complaint was associated with a four-fold risk of progression to MCI or dementia over the follow-up period. Moreover, this study showed that an informant complaint alone conferred a two-fold increased risk of progression over the follow-up period (as compared to no complaint) and a self-complaint was less predictive of conversion than the presence of both self and informant complaint.
Finally, considering the frequency of memory complaints in the elderly, it is very important for GPs, in clinical practice, to know which patients with memory complaints should be referred to a memory center to assess cognitive functions.
In order to improve this screening, a shorter scale with 5 items could be used. Among the 20 items of the McNair and Kahn scale, 5 significant items were selected to design a mini scale. These 5 items are: item 1, “I hardly remember usual phone numbers”; item 5, “I forget appointment, dates, where I store things”; item 6, “I forget to call people back when they called me”; item 10, “I forget the day of the week”; item 13, “I need to have people repeat instructions several times”.
Conclusion
The diagnosis of AD is often made at a late stage, and identifying prodromal markers which allows patients to be identified at a subclinical stage of cognitive decline has become an increasingly important matter of investigation. SCD is a promising indicator of memory impairment. Using data from a large population based cohort study of subjects followed up over 5 years and presenting spontaneous SCD to their family physician, our study has found that using the McNair and Kahn scale to assess memory complaints in a normal population without cognitive impairment can predict a decline in cognitive performance. In therapeutic trials, it is crucial to identify AD at its prodromal stage, and the McNair and Kahn scale could be a tool to screen patients and to limit screening failure rate before analysis of biomarkers. In a cognitively normal population with memory complaints, the McNair and Kahn scale allows screening of patients who probably have pre-MCI or preclinical AD. In the 20-item version of this scale, 5 items were significant and these were selected to propose a mini McNair and Kahn scale. Moreover, in clinical practice, it would be easy and quick for GPs to screen their patients with this miniscale.
Footnotes
Acknowledgments
This study was initiated and funded by IPSEN-Beaufour, manufacturer of EGb 761®. The academic authors (S. Dardenne, J. Delrieu, S. Sourdet, C. Cantet, S. Andrieu, B. Fougère, B. Vellas) have had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. They declare that they participated in the design, implementation, and interpretation of the study and that they have seen and approved the final version of the manuscript.
The industrial author (H. Mathiex-Fortunet) declares that she participated in the design, implementation, and interpretation of the study and that she has seen and approved the final version of the manuscript. She has the following conflicts of interest to declare: employment by the funding source.