
Abstract
Background:
Among non-pharmacological therapies, musical intervention is often used for patients with Alzheimer’s disease (AD) and patients presenting chronic pain. However, their efficacy is still under debate.
Objective:
Our aim was to determine the efficacy of choral singing versus painting sessions on chronic pain, mood, quality of life, and cognition in AD patients.
Methods:
In this multicenter randomized controlled trial, 59 mild AD patients were randomized to a 12-week singing (SG; n = 31) or painting group (PG; n = 28). Chronic pain, anxiety, depression, and quality of life were assessed before, after, and 1 month after the sessions. Cognitive abilities were assessed before and after interventions. The evolution of these different measures was assessed with mixed linear models. The primary data analysis was by intention-to-treat, and completed by a ‘per protocol’ approach.
Results:
Both singing and painting interventions led to significant pain reduction (Time effect: F = 4.71; p = 0.01), reduced anxiety (Time effect: F = 10.74; p < 0.0001), improved Quality of Life (Time effect: F = 6.79; p = 0.002), improved digit span (F = 12.93; p = 0.001), and inhibitory processes (Time effect: F = 4.93; p = 0.03). Depression was reduced over time in PG only (Time x Group effect: F = 4.53; p = 0.01). Verbal Memory performance remained stable over time in SG, but decreased in PG (Time x group effect: F = 9.29; p = 0.004).
Conclusion:
Findings suggest that singing and painting interventions may reduce pain and improve mood, quality of life, and cognition in patients with mild AD, with differential effects of painting for depression and singing for memory performance.
INTRODUCTION
Alzheimer’s disease (AD) principally concerns patients 65 years and older [1], with two-thirds of the patients being aged 75 years and older [2]. Patients with AD often present multiple comorbidities that can induce chronic pain [3]. At an early stage, cognitive decline is often accompanied by mood disorders [4, 5]. Medications prescribed in the management of chronic pain and mood disorders are not free of side effects. They may increase the risk of confusion, falls, and also cognitive decline. Finally, they can induce a physical and psychological dependence and difficulties to withdraw them [6].
Non-pharmacological therapies can be an interesting complementary care strategy for pain and mood disorders in these patients. Among these therapies, musical intervention (MI) is often used both in AD patients with dementia [7] and in patients with chronic pain [8, 9]. Indeed, the abilities to perceive music and recognizing familiar excerpts or musical emotions were demonstrated to be preserved in AD, even in advanced stages [10, 11]. Therefore, MI is often used in therapeutic approaches aiming to enhance cognitive functioning, as well as mood, behavioral disorders, and quality of life.
Previous studies revealed beneficial effects of MI on cognitive functioning in patients with AD or associated disorders, in particular improved global cognitive functioning [12], autobiographic memory [13, 14], implicit memory [15, 16], and verbal memory [17, 18] as well as attention and executive functions [12 , 20]. One potential hypothesis of the efficiency of MI might be linked to the observation that cerebral areas involved in music memory were reported to be spared in AD [21 –23].
In addition to improved cognitive functions, MI has been reported to decrease behavioral disorders in patients with dementia [24]. Agitation and global behavioral disorders were reduced by MI in nursing-home residents [25]. A reduction of anxiety [26, 27] with MI was observed in patients with dementia [28], and music can also reduce depressive symptoms [19 , 29]. However, the effect of MI on anxiety and depression have essentially been studied in the moderate or severe dementia stages, and very few studies have been done on patients with mild AD [28], whereas mood disorders are frequently observed after diagnosis announcement. Moreover, AD patients often develop a reduction of self-esteem at this stage. In healthy older adults, regular musical activities such as singing or instrument playing can contribute to positive aging by increasing emotional well-being, and reducing social isolation [30, 31]. Concerning patients, a study including patients with cancer reflected that performing at a final concert after singing intervention increased self-esteem and confidence [32].
Even though the findings rather sound encouraging, there are a several methodological weaknesses in a number of the previously published studies reporting the role of MI on mood disorders, cognitive impairment, or quality of life [33, 34]. Indeed, most of these studies included heterogeneous groups of patients, notably regarding dementia stage and etiology. In addition, most of the control groups only received standard care, thus not providing information about the specific impact of MI in comparison to other non-drug interventions. Furthermore, the majority of studies failed to randomize the subjects, and the assessment was not made by blinded evaluators. The evidence for the specific efficacy of MI in dementia remains therefore questionable [14]. Well-designed and well-conducted randomized, controlled trials (RCTs) provide the best evidence for the efficacy of non-pharmacological treatments [35]. To our knowledge, no previous study including AD patients at mild stage has directly assessed the effect of MI versus a comparable non-musical intervention using a RCT design.
Several previous papers thus assessed the role of MI on mood disorders in dementia. However, no study has examined the efficacy of MI on physical pain in AD patients, although common mechanisms have been identified between psychological and physical pain. Recent neuroimaging studies highlighted common neuronal networks between these two pain matrix [36]. Depression is frequently observed in patients suffering from chronic pain, and, inversely, depressed patients are at higher risk to develop chronic pain. Moreover, antidepressant drugs are prescribed for both depression and chronic pain [37]. Furthermore, some previously reported findings suggest that MI reduces chronic pain in different populations. Indeed, listening to music activates different regions in the brain that participate in the reward-response system and modulate the dopaminergic system underlying pleasure [38]. A recent RCT study using Naltrexone, which is one of the blocking endogenous opioids, demonstrated that these neuromodulators are critical to experiencing emotions in music [39]. This effect could reduce stress, anxiety, and depression, but also pain and support a better overall functioning. Several studies revealed that receptive MI, by inducing relaxation, could decrease neuropathic pain [40], fibromyalgia [41], rheumatic pain [42], or chronic lombalgia [43]. A few studies testing the elderly have demonstrated a reduction of pain with receptive MI in patients with rheumatic pain [44] or terminally ill patients [45].
Finally, assessing chronic pain in AD patients would be interesting as numerous recent researches have highlighted links between cognition and chronic pain. Cole et al. [46] found that AD patients had a lower pain threshold, a sustained reaction to nociceptive stimulus and a more prolonged pain-related activity than controls. Linked to these behavioral measures, functional MRI differences were observed in cognitive and emotional network such as the anterior cingular cortex, insula and dorsolateral prefrontal cortex, involved in emotion evaluation and regulation [46]. These results support the notion that limited cognitive abilities present in AD, may favor pain chronicity.
The present study aimed at assessing the efficacy of MI on chronic pain in patients with AD at minor cognitive disorder or mild major cognitive disorder stage, using a RCT. The secondary objectives were to measure the effectiveness of MI on anxiety, depression, quality of life, self-esteem, and cognition on this population. Among MI, a singing intervention (SI) was chosen in our study: indeed, this practice can, through the body resonance, promote the increase of endorphin production [40], which is involved in the process of pain modulation and play a significant role in inhibiting pain perception [47]. Moreover, SI has demonstrated benefits on cognitive function in previous studies on AD [19]: singing requires the intervention of many processes such as short-term memory, long-term planning control of errors, and engages several brain areas of the prefrontal cortex. Finally, singing enhances group cohesion and allows the possibility of a final concert, which is particularly interesting for improving self-esteem.
As a control intervention, group painting intervention was selected as it is similar to choral MI in several points: both activities are pleasant artistic and leisure activities, they can be performed in a group setting, and a final project (concert and exhibition) can be organized at the end of the sessions.
PATIENTS AND METHODS
Study design
The LACMé study was a multicenter RCT with two parallel arms and a blinded endpoint evaluation. The study was approved by Saint Etienne University ethics committee, and conducted in accordance with the Declaration of Helsinki and ICH (International Conference on Harmonisation) recommendations, Guideline for Good Clinical Practice. This trial was registered at clinicaltrials.gov (Identifier: NCT02670993).
Participants
Participants were recruited from 3 memory clinics located in University Hospitals from Saint Etienne (neurology and geriatrics units) and Lyon (geriatrics unit), France.
Inclusion criteria
All participants recruited for the study met the following inclusion criteria: 60 years and older and probable AD at minor cognitive disorder or mild major cognitive disorder stage, according to Diagnostic and Statistical Manual of Mental Disorders-V [48] and National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS/ADRDA) criteria [49]. The severity of cognitive disorders was assessed with the Mini-Mental State Examination (MMSE), and only participants with a MMSE superior or equal to 20 were included. The included patients also presented chronic pain, assessed with Simple Visual Scale (SVS) [50], at moderate or severe stage (score superior or equal to 2/4 since more than 1 month) and were able to complete the clinical and neuropsychological evaluations. Psychotropic drugs, acetylcholinesterase inhibitors, or memantine had to be stabilized for more than 3 months, and pain medication for at least 1 month.
Exclusion criteria
Exclusion criteria concerned patients with a neurocognitive disorder etiology different from AD, with serious, progressive, or unstable pathologies which could interfere with the variables under consideration or patients under guardianship.
Measures
Baseline evaluations were made after obtaining participants inform consent (T1). The patients underwent an extensive assessment including inclusion and exclusion criteria, AD diagnosis and stage, chronic pain, demographic and lifestyle factors, former musical and artistic practice, mood disorders, quality of life, self-esteem, and neuropsychological performance. The outcome measures are detailed below.
Concerning follow-up measures, chronic pain, mood disorders, quality of life, and self-esteem were evaluated at 12- and 16-week follow-up (T2, T3). The neuropsychological battery was assessed at 12-week follow-up.
Primary outcome measures
Chronic pain was assessed with three different measures, including the Numeric Rating Scale (NRS) [51], the SVS [50], and the Brief Pain Inventory (BPI) [52].
In the NRS, the participant selects a number from 0 to 10 that best indicates usual pain level for the past week (with 0 indicating no pain, and 10 the most severe pain one can imagine) (NRS-U). The most intense pain perceived during the 8 last days was then evaluated according to a “worst pain” score on a 0-to-10 scale, varying from 0 (no pain) to 10 (the most severe pain one can imagine) (NRS-I).
In the SVS, the patients are asked to use a categorical scale varying from 0 to 4, with 0 indicating no pain, and 4 indicating very intense pain. As in the NRS, the patients were asked to assess successively usual pain from the 8 last days (SVS-U) and the most intense pain from the 8 last days (SVS-I). These scales were validated in populations of patients with mild cognitive disorders [53].
The BPI measures the intensity of pain (sensory dimension) and interference of pain in the patient’s life (reactive dimension), thanks to numerical rating scales from 0–10. Only the reactive dimension from a short-form of the questionnaire was used in the present study. This dimension assessed pain consequences in general activity, mood, will to live, ability to walk, work, relations with other people, sleep, personal care, and recreational and social activities. The BPI is a widely used, well-standardized instrument for evaluating multiple dimensions of pain. It was validated in various populations and languages [52 , 55].
Secondary outcome measures
Anxiety was measured with the State Trait Anxiety Inventory (STAI). The STAI consists of two subscales: “state anxiety” (STAI-S), assessing a transitory emotional response to a stressful situation, and “trait anxiety” (STAI-T), assessing a general long-standing disposition to respond to stress with elevated anxiety. Each subscale comprises 20 items rated from 1 (lowest anxiety level) to 4 (highest anxiety level). Scores are summed over subscales (leading to scores from 20 to 80), with higher scores indicating greater anxiety [56]. The STAI total score, summing STAI-S and STAI-T scores, was used in our analysis.
Depressive symptoms were assessed with the Geriatric Depression Scale (GDS), which has been validated in elderly subjects. This 30-item scale has proved its usefulness in detecting depressive symptoms in patients presenting mild dementia [57].
Quality of life and self-esteem. The EuroQol-5 dimensions (EQ-5D) health survey is a measurement tool for health-related quality of life that is widely used in elderly patients with cognitive impairment [58]. The EQ-5D comprises five dimensions or items assessing current health state, notably inquiring about mobility, self-care, everyday-life activities, pain/discomfort, and anxiety/depression, graded into three levels (level 1 = no problem; level 2 = some/moderate problem; and level 3 = strong problem).
The Rosenberg Self-Esteem Scale consists of 10 Likert-type items, for example, “I feel that I am a person of worth, at least I am equal to others” with four alternatives for answers: “1 strongly agree, 2 agree, 3 disagree, 4 strongly disagree” [47]. A measure of self-esteem is obtained by summing up the scores obtained in the scale’s items, after recoding five items with reverse scores. The sum of these scores can range from 10 to 40; higher scores indicating higher self-esteem.
Neuropsychological performance. A complete battery of neuropsychological tests was used. Verbal episodic memory was explored with the 16-item Free and Cued Recall Test (FCRT) [59]. The Trail Making Test (TMT) [60] assessed speed of information-processing and mental flexibility. Digit Symbol test and Digit Span assessed working memory [61] and the Stroop test [62], assessed speed of information-processing and inhibition. Letter and Category Fluency tests [63] assessed mental flexibility and verbal fluency. The Frontal Assessment Battery (FAB) assessed Cognitive dysexecutive syndrome [64].
Randomization
All participants provided written inform consent. To ensure equal distribution between treatment groups, the randomization was made by a team member who had no contact with the patients. In each center (Lyon, Saint Etienne, see above), consented subjects were randomly assigned to a SI or a PI group with a 1:1 ratio.
Blinding
All principal outcome measures were assessed by an independent neuropsychologist in each center, who was different from the practitioner conducting SI or PI. The database and the statistical analysis were made by research team members. Both the neuropsychologist and the research team members were blind to the intervention type.
Intervention Conditions
The patients participated in 12 weekly two-hour SI or PI sessions during 3 months.
SI groups
The SI was delivered by a professional choir conductor accompanied by a psychologist, whose role was to help the conductor to manage the patients if necessary (in particular welcome, departure and possible difficulties with patients during the sessions). Before the intervention, the patients assigned to SI groups were asked to fulfill a questionnaire collecting their musical preferences among several songs. The choir conductor selected the songs according to the patients’ preferences.
Structure of an intervention session: after a personalized welcome, the patients performed a body and voice warm-up before song learning. Four different songs previously chosen by the patients among a list of well-known songs were practiced across the different sessions. The songs were then worked by the patients with piano accompaniment made by the choir conductor. A concert gathering the patient choir and a choir of young singers was organized after the SI sessions. It was attended by patients’ and young singers’ families and patients’ care team.
PI groups
The PI was done by a painting teacher accompanied by a psychologist. After a personalized welcome in the first part of each session, paintings of professional painters were shown to the patients, generating discussions across the group. The second part of the session was devoted to the patients’ painting realization according to a predetermined theme. An exhibition was organized after the PI sessions in the presence of patients’ families and care team.
Sample size
Sample size was computed according to predictions related to the NRS score, corresponding to the main objective measure. With the hypothesis of reduction of 1 point (SD 1.3) on the NRS scale, the sample size was 27 patients per group, and a total of 54 patients (with a 80 % power and an alpha risk of 5%) [43]. With an expected rate of 10% of patients lost to follow-up at the post-intervention testing sessions, the minimal number of patients to be included in the study was 60.
Statistical analyses
The primary data analysis was by intention-to-treat (ITT), carried out using multiple imputation dataset, with full analysis of all patients as randomized and completing the baseline assessment. The analysis was then completed by a ‘per protocol’ (PP) approach conducted on the patients who completed at least 6 SI or PI sessions, representing the ‘treatment maintenance’ sample, and reflecting usual clinical practice for AD patients participating to group interventions [27]. This analysis is presented for primary outcome measures (NRS, SVS, and BPI scores). For all participants, a descriptive analysis was performed on all study variables using tendency and dispersion measures for quantitative variables and relative and absolute frequencies for qualitative variables. For quantitative variables, baseline characteristics were compared between the two participant groups with Student t-tests for the analysis of normally distributed variables, and Mann-Whitney test for non-normally distributed ones. The χ 2 test was used for analyzing categorical data. The evolution of pain, anxiety, depression, quality of life, self-esteem and neuropsychological assessment scales were compared between the SG and the PG using mixed-effects models including time as a fixed effect and subject as a random effect. The different scales were tested using a multiple degree of freedom comparison of scores. Pearson’s partial correlations according to intervention group were then computed between the evolution of pain, anxiety, depression, quality of life, and self-esteem scales before and after the interventions.
All statistical tests were two-tailed. A p value <0.05 was considered significant. Statistical analyses were performed with SPSS version 17 (SPSS Software, Chicago, USA).
RESULTS
Baseline characteristics
Of the 77 patients selected for the study, 12 dropped-out of the study before randomization and 65 were randomized. Among them, 22 were recruited in Saint Etienne neurology unit (center 1, 11 assigned in the SG and 11 in the PG), 21 in Saint Etienne Geriatrics unit (center 2, 11 assigned in the SG and 10 in the PG) and 22 in Lyon geriatrics unit (center 3, 11 assigned in the SG and 11 in the PG). Six subjects withdrew after randomization. A total of 59 patients completed the baseline evaluation, among them 31 belonged to the SG and 28 to the PG. Fifty-two participants completed the second (T2) evaluation, and 50 completed the third (T3) assessment. The study flow chart is shown in Fig. 1.
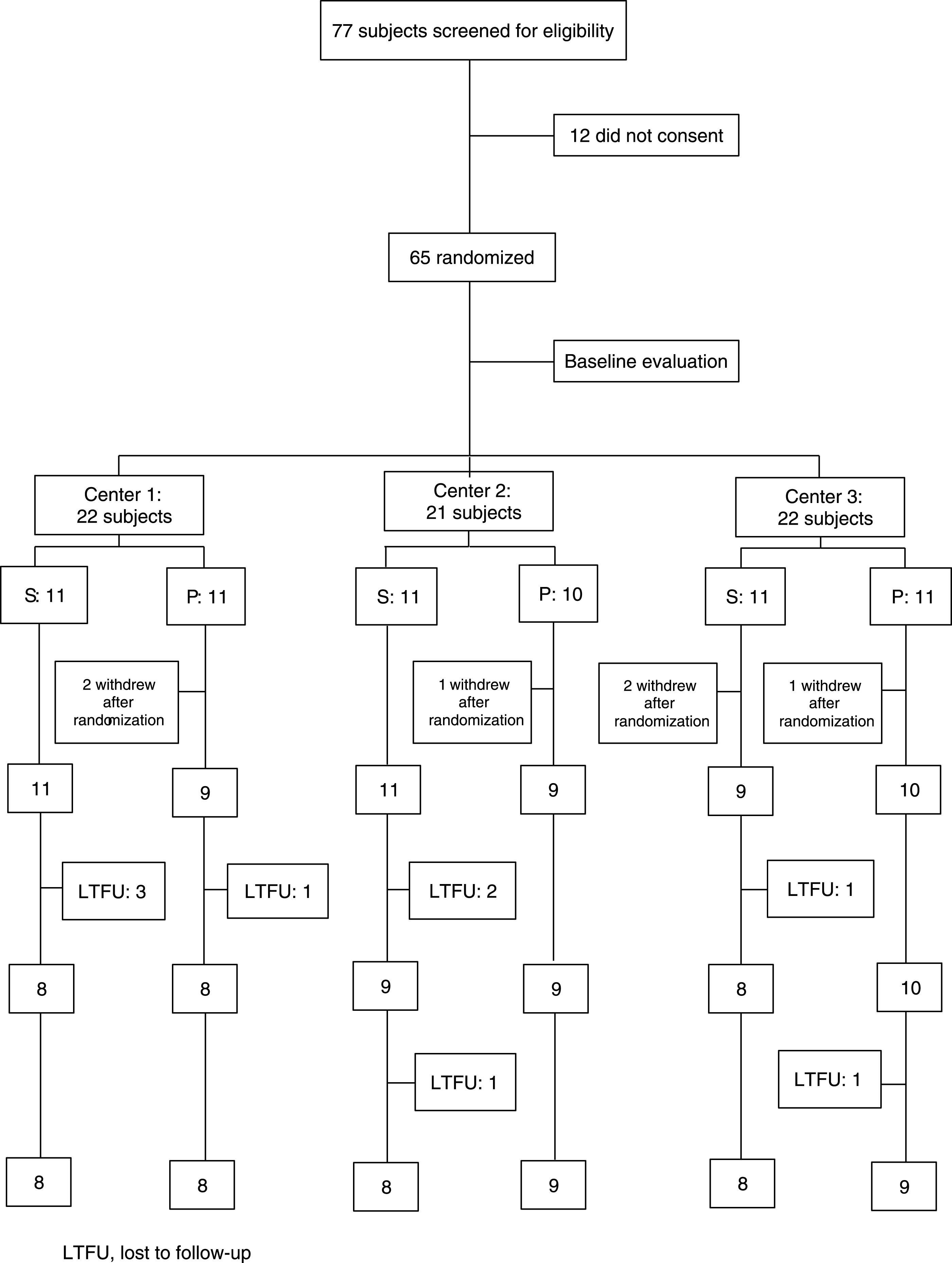
Flow chart of the LACMé study.
The demographic and clinical characteristics of the samples are summarized in Table 1. No statistically significant differences were observed between SG and PG with regard to demographic characteristics, disease severity or artistic background. No differences between the two groups were observed in outcome measures at baseline.
Patients’ baseline characteristics
*χ 2 test for qualitative variables and t test or Mann-Whitney test for quantitative variables.
Concerning interventions participation, the mean number of sessions attended by the patients was 6.4 (SD 4.3) for SG and 7.7 (SD 4.0) for PG. No significant difference was observed between the two groups (t = –1.19, p = 0.24).
Pain assessment
Table 2 shows the results of ITT and PP analyses for the primary outcome measures of pain, including means and standard deviations for pain scales at different follow-ups and the results of the mixed model adjusted on age, sex, and educational level. For ITT analysis, the mean SVS score significantly decreased over time in both SG and PG from baseline until week 16 (p = 0.01). Similarly, BPI score was significantly reduced on both conditions from baseline to 16-week assessment (p = 0.009). However, there was no interaction time by group in these two analyses. Moreover, NRS-I was also reduced in both groups between pre and post (16 weeks) testing, but the decrease just failed to reach significance (p = 0.057) and there was no interaction time by group (p = 0.86). No difference between SI and PI or over time was observed for NRS-U or SVS-I.
Comparison of SG and PG on primary outcome measures – Intention-to-treat (ITT) (n = 59) and Per Protocol (PP) (n = 40) analysis – Linear mixed effect model adjusted on age, sex, and education
The PP analysis based on the number of participants who attended at least 6 intervention sessions showed a stronger time effect for SVS-U (p < 0.00001) and BPI (p = 0.001). Moreover, a decrease of NRS-I was observed over time (p = 0.007), as well as a trend toward reduction in SVS-I over time (p = 0.057). However, for NRS-I and SVS-I, the interaction between time and group were not significant (p = 0.85 and 0.86 respectively).
Table 3 shows the results of the ITT analyses including means and standard deviations for the mood, quality of life, self-esteem and neuropsychological scores and the results of the mixed model adjusted for sex, age, and education.
Comparison of SG and PG on secondary outcome measures – Intention-to-treat (ITT) analysis – Linear mixed effect model adjusted on age, sex and education. N = 59 patients
(1)I Indice, interference indice; (2)I errors, interference errors.
Mood, quality of life, and self-esteem
The mean depressive symptoms assessed with GDS scale improved significantly over time for PI only (interaction Time×Group: p = 0.01). A significant decrease of anxiety over time (pre/post intervention) was observed on STAI scale in both groups (Time: p < 0.0001), with a stronger effect of PI. The time×group interaction was near to significance (Time×Group: p = 0.06). Quality of life measured by EQ5-D was improved in both SI and PI groups after intervention (Time: p = 0.002). However, there was no significant time by group interaction (Time×Group: p = 0.60). Finally, self-esteem assessed with the Rosenberg scale was improved over time in the two groups but this effect did not reach statistical significance (Time: p = 0.078).
Correlations between pain, anxiety, depression, quality of life, and self-esteem scales
Correlation analyses were made between the evolution of NRS-I, SVS-U, and BPI scales with GDS, STAI, and Rosenberg scales. Significant positive correlations were observed between NRS-U and EQ5D evolution (r = 0.29, p = 0.03), and BPI and EQ5D evolution (r = 0.41, p = 0.002). Conversely, no significant relationship between the pain scales and anxiety, depression, or self-esteem scales evolution was observed.
Neuropsychological scores
Concerning verbal memory, FCRT total recall was stable over time for SI, and decreased for PI (Time: p = 0.001 and Time x Group: p = 0.03). A similar result was observed for FCRT free recall (Time: p = 0.035) and FCRT delayed total recall (Time: 0.005), with the interactions Time x Group just failing to reach statistical significance (respectively p = 0.08 and p = 0.08). Moreover, the Digit Span score was improved over time in both SI and PI (Time: p = 0.001) but there was no specific group effect (Time×Group: p = 0.32). Likewise, Stroop interference errors decreased after interventions (Time: p = 0.03), with a more important but non-significant effect of SI (Time x Group: p = 0.19). We failed to find significant differences over time in the other neuropsychological performances.
DISCUSSION
This multicenter, randomized clinical trial assessed the efficacy of SI versus PI on pain, mood disorders, quality of life, self-esteem, and cognition in AD patients at minor neurocognitive disorder or mild major neurocognitive disorder stage. Patients assigned to both SI or PI showed significant improvement in most of these different domains. A significant decrease of pain over time was observed for both interventions, as reflected in several pain measures (in ITT and PP analyses). However, for pain scales, these improvements did not differ between SI and PI groups. A time effect for both groups was also observed for anxiety, quality of life and self-esteem, that is anxiety decreased and quality of life and self-esteem increase post-intervention. In addition, the study showed a reduction of depressive symptoms with PI in comparison to SI. Furthermore, we found a benefit of SI in verbal memory in comparison to PI. Finally, some neuropsychological scores including working memory were improved over time, without between group differences.
Pain
LACMé is the first study to assess the efficacy of SI versus PI on pain in AD patients. Several chronic pain measures revealed reduced pain after intervention (in comparison to before intervention) for both SI and PI. Some previous studies have assessed the efficacy of MI on chronic pain with RCT methods. The majority of them concerned younger adults, and they used relaxing music listening. They showed a short-term [42, 43] or persistent [9] effect of music therapy on Visual Analogic Scale compared to a group without intervention or a group exposed to unpleasant noise [41]. Among studies focused on elderly patients [44], reported decreasing pain scores on both the Pain Descriptor Scale and the VAS over a 14-day period in patients with osteoarthritis. Three measures were made at day 1, 7, and 14, immediately before and after listening to 20 min of relaxing music compared to patients without intervention. However, they did not measure the long-term efficacy of music listening intervention, and music listening was not compared to another pleasurable activity [44].
Concerning PI, to our knowledge no previous study investigated the role of painting intervention on chronic pain.
Our study was the first to assess the interest to use art interventions in the management of pain in AD patients. The reduction of chronic pain highlighted by our results encourages the development of these non-drug therapies.
Mood, quality of life, and self-esteem
Our results revealed a greater decreasing of anxiety and depressive symptoms for PI than SI. Previous research has provided mixed evidence concerning a potential specificity of MI on symptoms in AD. In a previous study, Cooke et al. [27] observed an absence of effect of singing or playing an instrument on depression in ITT analysis. Furthermore, Narme et al. [29, 34] observed overall mood and well-being improvement in two interventions comparing the effect of musical to painting (study 1) or cooking (study 2) with a longer effect for musical intervention. On the opposite, another study observed a reduction of anxiety and depression with singing or music listening interventions in comparison with a third group without intervention in demented patients [19].
The stage and etiology of the disease might explain some differences. Indeed, previous studies providing a benefit of music therapy on behavioral disorders were conducted on patients with moderate to severe dementia without distinction of etiology [19 , 65–67]. The only previous RCT study focusing on mild to moderate AD patients compared the efficacy of music listening to a control group with reading intervention [28]. Conversely to our results, their findings revealed significant and long-lasting improvement in anxiety and depression in the music listening group compared to the reading group. We can suppose that painting group in LACMé study offered greater engagement than reading activity. Furthermore, their intervention could be considered as closed to relaxation [28], conversely to the singing activity used in our study.
The specific benefit of PI on depressive symptoms in our results may be due to differences in the sessions content between singing and painting. The SI were very structured and more framed. The PI sessions, in contrast, were more creative, inventive and less directed. Moreover, singing in group involves being comfortable with other people and emotional arousal, while painting is more individual. Patients with depressive symptoms tend to be introverted and may have difficulty having an activity inserted into a group.
In our study, both music and painting improved quality of life in our results and enhanced self-esteem. Our results are in line with previous reports showing an improvement of quality of life and self-esteem with non-drug therapies, without difference between type of care [19 , 68]. Related factors such as feelings of group coherence and belonging or the feeling to be taken in care and the regularity of group activities could explain this improvement, more than the content of the sessions itself.
Neuropsychological performance
The comparison between pre- and post-intervention testing revealed an improvement of inhibition processes after SI and PI, on Stroop test. To our knowledge, no previous study has assessed the influence of music or painting on inhibition. Concerning executive function, Thompson et al. reported a positive effect of Vivaldi music listening on AD patients during a verbal fluency task, compared to the same task realized without music [20]. Our results failed to observe this effect of mental flexibility. However, our measures were realized several days/weeks after intervention ending, perhaps missing that short-term effect.
In addition to inhibition improvement, our results revealed increased working memory after SI and PI sessions; however, Narme et al., who compared the effect of SI to PI on cognition, did not observe any change on cognitive performances with more severe patients [34]. Sarkamo et al. showed that SI had a specific enhancing effect on the short-term and working memory and both singing and music listening improved general cognition, attention, executive function and delayed memory in comparison with a control group without intervention [19]. Moreover, short-term benefit on working memory was more evident in a mild dementia subgroup than in a moderate one in their study [69]. Our findings, as well as these last results, could suggest that MI should be more efficient on cognitive function in patients at early stage.
Furthermore, a striking result of our study concerned the specific effect of SI on memory: we observed a stabilization of episodic verbal memory in the SI group, whereas these performances decreased in the PI group. This finding suggests that the content of our SI, such as the memorization of song lyrics together with the music, has been able to stimulate the neural networks involved in verbal memorization more strongly than did the PI. Music, especially with lyrics, is associated with activity of a widely and bilaterally distributed neural network [70] which may explain cognitive improvement or stability. Previous results revealing a memory enhancement with music in AD patients showed a benefit of encoding with a musical context [17]. Our results provide new arguments for a persistent effect of singing on episodic verbal memory, not only related to a transient increase of arousal.
Strengths of the study
Strength of our study was the use of a RCT methodology, which was only used by few previous studies [19 , 71]. Our study was multicentric, and patients were included in both SI and PI in each center. The assessors were blinded to the patient’s group. Moreover, our patients had a homogenous diagnosis of AD at prodromal or mild stage, unlike previous studies which included patients with various dementia etiologies at different stages.
In addition, we selected a painting intervention as a non-musical activity. Both activities were pleasurable, multisensory, provided in a group with a professional artistic intervener, and ended with a motivating final project supposed to develop self-esteem. These elements are in line with the recommendations for an ‘ideal’ control group, to assess music interventions [35].
Limitations
This study may have several limitations. First, the data concerning the patients’ treatments were not available in the study. It would have been interesting to compare the patients’ drugs consumption before and after the SI and PI. The drugs consumption would have been an implicit measure of interventions on pain, conversely to pain scales. Moreover, the pain drugs of certain patients could have been modified during the study, leading to a decrease in their pain scale scores.
Secondly, we observed relatively low pain scores in our patients, and patients with different etiologies of pain were included in the present study. In the future, it would be interesting to include patients with both AD and specific diseases such as headache or osteoarthritis to have more homogeneous patients concerning pain, with a higher level of pain.
Third, the study design did not include a group without intervention. It was indeed not possible to assess the natural course of the different variables collected in our study. It should have been interesting to propose to a third group a non-cognitive stimulation in order to establish the potential therapeutic effect of a non-specific care. In this absence, it could be difficult to estimate the non-specific effect of repeated meetings between patients.
However, several studies in subjects at risk of cognitive impairment showed that memory, mood, or quality of life remained unchanged or deteriorated over time without effective intervention [72, 73].
Finally, the dynamics of the improvements over time during interventions was not measured in the present analysis. This dynamic should indeed differ between painting and singing. It is also possible that an early effect on mood and/or pain manifests, but that this effect does not maintain at the same rate in later interventions. Intermediate measures would have been useful to better estimate this point.
In conclusion, the present findings showed that both SI and PI provided an improvement in various features, which is not expected in the natural course of AD. Contrary to our hypothesis, we did not highlight a superiority of SI to PI on our principal objective measures. Our results seem to show efficacy for each artistic field that could allow clinicians to orient patients according to the patients’ problems and interests.
Finally, these interventions necessitate little equipment, are easy to access, and do not require patients to have a prior predisposition or experience to perform and benefit from these activities. They could therefore be proposed to many structures managing AD patients.