
Abstract
Background:
The course of Alzheimer’s disease (AD) varies considerably between individuals. There is limited evidence on factors important for disease progression.
Objective:
The primary aim was to study the progression of AD, as measured by the Clinical Dementia Rating Scale Sum of Boxes (CDR-SB). Secondary aims were to investigate whether baseline characteristics are important for differences in progression, and to examine the correlation between progression assessed using three different instruments: CDR-SB (0–18), the cognitive test Mini-Mental State Examination (MMSE, 0–30), and the functional measure Instrumental Activities of Daily Living (IADL, 0-1).
Methods:
The Progression of AD and Resource use (PADR) study is a longitudinal observational study in three Norwegian memory clinics.
Results:
In total, 282 AD patients (mean age 73.3 years, 54% female) were followed for mean 24 (16–37) months. The mean annual increase in CDR-SB was 1.6 (SD 1.8), the mean decrease in MMSE score 1.9 (SD 2.6), and the mean decrease in IADL score 0.13 (SD 0.14). Of the 282 patients, 132 (46.8%) progressed slowly, with less than 1 point yearly increase in CDR-SB. Cognitive test results at baseline predicted progression rate, and together with age, ApoE, history of hypertension, and drug use could explain 17% of the variance in progression rate. The strongest correlation of change was found between CDR-SB and IADL scores, the weakest between MMSE and IADL scores.
Conclusion:
Progression rate varied considerably among AD patients; about half of the patients progressed slowly. Cognitive test results at baseline were predictors of progression rate.
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia, accounting for 50–70% of cases. Because of population aging, AD affects increasing numbers of people worldwide. The progressive disorder leads to increasing disability, with substantial impact on individuals, families, and societies. Therefore, to decrease the disease burden, it is highly important both to reduce the risk of developing AD and to slow its progression.
Symptoms and impairments resulting from AD usually become apparent at the prodromal stage of dementia, also called mild cognitive impairment (MCI) [1]. In addition to the cognitive decline, disease progression in AD leads to a loss of functional abilities, typically with initial impairments in instrumental activities of daily living (IADL) and later impairments in basic ADL. Thus, disease progression can be measured with scales that assess cognition or function, or with global scales that provide a compound measure of disease severity. The cognitive and functional decline may be disparate and describing the changes in more than one way may give a more thorough picture of the situation [2].
As a global assessment scale measuring progression of AD, the Clinical Dementia Rating (CDR), with its continuous scale the Clinical Dementia Rating Sum of Boxes (CDR-SB), is frequently used. A mean yearly change in CDR-SB between 1.4 and 2.3 points is reported for patients with AD. Disease progression in AD is generally described as slower in the initial stages than in a more advanced stage of the disease, with yearly progression in CDR-SB of 0.5 to 1.9 points among patients with amnestic MCI (aMCI) or very mild dementia (CDR 0.5) and 1.3 to 1.9 points among patients with mild dementia (CDR 1) [3–6]. There is considerable individual variation in progression rates [7, 8]. Using the Mini-Mental State Examination (MMSE) to measure cognition, the average loss is between 1.5 and 2.3 points per year [5, 9]. A rapid cognitive decline, defined as a decrease of 3 to 5 points per year on the MMSE [8], has been shown in 10–30% of AD cases, depending on the threshold set and the population studied [8, 10]. Few studies have examined factors related to slow decline in AD [9].
A population-based study found that 30–58% of the participants with AD declined slowly, with a yearly change of less than one point on the CDR-SB and the MMSE [6]. Consistent with this finding, two memory clinic studies found that 25–30% of the patients were stable over a period of two to three years [5, 8].
Some studies have shown that young age at onset, high educational level, and severity of cognitive and functional impairment at the time of diagnosis are associated with rapid decline in AD patients [11]. There is still a considerable lack of evidence on other predictors for the rate of decline in individual patients with AD [12]. Knowledge about the prognosis for individual patients is very important to enable better planning for the future. Further, the identification of modifiable predictors for the disease course could be a target for future intervention studies focusing on treatment that might hamper disease progression. Therefore, more research is needed on well-defined and clinical AD populations focusing on various aspects of disease progression.
The primary aim of the present study was to study the overall progression of AD, as measured by the primary outcome measure CDR-SB. Further, we wanted to investigate whether baseline characteristics are of importance for differences in progression, and to examine the correlation between the progression assessed by a global score (CDR-SB) and progression in cognitive (MMSE) and functional (IADL) measures.
MATERIALS AND METHODS
Study design
The Progression of Alzheimer’s Disease and Resource use (PADR) study is a longitudinal observational study with assessments at the time of diagnostic workup (baseline) and follow-up after a mean of 24 months (range 16–37, 80% between 20 and 28 months).
Recruitment of patients
The PADR study recruited patients from three memory clinics in Norway. Patients were referred by general practitioners or other specialists. To be included in the PADR study, patients must have MCI or dementia at baseline, be home dwelling, able to give informed consent, and have a proxy who could serve as an informant. Patients who were not fluent in Norwegian, had severe physical illness, or lived far away from the memory clinics were excluded.
Two of the memory clinics were affiliated to the Norwegian register for persons with cognitive symptoms (NorCog), a clinical register recruiting patients from memory clinics with standardized assessments [13]. Between May 2009 and June 2012, 352 of the patients in NorCog from Oslo University Hospital and Innlandet Hospital Trust were included in the PADR study. Of these, 212 patients with MCI or dementia at baseline underwent the follow-up assessment.
In addition, the geriatric outpatient clinic at St Olav University Hospital in Trondheim recruited 203 patients between February 2010 and February 2014. Of these, 128 patients underwent a follow-up assessment. For 17 additional patients who were not able to meet for follow-up assessment due to their medical condition, information was collected from caregivers only.
Of the 357 patients who participated in the follow-up assessments, 75 had been diagnosed at baseline with cognitive impairment due to etiologies other than AD. Included in the present study were 282 patients with a diagnosis of AD dementia or aMCI at baseline. A total of 177 (62.8%) had AD dementia and 105 (37.2%) had aMCI. The aMCI patients were judged to have AD.
The study was conducted in accordance with the Helsinki Declaration of 1975. The Regional Committee for Medical and Health Research Ethics in South East Norway approved the study (REC number 2011/531). Patients received oral and written information and gave written consent to participate. Only patients with capacity to consent were recruited at baseline, as recommended by REC.
Assessments
The baseline assessments of patients and interviews with caregivers were performed as regular consultations by consultants and nurses employed at each memory clinic and standardized in a research manual. All patients underwent a physical and neuropsychological examination and structural brain imaging (magnetic resonance imaging (MRI) in most cases, otherwise computed tomography scan). Blood sample analyses were done for standard assessments. Cerebrospinal fluid (CSF) was drawn in 110 of the 282 patients (34% of aMCI patients and 42% of patients with AD dementia) and analyzed for Aβ42, T-tau, and P-tau. Apolipoprotein E (ApoE) genotyping was conducted using the Illumina Infinium OmniExpress v1.1 chip at deCODE Genetics, Reykjavik, Iceland, and the result was dichotomized based on the presence of at least one ApoE ɛ4 allele into carriers and non-carriers of ApoE ɛ4. The study researchers performed the follow-up assessments. If possible, patients living in nursing homes at the time of follow-up assessments were visited at their place of living. Otherwise, information was collected through telephone interviews with caregivers. Ongoing use of cholinesterase inhibitors and/or memantine at follow-up was registered. Severity of depressive symptoms was rated with the Cornell Scale for Depression in Dementia (0–19) and the Montgomery and Aasberg depression rating scale (0–60) [14, 15].
Diagnostic workup
The ICD-10 criteria for research were used to diagnose dementia [16] and the Winblad criteria to diagnose MCI [1]. The criteria defined by the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) were used for AD dementia [17]. MCI patients with impaired memory as an early symptom and a score equivalent to or below 1.5 SD on at least one memory test [18] were categorized as AD (without dementia). This group included multi-domain amnestic MCI patients in addition to those with only memory impairment. Diagnoses were assigned by the study researchers reviewing all available data from the baseline examination; no diagnoses were revised based on the subsequent disease course. Information on ApoE status was not available in the diagnostic process. Decreased beta amyloid and/or elevated phospho tau or total tau in CSF supported AD diagnosis. No patients with non-amnestic MCI or dementia other than AD had CSF biomarkers consistent with AD (CSF available for 20 of 75 patients).
Outcome measures
The primary outcome measure was the CDR-SB. The CDR evaluates six areas: memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care [19]. The score on each item may be zero, 0.5, 1, 2, or 3. A global score, staging the disease from zero to 3, is obtained based on an available online algorithm that gives precedence to the memory item. Severity of cognitive impairment was categorized by CDR global score at baseline, in the groups CDR 0.5 (very mild AD), CDR 1 (mild AD), and CDR 2 (moderate AD). For research, the item scores can be summed to produce a continuous scale, CDR-SB (0–18, higher scores denoting more severe impairment). All study researchers underwent online training and were certified as “CDR raters” [20] before scoring the CDR based on all information available from the baseline assessments. In accordance with other studies assessing progression in dementia with CDR-SB [6, 8], patients who had an increase of less than 1 point in the CDR-SB score per year of follow-up were regarded as slow progressors.
A comprehensive cognitive test battery was performed at baseline and repeated at follow-up, including the MMSE (0–30), the word-list test from the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) (delayed recall of 10 words), the clock drawing test (0–5), and the Trail Making Test A and B [21–24]. Patients with an average annual decrease in the MMSE score of <1 point, 1–6 points or ≥ 6 points were classified as slow [6, 8, 9], intermediate [9], and rapid progressors, respectively [9, 10].
IADL performance was assessed using the scale of Lawton and Brody [25]. The IADL scale evaluates eight items, and each can be scored as “0” (dependent) or “1” (independent). Three of the items (“prepare food”, “housecleaning”, and “laundry”) were not applicable for many of the patients, especially in men. They were therefore omitted from the analyses. The sum score was divided by the number of items evaluated, giving a score ranging from 0 (completely dependent) to 1 (completely independent) [25]. Patients were regarded as slow progressors in IADL if they lost independence on a maximum of one IADL item from baseline to follow-up.
Statistics
Descriptive statistical methods were used for baseline characteristics. For comparisons between groups, independent samples t-tests were used for continuous data, and Pearson’s χ2 test was used for categorical data. Change from baseline to follow-up was calculated dividing score differences by time in years and was approximately normally distributed. In order to check the validity of the primary analyses, the missing MMSE values at follow-up (19/282) were imputed with multiple imputation, based on age, education, MMSE, and CDR-SB at baseline and dementia diagnosis, place of residence (nursing home or own home), and CDR-SB at follow-up.
A multiple linear regression analysis was conducted with the progression measured by CDR-SB change as the dependent variable. First, unadjusted analyses were carried out for demographic variables, results of cognitive tests at baseline and history of previous diseases. Before conducting the analyses, we checked for inter-correlations between independent variables using the Spearman correlation coefficient. Variables that were intercorrelated with a Spearman rho of >0.5 were not included in the analyses. The Trail Making Test A and the clock drawing test were excluded from the regression analyses because of high correlation with the Trail Making Test B and each other, and the MMSE was excluded because of high correlation with both the word-list delayed recall test and the Trail Making Test B. As independent variables, we therefore included age, sex, whether the patient was living alone, length of formal education, ApoE genotype, previous diagnoses, number of drugs used regularly, symptom duration at the time of diagnosis, and the CERAD word-list delayed recall test, as well as the Trail Making Test B. Multiple regression analyses were performed including independent variables with p values <0.2 from the unadjusted analyses. The adjusted model included 204 patients with complete data on all these variables. The model was checked for multicollinearity by tolerance statistics and variance inflation factor.
The external responsiveness, the extent to which a change in one measure over time relates to corresponding changes in another measure, was examined for the changes per year for CDR-SB, MMSE, and IADL. Spearman correlation coefficients were calculated to compare these changes. Based on factor analyses from other studies of CDR-SB [3, 4], we also divided CDR-SB into “cognitive” and “functional” subscores. The cognitive subscore included the first three items (memory, orientation, and judgment) and the functional subscore the last three (community activities, home and hobbies, and personal care). We also explored the correlation between the change in cognitive and functional subscore of CDR-SB with the changes in CDR-SB, MMSE, and IADL.
Data were analyzed using IBM SPSS Statistics for Windows, version 23.0, Armonk, NY, USA. Statistical significance was defined as p < 0.05.
RESULTS
Of the 555 patients with cognitive impairment or dementia included at baseline, 198 were lost to follow-up, and 75 had other causes of cognitive impairment than AD (Fig. 1). Patients lost to follow-up had almost one year less of formal education, were more likely to live alone (38% versus 28%) and to be smoking (20% versus 11%), as compared to patients who remained in the study. A higher proportion of patients lost to follow-up had a score below – 2 SD on the Trail Making Test A (46% versus 36%) and B (69% versus 52%). There were no significant group differences for other cognitive tests nor for comorbidities.
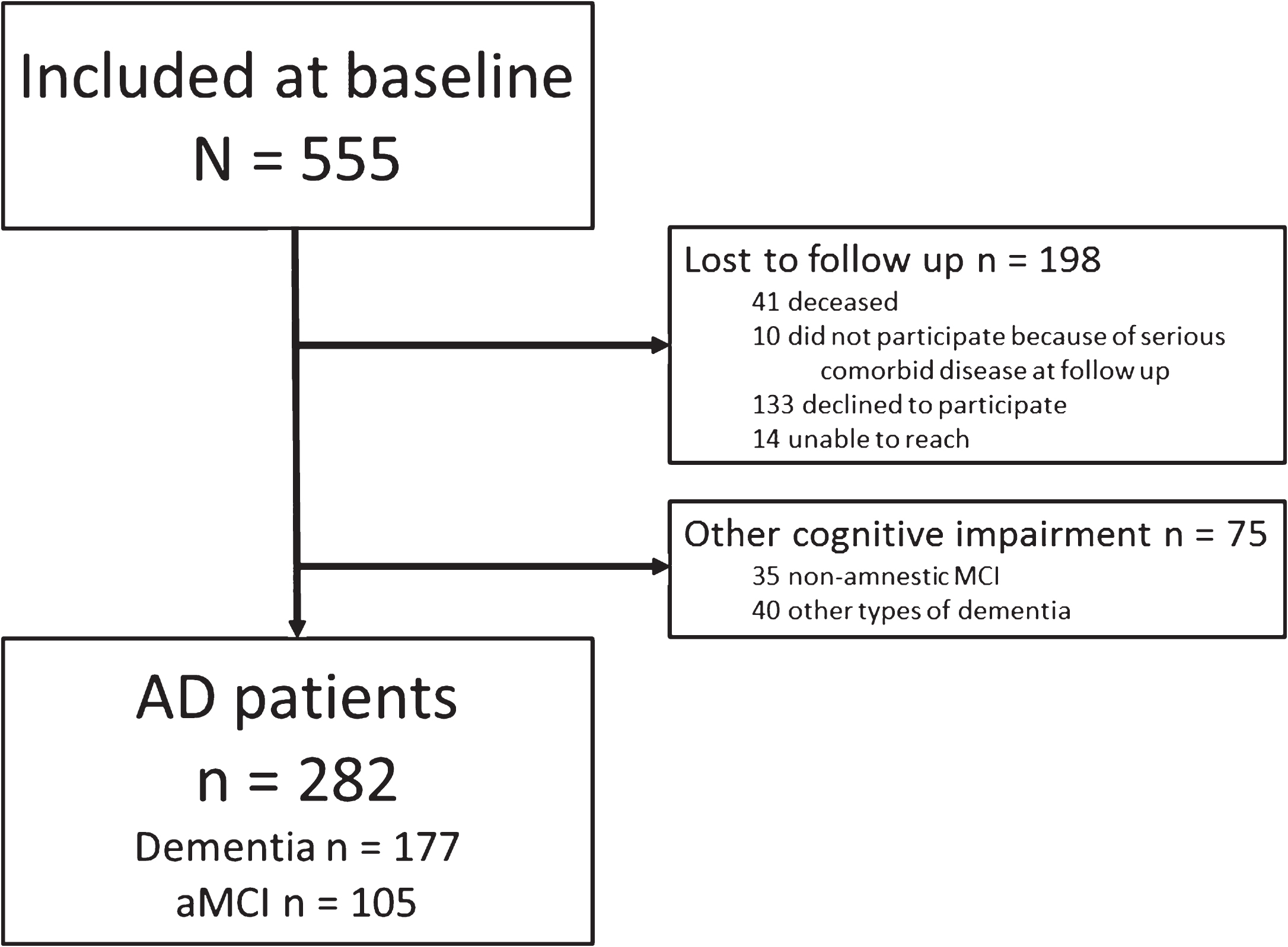
Study flow chart. Other types of dementia (n = 40) among patients with follow-up assessments: Dementia in Parkinson’s disease (n = 12). Dementia with Lewy bodies (n = 8). Vascular dementia (n = 7). Frontotemporal dementia (n = 4). In addition, two patients were diagnosed with other specified types of dementia and seven had unspecified dementia.
Of the 282 AD patients who participated in follow-up, 155 had a global CDR score of 0.5 (very mild AD), 105 had a CDR score of 1 (mild AD), and 22 had a CDR score of 2 (moderate AD) at baseline. Of the 105 aMCI patients, 98 had a CDR score of 0.5; the rest had CDR 1. The baseline characteristics of the AD patients are summarized in Table 1. The mean age was 73.3±8.8 years, mean length of education 11.7±3.6 years, and 54.3% were females. The mean MMSE score was 23.7±4.4, mean IADL score 0.78±0.22 and mean CDR-SB score 4.2±2.8. Symptoms started before age 65 in 19% of patients with dementia and in 38% of patients with MCI at baseline. Half of the aMCI patients with symptoms before age 65 had developed dementia by follow-up.
Clinical and demographic characteristics at baseline
ApoE, Apolipoprotein E; CDR, Clinical Dementia Rating scale; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; ChEI: Cholinesterase inhibitors; CSF: cerebrospinal fluid; IADL, Instrumental Activities of Daily Living; MMSE, Mini-Mental State Examination; TIA: Transient Ischemic Attack. *Ongoing use of cholinesterase inhibitors and/or memantine was recorded at follow-up.
As shown in Table 2, the mean increase (worsening) in CDR-SB was 1.6±1.8 points/year (cut-points for highest and lowest quartiles 0.3 and 2.2 points per year). We found no differences in progression between users (n = 122) and non-users (n = 160) of cholinesterase inhibitors or memantine.
Progression from baseline to follow-up, measured in CDR-SB, MMSE, and IADL
CDR, Clinical Dementia Rating Scale, MMSE, Mini-Mental State Examination, IADL, Instrumental Activities of Daily Living.
Table 3 shows the results of linear regression analyses for predictors associated with CDR-SB change. In the unadjusted linear regression analyses, there was a statistically significant association between age, number of drugs taken regularly, Trail Making Test B scores, the CERAD word-list delayed recall, and change in CDR-SB. In the adjusted analysis, the Trail Making Test B scores remained statistically significant. A model including age, ApoE ɛ4 carrier status, Trail Making Test B score, word-list delayed recall score, history of hypertension, and the number of drugs taken regularly explained R2 = 17% of the variance of the change in CDR-SB score. With a mean variance inflation factor of 1.19 and tolerance statistics between 0.76 and 0.91, multicollinearity was not found to be a problem for this model.
Associations between baseline variables and the progression of AD as measured by annual CDR-SB change
ApoE, Apolipoprotein E; CDR-SB, Clinical Dementia Rating scale Sum of Boxes; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; TIA: Transient Ischemic Attack. *n = 204 with complete data on all included variables in the adjusted model.
The number of slow progressors in terms of CDR-SB change was 132 (46.8%), with 32 patients (11.3%) having better CDR-SB score at follow-up, 20 (7.1%) unchanged score, and 80 (28.4%) with less than 1 point increase in CDR-SB per year. The number of patients who were slow progressors was 80 (51.6%) among patients with very mild AD, 46 (43.8%) among patients with mild AD and six (27.3%) among those with moderate AD (p = 0.075). As shown in Table 4, slow progressors were younger at diagnosis, had longer formal education, used fewer drugs, had slightly better IADL function, better scores on cognitive tests, and scored one point less on CDR-SB at baseline. There were no differences in the use of anti-dementia medications or in depressive symptoms among individuals with improved scores as compared to the rest of the patients.
Comparison of slow progressors with intermediate or rapid progressors from baseline to follow-up
ApoE, Apolipoprotein E; CDR, Clinical Dementia Rating scale; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; IADL, Instrumental Activities of Daily Living. Slow progression defined as <1 point increased score in CDR-SB per year. Intermediate or rapid progression defined as >1 point increased score in CDR-SB per year. aGroup comparisons.
The mean decline in MMSE scores was 1.9 points/year (SD 2.6, cut-points for highest and lowest quartiles 0 and 3.1 points/year) (Table 2), and 116 patients (44.4%) decreased less than 1 point/y (Fig. 2). Multiple imputation of missing MMSE values at follow-up resulted in a mean decline of 2.1 points/year for all patients and changed the proportion of slow progressors to 42.9%. The mean decline in IADL was –0.13/year (SD 0.14), and 163 patients (60.4%) showed little decline, of which 71 patients lost independence on only one IADL item from baseline to follow-up, 78 had unchanged score, and 14 improved.
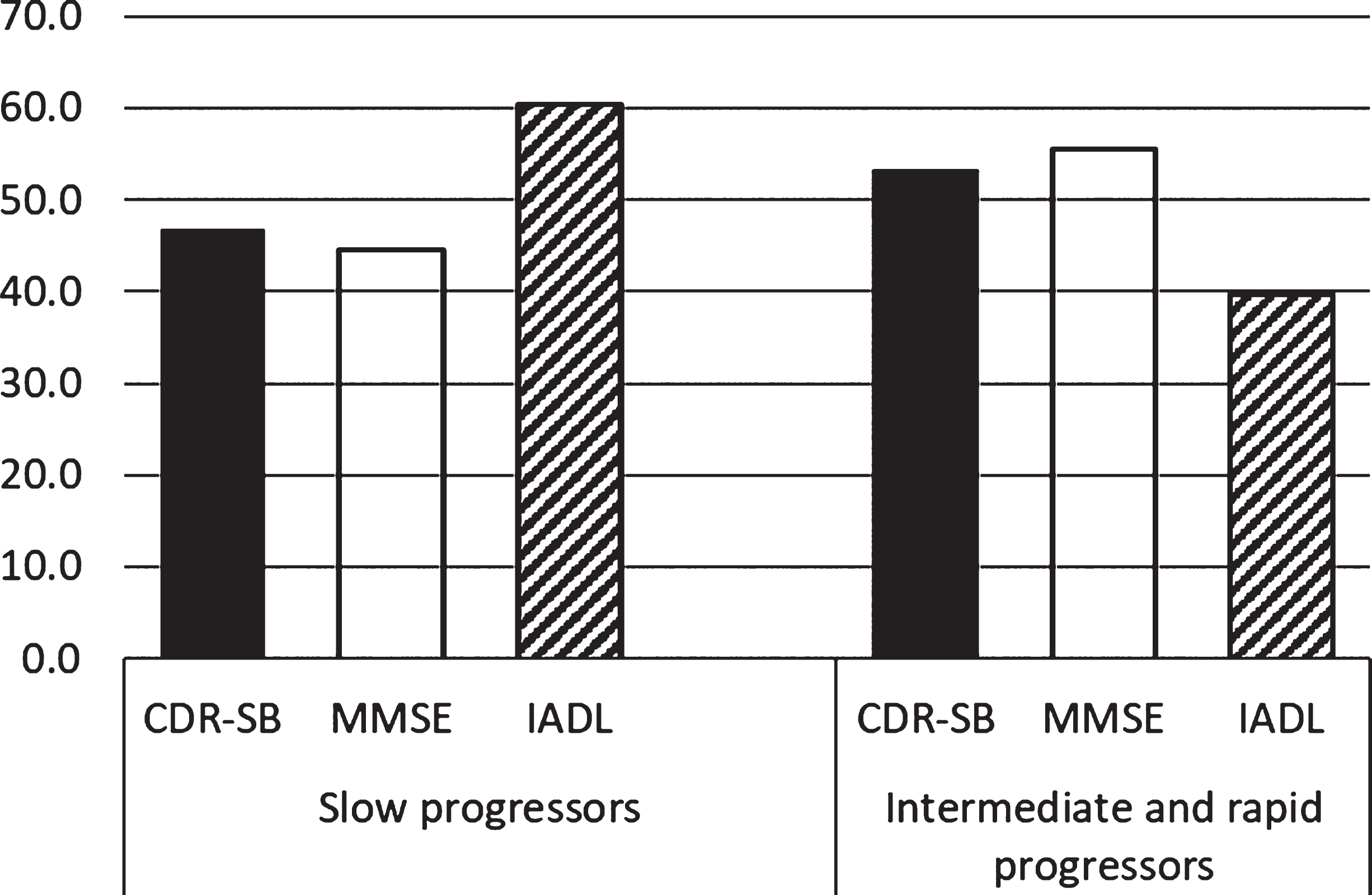
Percentage of patients being slow progressors or experiencing intermediate or rapid progression, as measured by a global score (CDR-SB), a cognitive test (MMSE) and an assessment of function (IADL). CDR-SB, Clinical Dementia Rating scale sum of boxes; MMSE, Mini-Mental State Examination; IADL, Instrumental Activities of Daily Living (Lawton and Brody). Slow progression defined on CDR-SB and MMSE as <1 point worsened score per year, and on the IADL scale (Lawton and Brody) defined as loss of independence in maximally 1 IADL function over the follow-up period of mean 2 years. Intermediate or rapid progression defined as score differences from baseline to follow-up above the defined thresholds for progression.
Rapid progression, as defined by a decrease in MMSE score of 6 points or more per year, was found in 19 (7.3%) patients, whereas 116 (44.4%) were slow progressors, and 126 (48.3%) intermediate progressors. Better scores on cognitive tests and CDR-SB at baseline predicted slow progression as measured both with the MMSE and IADL (results not shown).
As shown in Table 5, the correlation between the change in CDR-SB and the change in IADL (–0.61) was somewhat stronger than that between the CDR-SB and MMSE (–0.53). The changes in both the cognitive and the functional subscore of CDR-SB correlated more strongly with IADL (–0.49 and –0.59, respectively) than with MMSE scores (–0.44 and –0.49, respectively). The weakest correlation was between changes in MMSE and IADL scores (0.36). When analyzed separately by CDR group, correlations were generally strongest for the CDR 1 group, for which correlations between change in CDR-SB and change in IADL and MMSE were –0.65 and –0.53, respectively. For the CDR 0.5 group correlations between change in CDR-SB and change in IADL and MMSE were –0.61 and –0.47, respectively. The CDR 2 group had the weakest correlation between change in CDR-SB and change in IADL (–0.43), while the correlation with change in MMSE was the strongest (–0.59).
Correlations between changes per year from baseline scores (Spearman correlation coefficients)
p values for all correlations shown are <0.001. CDR-SB, Clinical Dementia Rating scale Sum of Boxes; CDR-SB cognitive subscore, the sum of the items memory, orientation, and judgment; CDR-SB functional subscore, the sum of the items community affairs, home and hobbies, and personal care; MMSE, Mini-Mental State Examination; IADL, Instrumental Activities of Daily Living.
DISCUSSION
This study investigates the progression of AD, predictors for progression and the correlation between change in a global score (CDR-SB), a cognitive (MMSE) and a functional measure (IADL). The overall progression rate of AD patients in the PADR study is similar to what has been reported in other studies. However, we found considerable heterogeneity, as half of the patients progressed slowly over the follow-up period of two years. Multiple regression analysis showed that the Trail Making Test B and the CERAD word-list delayed recall at baseline predicted progression, and could together with age, ApoE4 carrier status, hypertension, and the number of drugs used explain 17% of the variance in CDR-SB change. The correlation between changes in CDR-SB, MMSE and IADL scores seemed strongest between the CDR-SB and IADL and least strong between the MMSE and IADL scores.
Although AD is a progressive disorder, we found that a large proportion of patients experienced no or little decline during two years of follow-up, which is consistent with other studies [5, 9]. The large proportion of slow progressors illustrates the need to look beyond the mean progression rates to understand the considerable variance in disease course in AD. A fraction of AD patients show a rapid decline, a larger group experience an intermediate progression, but having slow disease progression may be equally, or even more, common. It has been argued that a high number of slow progressors in clinical AD studies may be due to selection of healthier participants in such studies [9]. However, a high proportion of slow progressors among AD patients was also found in a population study [6]. We believe our and similar studies deliver important background information both for patients in the symptomatic stages of the disease and for intervention studies in AD. The high proportion of slow progressors over the first two years implies a need for large study groups and/or long follow-up periods to ensure sufficient power to detect effects of interventions. Additionally, there is a need for more research to identify predictors of progression in AD and to explore whether there are biological differences that could explain the divergent disease courses.
Our study showed considerable heterogeneity in the disease course of AD patients. A similar study found that cognitive tests at baseline predicted 37% of the subsequent change in CDR-SB over three years of follow-up [26]. Although that study population was somewhat healthier, the results were similar [26], showing that lower scores on cognitive tests at baseline predicted an unfavorable disease course [9].
In the present study, the predictors included at baseline were able to explain only a small proportion (17%) of the variance in progression. We did not find any significant influence of sex, ApoE genotype, length of education, or medical history concerning other vascular risk factors or cerebrovascular disease on the disease course in AD. In the literature, a range of other factors have been examined for their potential influence on disease progression in the symptomatic phases of AD, including family history of dementia, neuropsychiatric symptoms, markers of inflammation, and functional level at baseline. The evidence for all these factors is mostly inconclusive, and even less is known about what influences progression in the preclinical phases of the disease [11, 12]. Further analyses will be performed in the PADR study focusing on other predictors for disease progression.
As in other studies, some of the study patients improved from baseline to follow-up [27], which could not be explained by depressive symptoms or the use of anti-dementia medication. It might be hypothesized that the improvement can be related to optimized treatment of comorbid disorders including withdrawal of inappropriate drugs, or it can be a consequence of test-retest variability in scores for patients who were essentially stable.
Most, but not all, studies in AD report an inverse association between the age at onset and rate of disease progression [7, 11]. In our study, older age was found to be a predictor of cognitive deterioration in the unadjusted regression analysis but could explain only a small fraction of the change in CDR-SB, and the effect of age disappeared in the adjusted analysis. Slow progressors in our study were on average younger. Studies of imaging and pathology in AD show faster evolving brain atrophy in early-onset than in late-onset AD [28], which is in contrast to our study where some of the younger patients with mild or very mild AD showed little progression. The heterogeneity of our sample regarding age and disease severity indicates that age-related comorbidities may be of importance for disease progression although this could not be shown by the analyses in the present study [29].
Although a majority of studies find that education may be a predictor of rapid cognitive decline in AD, others find no effect of education on progression [9, 11] which is in line with our findings. The mean education level in our study is relatively high compared to other clinical studies in AD. The younger patients with little progression also included many with long education. If well-educated patients and their families have an increased awareness of early AD symptoms, they may receive a diagnosis at an earlier stage, when disease progression is likely to be slow.
In contrast to some other studies, we did not find differences in CDR-SB progression rates across different stages of disease severity at baseline but were able to demonstrate such a difference for the MMSE, where the number of points lost increased with disease severity. There was also a difference in the number of slow progressors characterized by these scales, with the CDR-SB defining a higher number as slow progressors than the MMSE. This was also shown by Tschanz et al. [6] in another study using the same definitions of slow progression. The observed differences between MMSE and CDR-SB may have several explanations. While MMSE scores are known to depend on age and education [30], these factors are not known to affect the CDR-SB [31]. The MMSE is most sensitive to change in the middle to late stages of the disease [32], whereas the sensitivity of CDR-SB is not known to differ with disease severity and can also be scored for those who are unable to undergo cognitive tests. With our chosen cutoff, we defined more patients as slow progressors in IADL as compared to CDR-SB or MMSE scores. This is probably due to the psychometric qualities of the questionnaire, which may not have the necessary responsiveness to change [33].
The correlations shown between change in the CDR-SB and change in the MMSE and IADL are in agreement with two other studies with similar design [3, 4]. Notably, the correlations were stronger between CDR-SB and IADL than between CDR-SB and MMSE. This illustrates that follow-up assessments should focus both on cognition and function. Therefore we consider CDR to be the best of these tools to assess disease progression.
A strength of the present study is the relatively large sample size. In contrast to some studies assessing only patients able to attend the memory clinic, we also did follow-up assessments of patients with severe disease in nursing homes.
The major limitation of the study is that the generalizability is restricted by the inclusion criteria and the attrition rate. Memory clinic patients represent a selected population in terms of age, education level, and disease presentation, and for ethical reasons, we could not include patients with severe dementia at baseline. We have studied progression of AD among patients with MCI and mild to moderate dementia. Therefore, the results are not valid for prodromal or severe stages of the disease. There is still limited evidence on progression in preclinical AD. More research on progression in the prodromal phase is needed when designing pharmacological interventions among these patients.
It might be that we overestimate the number of slow progressors because patients with severe AD were not included, these would probably have a faster progression. Patients lost to follow-up scored lower on the Trail Making B test and may therefore have a more rapid progression. In addition, patients who died between baseline and follow-up were not included in the analyses because we did not know whether the cause of death was related to AD or to intercurrent disorders. Another limitation is the fact that we performed only one follow-up assessment, making non-linear estimates of progression impossible.
Conclusion
Although AD on a group level is a progressive disorder, we found that almost 50% of the patients had a slow or no detectable progression over two years. The results of cognitive tests at baseline were significant predictors of progression rate but could explain just a small part of the variance in progression. These results are relevant to patients, their caregivers, and society, as predicting the disease course for individual patients is important in order to plan for the future. Further, these results are important for intervention studies, as recruitment of patients who can actually be expected to experience symptom progression is essential to be able to show effect of new interventions. Further research on predictors of disease progression is important for future intervention studies and is included in coming projects by the PADR study group.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Regional Committee for Medical and Health Research Ethics for South East Norway approved the study (REC number 2011/531). All patients received oral and written information and gave written, informed consent to participate. Only patients with capacity to consent were recruited at baseline, as recommended by REC.
Footnotes
ACKNOWLEDGMENTS
The work by Rannveig S. Eldholm and Maria L. Barca was funded from the Norwegian ExtraFoundation for Health and Rehabilitation through the Norwegian Health Association. Rannveig S. Eldholm also received funding from the Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology (NTNU). Karin Persson’s work was funded by the Southern and Eastern Norway Regional Health Authority.
We thank the study participants, their caregivers, and the employees of the nursing homes for their contributions to the study. We also thank the staff in the three memory clinics in St. Olavs Hospital, Oslo University Hospital, and Innlandet Hospital for their willingness and collaboration.