
Abstract
Background:
Olfactory impairment is reported in mild cognitive impairment (MCI) and Alzheimer’s disease (AD) and is associated with hippocampal atrophy. In elderly people, dementia with AD neuropathology and white matter lesions (WML) is common. In this context, olfactory impairment could also depend on the presence of WML.
Objective:
To assess the cross-sectional relationship between olfaction and WML in elderly subjects with MCI.
Methods:
Consecutive subjects, >65 years old, diagnosed as MCI after a comprehensive neuropsychological assessment in an expert memory center, with a brain MRI performed within a year and without major depressive state, were included. Olfaction was assessed by the Brief Smell Identification Test (BSIT). Two trained neuroradiologists, blind to cognitive and olfaction status, visually assessed hippocampal atrophy according to Scheltens’ scale and WML according to Fazekas criteria.
Results:
Seventy-five MCI subjects (mean age (SD) = 77.1 (6.2) years, 74.7% of women) were included. After adjustment for age and sex, factors associated with low BSIT scores were older age (p = 0.007), lower BMI (p = 0.08), lower MMSE score (p = 0.05), lower FCRST (p = 0.008), hippocampal atrophy (p = 0.04), periventricular WML (p = 0.007), and deep WML burden (p = 0.005). In multivariate analysis, severe deep WML (OR (95% CI) = 6.29 (1.4–35.13), p = 0.02) remained associated with low BSIT score independently from hippocampal atrophy.
Conclusion:
In elderly MCI subjects, low olfactory performances are associated with WML, whose progression may be slowed by vascular treatments. A longitudinal study to evaluate whether the progression of WML, hippocampal atrophy and low olfactory function, can predict accurately conversion from MCI to dementia is ongoing.
INTRODUCTION
Alzheimer’s disease (AD) neuropathology is characterized by intraneuronal protein clusters of hyperphosphorylated tau protein (neurofibrillary tangles), extracellular amyloid-β (Aβ) protein aggregation and vascular deposition that start decades before the onset of clinical symptoms [1]. However, among elderly subjects, pure AD is rare whereas dementia with a combination of AD neuropathology and brain vascular lesions such as white matter lesions (WML) is very common [2]. Such vascular lesions worsen the cognitive impairment [3, 4].
If olfaction usually decreases with age [5–7], a growing body of evidence supports an earlier olfactory impairment in AD patients and mild cognitive impairment (MCI) subjects [8–10]. Olfactory loss has repeatedly been associated with incident MCI and AD [9, 11–14] as well as with conversion from MCI to AD [8, 15–18]. Olfactory loss is also associated with AD markers such as hippocampal atrophy and PET amyloid burden [19].
Lesions in the olfactory cortex, where phosphorylated tau protein accumulates early in the course of AD [20], could explain the association of olfaction and AD. Moreover, in transgenic AD model mice, deposition of Aβ aggregates in the olfactory pathway correlates with olfactory dysfunctions [21, 22]. However, findings on olfactory dysfunction and vascular cognitive impairment [23] are still scarce since only small sample studies found an association between vascular dementia (VaD) and lower olfactory performances [24, 25]. Olfactory impairment in elderly AD subjects could also be related to the presence of WML since olfactory dysfunction is associated with WML burden in multiple sclerosis [26, 27] and Parkinson’s disease [28].
To our knowledge, no research on olfaction and WML in subjects at risk for AD or mixed dementia suffering from MCI [29, 30] has yet been reported. Our objective was, therefore, to assess the relationship between olfactory function and WML in elderly subjects with MCI.
MATERIALS AND METHODS
Subjects
Seventy-five consecutive subjects were recruited at Broca hospital geriatric memory clinic (expert memory center) from January to June 2016. All subjects gave written informed consent for their participation in the study, which was approved by the local ethics committees on human experimentation. Inclusion criteria included age 65 years and older, French speaking, available brain MRI performed within one year, and MCI diagnosis according to the European AD Consortium [29]. Exclusion criteria were major depressive states according to DSMIV-R criteria [31], AD or other dementia [31], and subjects with a disease that could interfere with olfaction (e.g., Parkinson’s disease [32], rhinitis, etc.). All data were anonymized prior to the analysis. Demographic data, vascular risks factors: hypertension defined as self-reported diagnosis of hypertension or use of antihypertensive medications or blood pressure >140/90 mmHg, smoking status (categorized as never (less than 10 pack-years), former, or current smokers), diabetes defined as history of diabetes mellitus or use of glucose-modifying medications and dyslipidemia defined as history of dyslipidemia or use of lipid lowering medications, cardiovascular diseases (coronary heart disease, stroke, heart failure), and current medications were recorded by a physician. Body mass index (BMI) was calculated as weight in kilograms divided by the square of the height in meter. The educational level was scored as primary school, secondary school, and high school diploma and above.
Blood samples were collected for all subjects (complete blood cell count, measurement of electrolytes, serum creatinine, total cholesterol, high and low density lipoprotein-cholesterol, thyroid stimulating hormone, folate and vitamin B12, fasting blood glucose, albumin and C-Reactive Protein (CRP). For a subsample of participants (n = 47), APOE genotype was performed using TaqMan® SNP Genotyping Assays (Applied Biosystem, Courtaboeuf, France). Genotype calling was performed using the Sequence Detection Software 2.1.1 (Applied Biosystems, Courtaboeuf, France).
Cognitive function assessment
All subjects underwent comprehensive cognitive assessment performed by trained neuropsychologists [33]. The global cognitive function was assessed with the Mini-Mental State Examination (MMSE) [34]. Episodic memory was tested by the Free and Cued Selective Reminding Test (FCSRT) [35]. The FCSRT tests the ability of the subjects to recall 16 words linked to different semantic fields during three consecutive learning-recalling sessions, with and without cues. Memory impairment on free and cued selective recalling predicts AD [36]. Verbal fluency [37], executive function (Trail Making Test A and B [38] and naming [39]) were tested. Depression was screened using the Geriatric Depression Scale (GDS, scored out of 30, a score >15/30 indicating a risk of depression [40]). MCI was defined as Petersen criteria (<1.5 SD in norms in cognitive function according to age, sex, educational level) [30]. Participants were then categorized as amnestic MCI (aMCI), corresponding to an impaired FCSRT: results <1.5 SD in norms according to age and education level, French norms given by Amieva et al. [41] and cut offs proven to have a good sensitivity and specificity to predict AD according to Sarazin et al. study (17/49 for free recall, 40/48 for total recall, and below 71% for index of sensitivity of cueing) [42], and non-amnestic MCI (naMCI) subtypes (<1.5 SD in norms in other cognitive functions than episodic memory) [30].
Olfactory evaluation
Olfaction was assessed [43], during participant’s clinical evaluation at the geriatric memory clinic by the Brief Smell Identification Test (BSIT), a broadly used and validated convenient 12-item test [44]. Patients are instructed to smell each odor and to identify it between 4 forced options proposed. The score is out of 12, with higher score demonstrating better olfaction.
MRI measurements
MRI protocols included axial and coronal T1, axial and coronal T2/FLAIR, axial EG T2, and proton density/T2 in a 1.5 Tesla MR unit. Atrophy of the right and left hippocampus and deep and periventricular WML were visually assessed by two trained neuroradiologists using Scheltens [45] and Fazekas [46] scales blind to cognitive status and BSIT score. Intra- and-inter-rater reliability (expressed as Cohen’s kappa coefficients) varied 0.76–0.97 and 0.78–0.92, respectively.
Hippocampal atrophy was rated on coronal images as 0, no atrophy; 1, discrete; 2, mild; 3, moderate, and 4, severe. Because there were few subjects with Scheltens score 0 and no subjects with Scheltens score 4, hippocampal atrophy was categorized as none or discrete (Scheltens 0-1), moderate (2), and severe (3). Periventricular WML was rated as 0, no lesion; 1, “caps” or pencil-thin lining; 2, smooth “halo”; 3, irregular lesions extending into the deep white matter, and deep WML as 0, no lesion; 1, punctate foci; 2, beginning confluence of foci; and 3, large confluent areas. Because only of a very few patients had severe deep WML, moderate and severe deep WML patients were merged. Thus, deep WML were categorized as none (0, no lesion; 1, discrete and 2, moderate to severe). For the same reasons, periventricular WML were categorized in the same way (0, no lesion; 1, discrete and 2, moderate to severe).
Statistical analysis
All Statistical analyses were performed using R Software.
General characteristics of the 75 participants were analyzed in the whole sample and according to the level of deep WML and compared with Fisher’s test and Kruskal–Wallis analysis of variance for categorical and continuous variables respectively.
The sample was further dichotomized according to the median value of BSIT. General characteristics of the 75 participants were then analyzed according to the median value of BSIT and compared with χ2 or T-test and with logistic regression adjusted for age and sex.
BSIT scores were drawn according to the level of deep white matter lesions in a boxplot. The clinical significance of observed mean difference was interpreted in terms of Cohen’s d effect size, calculated as the difference in means divided by the standard deviation for the whole sample [47]. Effect size was interpreted as <0.2 = very small change, 0.2–0.5 = small change, 0.5–0.8 = moderate change, and >0.8 = large change [47, 48].
A multivariate logistic regression model was constructed and included the BSIT score above or below median value as the dependent variable and variables that were associated with BSIT scores (p < 0.15) as independent variables. However to avoid collinearity issues, neuropsychological test results, hippocampal atrophy, and MCI type were not simultaneously included in the model but only the factor most associated with BSIT score in the univariate model. Likewise, deep and periventricular white matter lesions were not entered simultaneously included in the model but in two distinct models. These models were computed again with deep WML and periventricular WML as ordinal variable coded as 0, none or discrete; 1, moderate; and 2, severe and hippocampal atrophy coded as and 0, none; 1, discrete; and 2, moderate or severe atrophy in order to account for linear relationships.
RESULTS
General, medical, and cognitive characteristics of the 75 participants (mean age (standard deviation (SD) = 77.1 (6.2), 74.7% of women) are summarized Table 1. Sixty percent of the sample received at least high school diploma, 8% had diabetes, 56.3% hypertension, 31.5% hypercholesterolemia, and 8.82% were current smokers. The mean MMSE was 27.6 (2.2)/30. MCI subtypes were, respectively, aMCI and naMCI, in 48% and 52% of the cases. APOE ɛ4 allele was present among 19.1% of the 47 tested participants.
General characteristics in the whole sample and according to the level of deep white matter lesions
*Fisher’s exact test or ANOVA. % (N), percentage (number); M (SD), mean (standard deviation); SBP, systolic blood pressure in mmHg; DBP, diastolic blood pressure in mmHg; BMI, body mass index in kg/m2; MMSE, Mini-Mental State Examination; FCSRT, Free and Cued Selective Reminding Test; MCI, mild cognitive impairment; GDS, Geriatric Depression Scale; WML, white matter lesions.
BSIT score ranged from 2 to 12 with a mean (standard deviation) of 7.57 (2.49) and a median value of 8.
Fifty-three percent had none or discrete, 32% moderate, and 15% severe hippocampal atrophy; 26.7% had no deep WML, 38.7% discrete, and 34.6% moderate or severe;15% had no periventricular WML, 37% discrete, and 48% severe periventricular WML, scored on the brain MRI. Higher deep WML burden was associated with age (p = 0.01), hippocampal atrophy (p = 0.03), and periventricular WML (p < 0.001).
Cognitive and MRI characteristics according to the median value of BSIT (≥8 and <8) are summarized Table 2. After adjustment for age and sex, factors associated with low BSIT scores were older age (p = 0.007), lower BMI (p = 0.08), lower MMSE score (p = 0.05), lower FCRST (p = 0.008), hippocampal atrophy (p = 0.04), periventricular WML (p = 0.007), and deep WML burden (p = 0.005), the latter being illustrated in Fig. 1. Effect size for moderate deep WML was 0.02 and severe deep WML compare to none or discrete deep WML was –0.63.
Subjects’ BSIT score according to their general and medical characteristics
*χ2; †Logistic regression adjusted for age and sex; ‡adjusted for sex; #adjusted for age. % (N), percentage (number); BSIT, Brief Smell Identification Test; M (SD), mean (standard deviation); BMI, body mass index in kg/m2; MMSE, Mini-Mental State Examination; FCSRT, Free and Cued Selective Reminding Test; MCI, mild cognitive impairment; GDS, Geriatric Depression Scale; WML, white matter lesions.
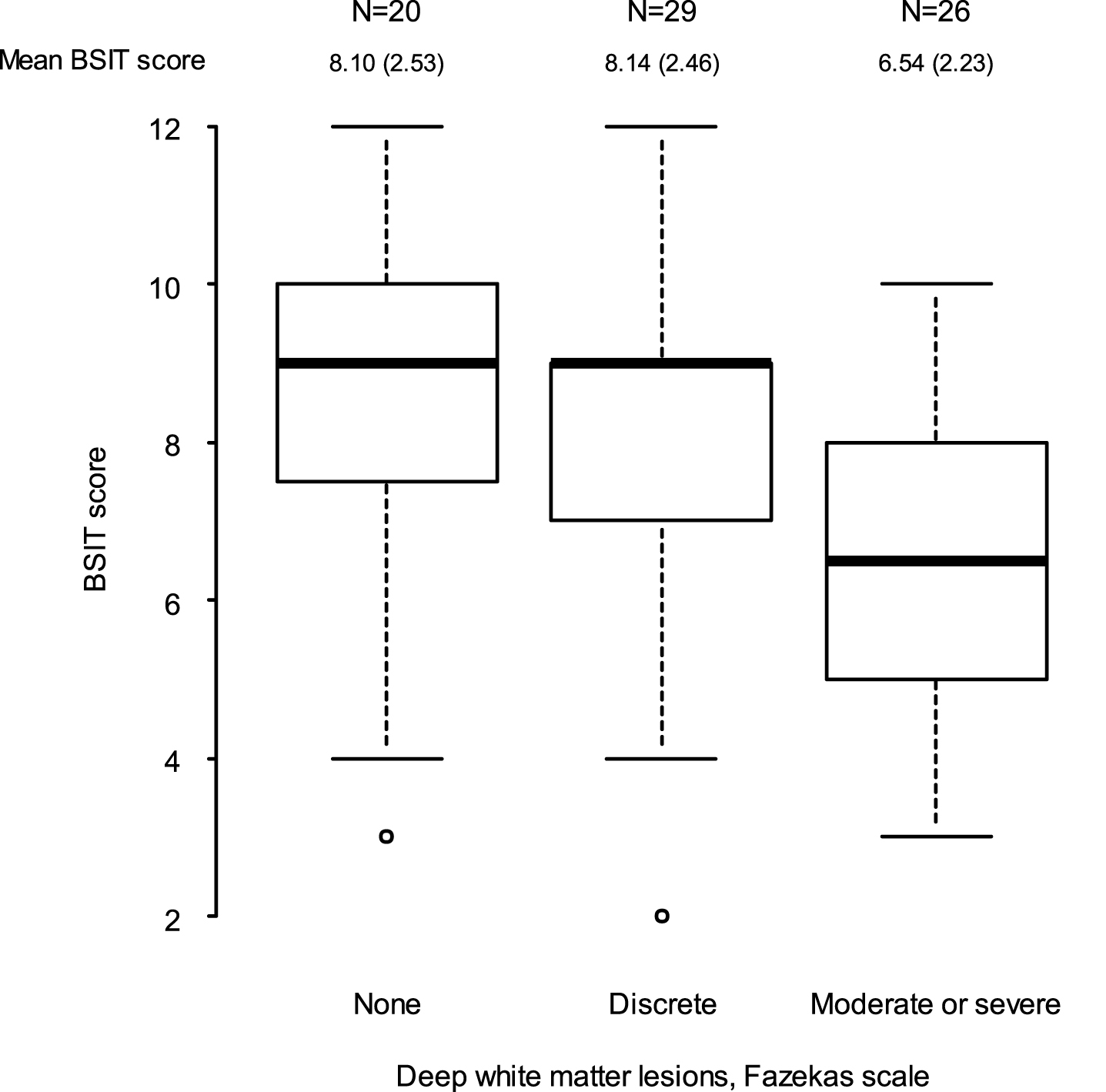
Brief Smell Identification Test scores expressed as N, mean (SD) according to the white matter lesions burden.
In a multivariate logistic regression model (Table 3) with BSIT scores <8 as dependent variable and age, BMI, hippocampal atrophy, and deep WML as independent variables, the factor independently associated with low BSIT scores was severe deep WML (OR (95% CI) = 6.29 (1.4–35.13), p = 0.02). The linear relationship between log odds of low BSIT and level of deep WML was also significant (p = 0.04). In the same model with periventricular WML adjusted for age, BMI, hippocampal atrophy, neither periventricular WML nor hippocampal atrophy were significantly associated with low BSIT. However, the linear relationship between log odds of low BSIT and level of periventricular WML was significant (p = 0.04).
Multivariate models with deep and periventricular WML
DISCUSSION
In the present study, low olfactory function in elderly MCI subjects was associated with WML independently of hippocampal atrophy.
As already reported, in univariate analysis a lower olfaction was associated with older age [5–7, 43] and poorer cognition [49, 50]. Lower olfaction was not associated with male gender as described in previous studies [43, 51] probably because the low number of males included. Lower olfaction was also marginally associated with lower BMI perhaps because weight loss can be the result of cognitive impairment [52].
In the present study, low olfactory performances were significantly associated with hippocampal atrophy in univariate analyses. Impaired olfaction has been associated with a lower hippocampal volume and a thinner entorhinal cortex in cognitively normal elderly subjects [19]. In AD, which is characterized by hippocampal atrophy, olfactory impairments have also been reported in cross-sectional [25, 43] and longitudinal studies [53]. In MCI patients, low olfactory performances predict conversion to AD [17] and cross-sectional and longitudinal studies indicated that an amnestic MCI, more predictive of AD than naMCI [30], is significantly associated with poorer olfaction [8, 9].
In the present study, elderly MCI participants with higher level of periventricular and deep WML exhibited lower olfactory performances independently of hippocampal atrophy. Unfortunately, in the aforementioned studies the relationship of AD and dementia and low olfactory performances was not controlled for the presence of white matter lesions load.
WML contribute to cognitive impairment in VaD [23] but also in AD in which WML prevalence is high. To date, only a few studies examined the relationships between olfactory impairment and VaD.
In a small study, using the Pocket Smell Test, a three-item screening measure of olfaction, AD patients (n = 20) performed worse than VaD patients (n = 20) or patients suffering from major depressive states (n = 20), even after adjusting for MMSE scores [25]. In another small sample study, another olfactory test [43] did not discriminate between AD and VaD but both groups had significantly lower scores than controls [24]. In these studies, brain vascular damage locations as well as WML were not investigated. Moreover, the association between WML and olfactory function has not been studied in the field of MCI with regard to hippocampal atrophy as measured by MRI. Conversely, association of low olfactory performances and WML has already been reported in multiple sclerosis patients [26, 27] and in early stages of Parkinson’s disease [28]. In the later, low olfaction could be related to microstructural alterations in the white matter of the central olfactory system [54]. The association between WML and olfaction could also be explained by impaired information processing between the olfactory bulb, olfactory cortex, and frontal cortex areas due to white matter alterations [28].
In the present study, deep WML were more strongly associated with lower olfaction than periventricular WML as also found in Parkinson’s disease [28]. One may hypothesize that deep WML have a greater impact than periventricular WML on olfactory circuits that extend in the deep white matter region, from the primary olfactory cortex to the orbitofrontal or prefrontal cortex [55]. Furthermore, deep WML could reflect a more severe small vessels disease as compared to periventricular WML [56].
The present study has some limitations. First, its cross-sectional design precludes drawing causal inference. Second, the sample size was small, the power was therefore limited, and it was not feasible to apply adjacent categories logit model. Third, only a semi-quantitative evaluation of hippocampal atrophy and WML was performed, and no volumetric assessment was provided. Fourth, APOE genotype was only provided in 60% of the patients. Fifth, the 12 items BSIT is a shorter (and more convenient) version of the gold standard olfactory test, the University of Pennsylvania Smell Identification test (UPSIT) which comprises 40 odorants and, even though validated [57], BSIT is less sensitive than UPSIT in detecting subtle alterations in smell function [43]. Lastly, odor intensity and pleasantness were not taken into account with BSIT testing, despite their reported impairment in AD [58].
Despite that, to our knowledge, the present study is the first to demonstrate an association between poor olfaction and WML in MCI patients with many potential confounding factors taken into account, as in a recent longitudinal study [53]. Finally, the BSIT is reliable and very easy to administer even in elderly people, and could be added in the battery to detect early cognitive impairment.
Conclusion
In MCI elderly subjects, low olfactory performances were associated with WML independently of hippocampal atrophy. A longitudinal study is currently ongoing to evaluate if olfactory impairment can predict conversion from MCI to AD or improve the value of WML and hippocampal atrophy to predict conversion from MCI to AD. WML are of particular clinical interest since they may be prevented and their progression may be delayed by vascular risk factors treatments (diabetes treatment and anti-hypertensive therapies, in particular).
Footnotes
ACKNOWLEDGMENTS
This study was supported by INSERM, “Université Sorbonne Paris Cité dynamique du vieillir” programme and ANR Research Grant (ANR-10-MALZ-003-01 SOMADOLF). The authors thank Mrs Maria Rego-Lopes and nurses at the Broca memory clinic for their help in data collection.
Ethics approval was provided by the local Committee.