
Abstract
Background:
Studies have reported that females have widespread increases in regional cerebral blood flow, but the studies were relatively small and inconsistent.
Objective:
Here we analyzed a healthy and a very large clinical psychiatric population to determine the effect of gender, using single photon emission computed tomography (SPECT).
Methods:
Whole brain and region of interest (ROI) gender differences were analyzed in a total of 46,034 SPECT scans at baseline and concentration. The sample included 119 healthy subjects and 26,683 patients (60.4% male, 39.6% female); a subset of 11,587 patients had complete diagnostic information. A total of 128 regions were analyzed according to the AAL Atlas, using ROI Extract and SPSS statistical software programs, controlling for age, diagnoses, and correcting for multiple comparisons.
Results:
Compared to males, healthy females showed significant whole brain (p < 0.01) and ROI increases in 65 baseline and 48 concentration regions (p < 0.01 corrected). Healthy males showed non-significant increases in 9 and 22 regions, respectively. In the clinical group, there were widespread significant increases in females, especially in the prefrontal and limbic regions, and specific increases in males in the inferior occipital lobes, inferior temporal lobes, and lobule 7 and Crus 2 of the cerebellum. These findings were replicated in the subset of 11,587 patients with the effect of diagnoses removed.
Conclusions:
Our results demonstrated significant gender differences in a healthy and clinical population. Understanding these differences is crucial in evaluating functional neuroimaging and may be useful in understanding the epidemiological gender differences among psychiatric disorders.
INTRODUCTION
How gender impacts brain function and influences behavior, cognition, and emotion is of critical importance in understanding the differences between genders and why some disorders are disproportionally represented, such as anxiety disorders [1], mood disorders [2], attention deficit hyperactivity disorder (ADHD) [3], autism [4], and antisocial personality disorder [5].
It is generally accepted that males and females differ in terms of brain size [6, 7], volume [8], grey/white matter ratio [9], and function [10]. Evidence indicates that healthy females generally have significantly higher rates of regional cerebral blood flow (rCBF) [10 –13] and regional cerebral metabolic rates for glucose (CMRglu) [14, 15] than males. However, not all imaging studies have observed these global differences due to variation in methodology or state, with some studies showing no gender differences at rest [16 –18], while others reporting differences during rest or cognitive tasks [10, 19].
The aim of this study was to investigate gender differences in rCBF using a region of interest (ROI) analysis in healthy subjects and a large clinical psychiatric cohort obtained over 21 years at baseline and during a concentration task with the goals of 1) quantifying rCBF gender differences in healthy individuals in whole brain average and 128 specific regions of interest; 2) comparing these results to the clinical population with and without the effect of diagnoses removed; and 3) investigating the predominant neurocircuitry that is most active in each gender across both states.
METHODS
Study subjects
We previously obtained 119 healthy adult volunteers, recruited through advertisements who had baseline (n = 88) and concentration (n = 119) SPECT studies [20]. The exclusion criteria for the study were: 1) current or past evidence of psychiatric illnesses as determined by a detailed clinical history, mental status examinations, and the Structured Clinical Interview for Diagnosis for DSM-IV (SCID-IV); 2) current reported medical illnesses or medication; 3) history of brain trauma; 4) current or past drug or alcohol abuse; 5) family history of a first-degree relatives with psychiatric illnesses. Written informed consent was obtained from all subjects under an approved IRB protocol.
In addition, we analyzed 45,915 baseline (n = 21,752) and concentration (n = 24,163) SPECT scans from a large clinical database of 26,683 patients obtained from 1995 through 2012. The average age was 41 and the range was 18–105. The patients came for the evaluation of complex and/or treatment resistant psychiatric issues to one of seven outpatient clinics (Newport Beach, Fairfield, and Brisbane, CA; Bellevue, WA; Reston, VA; Atlanta, GA; and New York, NY). In a subset of this group, we also analyzed data from 20,937 baseline (n = 10,026) and concentration (n = 10,911) SPECT scans from 11,587 patients where complete diagnostic data was available. Diagnoses were made by board certified or board eligible psychiatrists, using all of the data available to them, including a detailed clinical history, mental status examination, DSM-IV driven checklists, Beck Depression Inventory, and brain SPECT scans. Informed consent was obtained from all patients or legal guardians to allow their anonymous clinical data and SPECT scans to be utilized for research purposes. For this study, we combined the major diagnostic categories accordingly: mood disorders, bipolar disorders, anxiety disorders, posttraumatic stress disorder, substance abuse, ADHD, schizophrenia and other psychotic disorders, dementia, and brain trauma.
Brain SPECT imaging and analysis
Participants underwent high-resolution brain SPECT imaging to measure rCBF at baseline and during a concentration task as previously described [21]. Briefly, each subject received an age/weight-appropriate dose of technetium-99 m hexamethylpropyleneamine oxime (Tc-99 m HMPAO) intravenously in a dimly lit room at baseline and then again on another day while performing a concentration task (Conners’ Continuous Performance Test, CCPT-II, Multi-Health Systems, Toronto, Ontario), which measures response inhibition and attention. For the concentration task, the radiopharmaceutical was injected 3 min after starting the 15-min test. Subjects were then scanned 30–45 min after injection using a Picker Prism 3000XP triple-headed gamma camera with low energy high resolution fan beam collimators. Data was acquired in 128×128 matrices, which yielded 120 images per scan with each image separated by 3 degrees, spanning 360 degrees. SPECT data was processed and attenuation correction performed using general linear (Chang) methods [22]. All images were reconstructed using an oblique reformatting program, and oriented according to anterior-posterior commissure line, so the final images were similarly aligned for analysis.
Region of interest analysis
To minimize disruption to the individual SPECT scans caused by transforming the processed imaging data into stereotaxic space for ROI analysis, the ROI Extract software used by Amen Clinics, Inc. instead transforms the stereotaxic atlas into the individual scan space. The processed reconstructed images were left unchanged. Spatial normalization and alignment of the atlas to the individual space is performed using a mutual information based affine registration [23] algorithm implemented using the ITK Insight Toolkit [24]. Mutual information registration algorithm used in ROI Extract finds an affine transformation of a canonical SPECT scan template in Montreal Neurological Institute space that minimizes the joint entropy between the unchanged individual image and the transformed atlas image. The resulting affine transformation matrix is then applied to the atlas label map, transforming it into the subject specific space. Once the atlas has been transformed into the individual space, ROI metrics can be calculated. The Automated Anatomical Labeling (AAL) atlas was used for ROI analysis [25]. The AAL atlas consists of 128 brain regions defined across both hemispheres. ROI metrics included region mean, standard deviation, minimum, maximum, 5th percentile histograms, largest maximum valued connected cluster after thresholding, and largest minimal valued connected cluster after thresholding. These metrics serve to characterize each ROI in terms of maximum and minimum activations within those regions along with providing information on the size of those maxima and minima and histograms of the value distributions within regions. Each of these metrics is potentially useful in discriminating between disease states in the brain when compared to healthy subjects. Each of these metrics are computed and archived in anin-house data management system.
In the healthy and clinical groups, whole brain and ROI differences at baseline and concentration were then analyzed using SPSS statistical software (SPSS Inc., Chicago, IL, USA). ANOVA and MANOVA models were used to compare baseline and concentration ROI perfusion values between healthy men and women with covariates that included age and scan site. MANOVA was used to compare baseline and concentration ROI perfusion values between men and women in the psychiatric cohort with age, gender, binary identifier for major psychiatric clinical diagnoses, and site of scan as covariates. For all analyses, uncorrected and Bonferroni corrected p-values were also calculated as well as F-weights. Gender by diagnosis interactions were separately modeled. Cohen’s d [26], the proportion of a standard deviation difference between the two groups, was also calculated. Positive values indicated females were higher than males, negative values indicated males were higher than females.
RESULTS
In the healthy population, the mean age was 42±17.16 years for males (n = 35 baseline and 51 concentration) and 42.86±16.88 for females (n = 53 baseline and 68 concentration); 43% men, 57% women; range, 18 to 84. The whole brain average perfusion was significantly increased in females at both baseline (males 535.32±108.53; females 605.32±105.2; F (1, 85) = 9.08; p < 0.01; Cohen’s d = 0.65) and concentration (males 531.42±79.79; females 576.62±83.8; F (1, 116) = 8.76; p < 0.01; Cohen’s d = 0.55).
Figure 1 demonstrates ROI differences present at baseline and concentration mapped onto a 3D brain surface. At baseline, females had increased perfusion in 119 of 128 regions; perfusion of 65 regions was significantly elevated after Bonferroni correction at the p < 0.05 significance level (refer to Table 1; additional information in Supplementary Tables 1–4). The most significant regions included the bilateral amygdala, caudate, palladium, hippocampus, olfactory area, anterior, mid and posterior cingulate, insula, thalamus, multiple regions within the prefrontal cortex, precuneus, and cerebellar lobules 3, 4, 5, and 6 and areas 3 and 10 of the vermis. Males showed elevated activity in 9 regions, primarily within the left and right cerebellum Crus 2 region, right inferior occipital lobe, and anterior inferior temporal lobes, but none were significant.
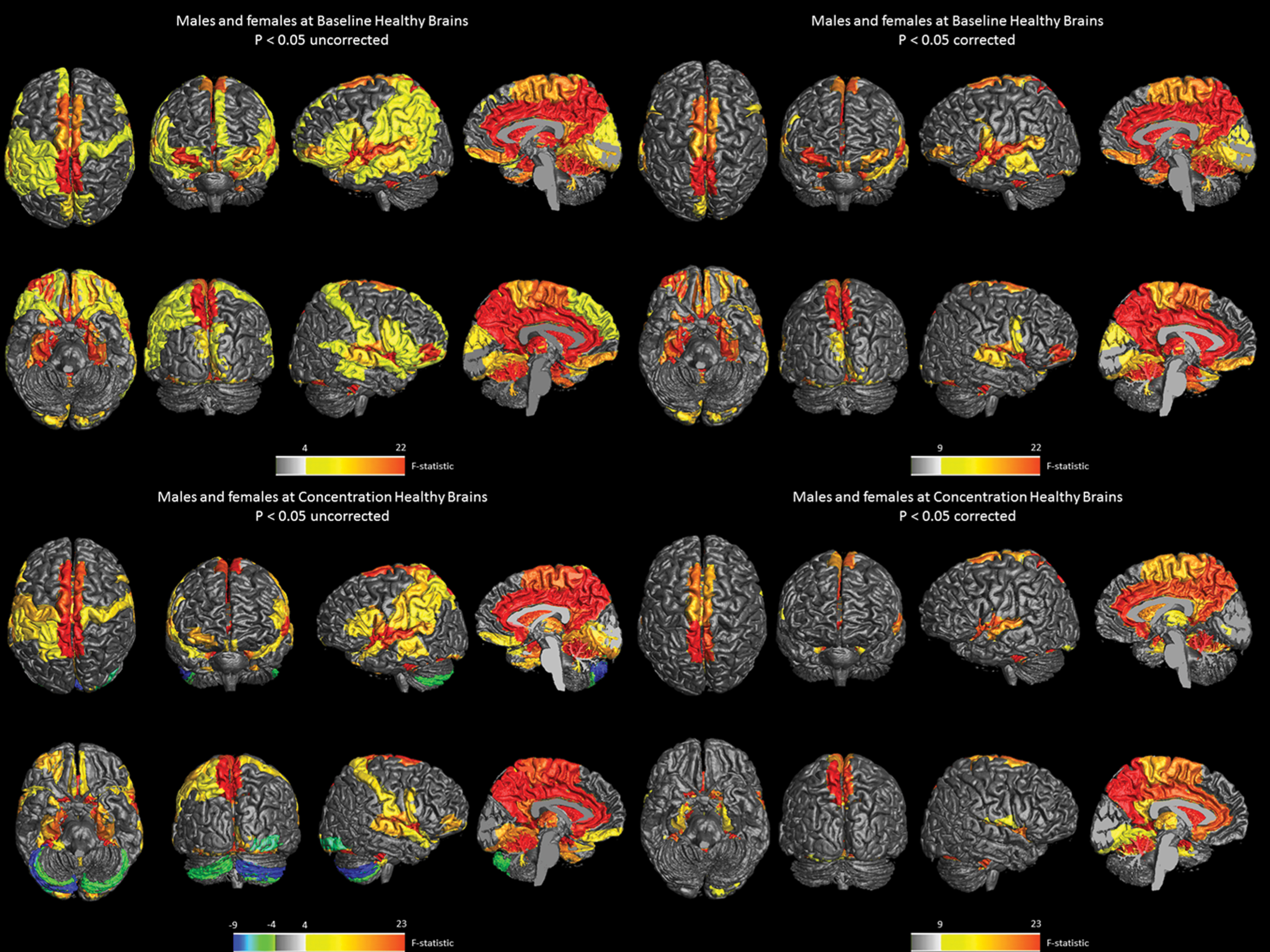
3D surface and midsagittal images illustrating regional sex differences in rCBF in healthy brain cohort at baseline (n = 88) and during a concentration task (n = 119). Figure 1 shows 3D surface and midsagittal images from region of interest analysis showing areas of significant increased perfusion in healthy females (red) and males (blue) at baseline (top) and concentration (bottom) at p < 0.05, uncorrected (left) and corrected (right). Under corrected conditions at baseline, the highest increase for males is the right cerebellum Crus 2 (d = –0.35) with an F statistic of 9, while the highest regional increase for females is in the right hippocampus (d = 1.08) with an F statistic of 22. A similar pattern was observed at concentration, with the highest regional increase for males is in the right cerebellum Crus 2 (d = –0.62) with an F statistic of 9 while the highest regional increase for females is in the vermis, region 10 (d = 0.98) with an F statistic of 23.
Effect size by region of interest across healthy brain, clinical and diagnostic cohorts
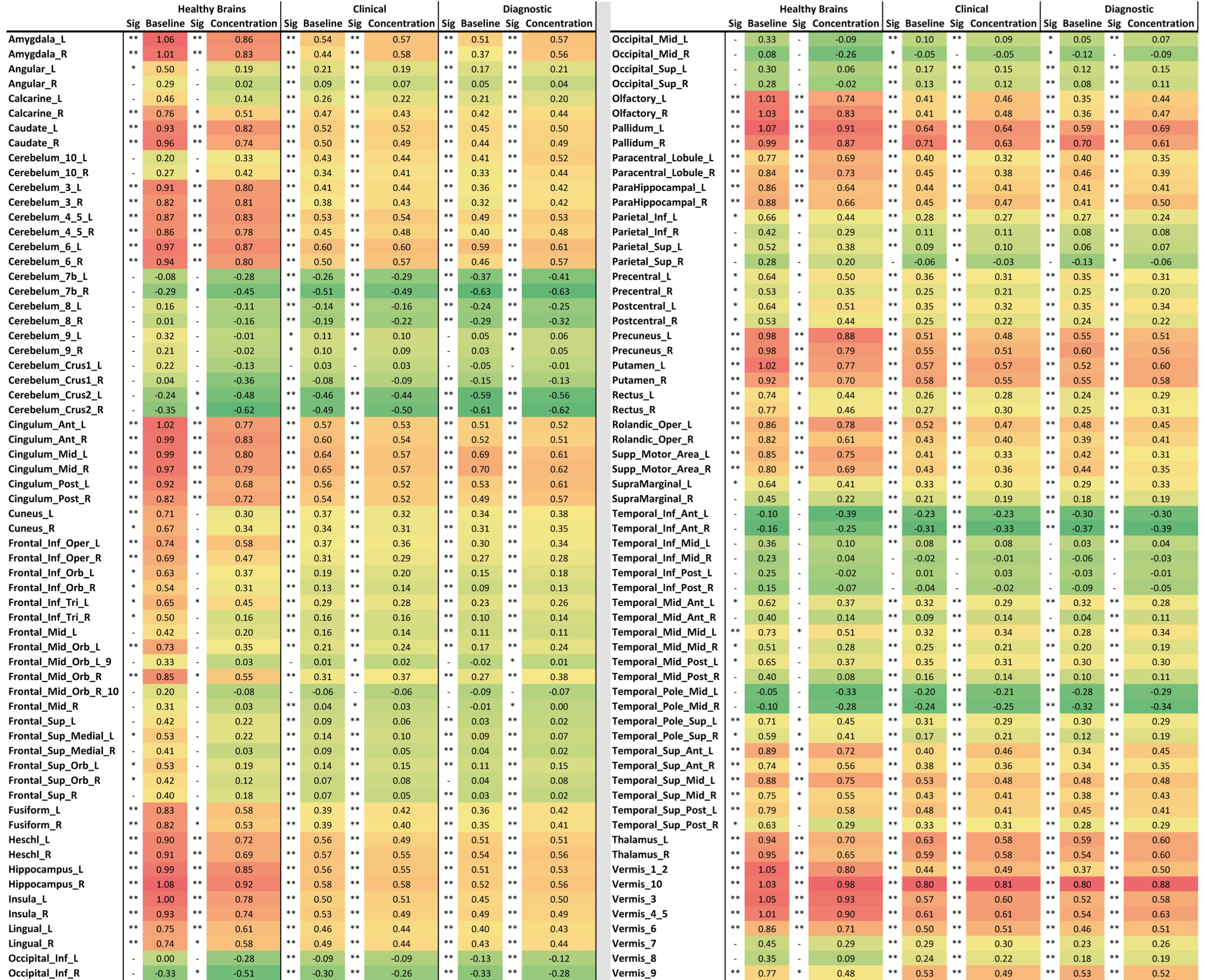
Effect size calculated by Cohen’s d for each region of interest corresponding to the AAL atlas. Each condition is shown along with asterisks to the left of each brain region indicating its significance level (- a dash indicates the region is not significant; *one asterisk is significant without correction; **two asterisks means significant after correction). Significance level is 0.05 for healthy brains and 0.01 for all others.
During concentration, healthy females had elevated activity in 106 of 128 regions; 48 areas were significantly elevated after Bonferroni correction (Table 1). The most significant ROIs were similar to baseline. Males had elevated activity in 22 areas of the brain, primarily within the left and right cerebellum Crus 2 region, right inferior occipital lobe, which were both significant (p < 0.05, uncorrected), and anterior and inferior temporal lobes, non-significant.
In the clinical population, the mean age was 31.13±17.44 years for males (n = 13,579 baseline and 14,762 concentration) and 31.16±17.41 for females (n = 8,173 baseline and 9,401 concentration); 61% male, 39% female; age range, 2 to 98. Whole brain averages from this group showed significant increases for females at baseline (n = 21,752 scans; males 509.92±157.92; females 565.15±140.35; F (1, 21748) = 628.606; p < 0.001; Cohen’s d = 0.37) and concentration (n = 24,163 scans; males 495.07±151.44; females 547.92±149.77; F (1, 24156) = 696.06; p < 0.001; Cohen’s d = 0.35). The clinical group showed a similar rCBF ROI pattern to those of the healthy group, but the level of statistical significance was markedly elevated, F values ranging from 2253 to –996. At baseline and concentration, females had elevated perfusion in 110 of 128 regions; 107 regions were significant after Bonferroni corrections (Table 1). Males showed elevated perfusion in 18 regions; 13 were significant after correction.
At baseline and concentration, females showed significantly higher activity in all but one region of the prefrontal cortex (right mid orbital, non-significant), caudate, thalamus, hippocampus, parahippocampal gyrus, amygdala, and anterior, mid and posterior cingulate gyrus, while males had higher perfusion in the inferior occipital lobes, inferior temporal lobes, and area 7 and Crus 2 of the cerebellum (Fig. 2).
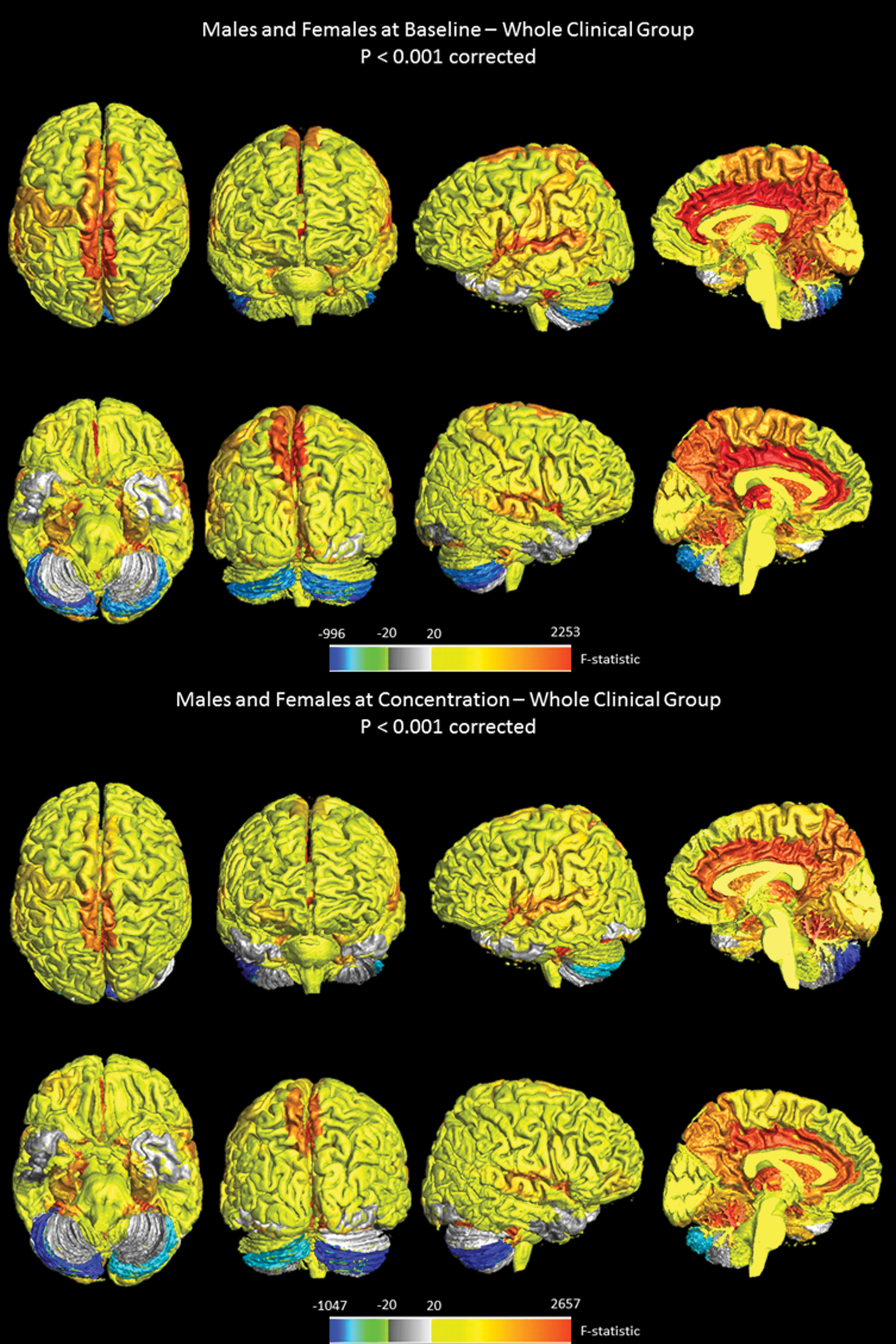
3D surface and midsagittal images illustrating regional sex differences in rCBF in clinical cohort of 26,683 patients at baseline (n = 21,752) and during a concentration task (n = 24,163). Figure 2 shows 3D surface and midsagittal images from region of interest analysis showing areas of significant increased perfusion in clinical females (red) and males (blue) at baseline (top) and concentration (bottom) at p < 0.001 corrected. At baseline, the highest increase for males is in the right cerebellum Crus 2 (d = –0.49) with an F statistic of –996, while the highest regional increase for females is in the vermis, region 10 (d = 0.80) with an F statistic of 2253. A similar pattern was observed at concentration, with the highest increase for males is in the right cerebellum Crus 2 (d = –0.50) with an F statistic of –1047 and the highest regional increase for females is in the vermis, region 10 (d = 0.81) with an F statistic of 2657.
Of the clinical group, complete diagnostic information was currently available on 11,587 of the 26,683 cases used in the analysis. We speculated the results from this cohort would be similar to that of the whole group when the effect of diagnoses was removed (refer to Table 1 and Fig. 3). In this subset, the mean age was 32.43±17.66 years for males (n = 6,144 baseline and 6,608 concentration) and 38.19±18.17 for females (n = 3,882 baseline and 4,303 concentration); 60.5% male, 39.5% female; age range, 2 to 89. See Table 2 for gender differences among major diagnostic categories. Analysis of whole brain averages at baseline revealed that the overall strength of effect of gender was larger (F (1, 10595) = 261.75; p < 0.001; d = 0.34) than the effect of any diagnosis. Of the pathologies studied, brain trauma showed the largest effect (F (1, 10602) = 43.46; p < 0.001; d = 0.17), followed by bipolar disorders (F (1, 10602) = 36.36; p < 0.001; d = 0.14), mood disorders (F (1, 10602) = 9.45; p =0.002; d = 0.08), schizophrenia/psychotic disorders (F (1, 10602) = 8.29; p = 0.004; d = –0.15), and ADHD (F (1, 10602 = 3.994; p = 0.046; d = –0.006). There was an interaction between gender and diagnosis for brain trauma (F (1, 10602) = 6.50; p = 0.011), ADHD (F (1, 10602) = 6.47; p = 0.011), anxiety (F (1, 10602) = 6.10; p = 0.014), post traumatic stress disorder (F (1, 10602) = 8.8; p = 0.003), and substance abuse (F (1, 10602) = 4.09; p = 0.043). At concentration, the effect of gender is greater than at baseline (F (1, 11571) = 367.382; p < 0.001; d = 0.37), and the effect of ADHD becomes stronger (F (1, 11571) = 6.94; p < 0.008; d = –0.008). Taken together, these results demonstrate that the effect of gender is a stronger determinant of cerebral blood flow and may interact with the pathophysiology of some neuropsychiatric disorders.

3D surface and midsagittal images illustrating regional sex differences in rCBF in a smaller clinical cohort with the effect of diagnoses removed in 11,587 patients at baseline (n = 10,026) and during a concentration task (n = 10,911). Figure 3 shows 3D surface and midsagittal images from region of interest analysis on a smaller subset of the clinical cohort with the effect of diagnoses removed showing areas of significant increased perfusion in females (red) and males (blue) at baseline (top) and concentration (bottom) at p < 0.001 corrected. At baseline, the highest increase for males is in the right cerebellum Crus 2 (d = –0.61) with an F statistic of –556 while the highest regional increase for females is in the vermis, region 10 (d = 0.80) with an F statistic of 1025. A similar pattern was observed at concentration, with the highest increase for males is in the right cerebellum Crus 2 (d = –0.62) with an F statistic of –759 and the highest regional increase for females is in the vermis, region 10 (d = 0.88) with an F statistic of 1724.
Demographic of diagnostic categories
Sample distribution by gender shown for each diagnostic category evaluated in study. Results highlighted in grey show diagnostic categories where the sample distribution significantly differs from the expected male/female ratio.
DISCUSSION
To our knowledge, this is the largest study using functional neuroimaging to help understand the effect of gender differences in healthy and clinical psychiatric populations. The main findings were: 1) Significant gender differences exist in both healthy and psychiatric cohorts at baseline and during a concentration task. 2) In the healthy group, the results become more statistically significant during a concentration task. 3) There are highly statistically significant differences in the clinical group during both conditions, even when the effect of diagnoses is removed. 4) Females have greater whole brain average perfusion and many areas of increased perfusion throughout the brain. The same pattern of results appeared in both the healthy and clinical samples, but they became much more statistically significant in the large clinical sample. 5) Female brains have increases in rCBF in 83–96% of the ROIs, especially in the areas of the prefrontal, frontal, and limbic parts of the brain; males had higher rCBF in 4–17% of ROIs, especially in the inferior temporal and occipital lobes and cerebellar lobule 7 and Crus 2.
The increased perfusion in the prefrontal cortex in females may, in part, explain why females tend to have a lower incidence of externalizing disorders, such as ADHD and antisocial personality disorder [5]. Since the prefrontal cortex is also involved in forethought and self-control [27], it may be one of the reasons why females have a lower incidence of substance abuse [28] and incarcerations [29]. The increased limbic perfusion may contribute to females being more vulnerable to mood disorders [30]. In both groups, females show significantly higher rCBF bilaterally in the amygdala, an area important in processing emotional information, and a region more active in females prone to anxiety and depression [31]. The default mode network was also significantly more active in females. It comprises the posterior cingulate cortex/precuneus, medial prefrontal/pregenual cingulate cortices, temporoparietal regions, and medial temporal lobes and has been implicated in episodic memory retrieval, self-reflection, mental imagery, and stream-of-consciousness processing [32]. Additional studies with larger numbers of disease free controls for comparison would be necessary to fully confirm these observations and interpretations.
While females have a higher risk for Alzheimer’s disease than males [33], this relationship would not be expected given the baseline higher perfusion in the hippocampus and precuneus in females compared to males. This is because perfusion is frequently decreased in Alzheimer’s disease early in the course of the disorder [34] supporting the concept that higher perfusion may be protective. However, the increased risk in women may occur due to the post-menopausal lack of estrogen. Since estrogen has been shown to promote perfusion in the female brain [35], decreased levels may remove the protective higher perfusion we observe in this study.
Men consistently demonstrated more rCBF along the ventral visual stream (inferior occipito-temporal lobes), sometimes called the “What Pathway,” associated with visual perception, form recognition, and object representation [36], while females had increased rCBF in the dorsal visual stream, associated with the visual control of action. Males also had increased rCBF in lobule 7 and Crus 1 and 2 of the cerebellum; these areas have been associated with executive control [37].
One limitation of the study was the high rate of comorbidity in patients, common in real world clinical practices. Future work will be aimed at parsing ROI sex differences in areas most influenced by specific pathologies (i.e., amygdala in anxiety disorders), and further elucidating how gender differences interact with the disease process. Another limitation was that we did not account for hormonal or menopausal status within either cohort. Even though we controlled for age, the contribution of hormonal status is significant in studies on cerebral blood flow and should be accounted for in future gender analysis [38 –40]. In addition, we did not have detailed diagnostic information on the entire clinical sample.
This study suggests that it is critically important to always consider gender differences whenever analyzing SPECT, and likely other functional neuroimaging data. This work also lays a foundation for understanding the neurophysiological basis of differential gender risk for psychiatric and neurodegenerative disease. Future studies can use such information to tailor precision medicine treatments of these disorders.
DISCLOSURE STATEMENT
Authors’ disclosures available online (http://j-alz.com/manuscript-disclosures/17-0432r2).