
Abstract
Background:
Sundown syndrome (SS) is the onset or worsening of behavioral symptoms in the evening in patients with dementia.
Objective:
To identify the differential clinical profile of patients with dementia who present SS.
Methods:
A cross-sectional, case-control observational study was conducted by retrospectively reviewing the medical records of patients with dementia in a specialized Memory Unit. We compared the characteristics of patients with and without SS, including sociodemographic variables, etiology, and severity of the dementia, behavioral symptoms, sleep disorders (considering insomnia and hypersomnia), other diseases and treatments employed. We identified the factors related to SS and conducted a logistic regression analysis to establish a predictive nomogram.
Results:
Of the 216 study patients with dementia, 41 (19%) had SS. There was a predominance of women (2.4:1), advanced age (p = 0.0001), dependence (p < 0.0001), institutionalization (p < 0.0001), caregiver burden (p < 0.0001), anxiety (p < 0.0001), delirium (p < 0.0001), hallucinations (p < 0.0001), wandering (p < 0.0001), Lewy body dementia (p = 0.05), higher Global Deterioration Scale score (GDS; p < 0.0001), and sleep disorders (p < 0.0001). The multivariate analysis revealed that age (p = 0.048), GDS score (p = 0.01), and the presence of insomnia or hypersomnia (p < 0.0001) independently defined the presence of SS. We established a predictive nomogram for developing SS in patients with dementia, with a predictive capacity of 80.1%.
Conclusion:
In our study, age, a higher score on the GDS, and the presence of insomnia or hypersomnia are differential clinical characteristics of patients with SS. We defined a nomogram that helps predicting the occurrence of SS in patients with dementia.
INTRODUCTION
Sundown syndrome (SS), also known as sundowning, is a psychobehavioral disorder that occurs in some patients with dementia. SS consists of the onset of or an increase in behavioral problems in the late evening or during and after sunset, in the form of symptoms such as confusion, disorientation, vocalizations, anxiety, agitation, aggressiveness, and psychomotor restlessness [1]. These symptoms can be difficult to control, affecting the patient’s wellbeing and increasing the caregiver’s burden.
Despite being easily recognizable in the clinical setting, the phenomenon has no consensus in terms of diagnostic criteria, there are many doubts as to its origin and there is relatively scarce literature about it [2]. The possible causes of SS include etiologies related to circadian rhythm disorders, hormonal disorders, and physiological, pharmacological, iatrogenic, environmental, and psychological factors [3–5]. It has been hypothesized that SS might be the result of specific neuropathological abnormalities that interfere with normal circadian rhythm and behavioral regulation. An important component of circadian rhythm regulation is melatonin; a hormone secreted by the pineal gland in response to darkness, whose production and release is regulated by the suprachiasmatic nucleus itself (the major circadian pacemaker for the human body). Melatonin levels have been shown to decrease during aging and appear to be even more reduced in Alzheimer’s disease (AD) and other neurodegenerative pathologies. These findings have provided the rationale for melatonin supplementation in patients with clinical manifestations of disrupted sleep and circadian rhythm [3, 4]. On the other hand, light is the most potent cue for the circadian system, regulating the sleep-wake cycle and helping to improve nocturnal sleep. Individuals who display symptoms of SS often have more light in their rooms at night, less light exposure throughout the day, and/or dramatic reductions in light in the early evening [1]. Phototherapy has been used in patients with dementia during evening hours to reduce motor agitation and depression [2]. These disturbances related to circadian rhythms have led to the use of both treatments (melatonin and phototherapy) to decrease the symptoms associated with the phenomenon [4], and are supported by studies that monitored these rhythms [6]. However, new research findings point to the involvement of neuronal energy loss and oxidative metabolism in SS due to chronic exposure to stress as an important origin of neurobehavioral problems. The institutionalized elderly are in a chronic state of low energy due to natural aging, also provoked by a lack of adequate natural factors such as sunlight and water. This disruption of the energy circuit could alter the oxidative and inflammatory pathways, leading to neuronal damage, which can manifest as disruptive behavior [2]. Another subject of controversy refers to the appropriate treatment for this phenomenon, ranging from environmental interventions and behavioral changes to the use of acetylcholinesterase inhibitors, antipsychotics, and the aforementioned phototherapy and melatonin [3, 4]. SS also affects the progression and severity of dementia by accelerating cognitive impairment [7] and it is also associated with sleep disorders, when these disorders are related to the severity of the dementia [8].
All this evidence motivates us to better understand this phenomenon and to establish the foundations for its effective management, given the impact that the condition has on patients with dementia and their caregivers. This study therefore seeks to identify the differential clinical profile of patients with dementia and SS treated at a specialized in the diagnosis of cognitive impairment belonging to metropolitan general university hospital in Madrid, Spain. We conducted a multivariate analysis of the factors involved in the development of SS and defined a nomogram to determine the risk of presenting this disorder among patients with dementia.
MATERIALS AND METHODS
Study population
An observational, cross-sectional, case-control study was conducted through a retrospective review of the medical records of patients treated in the Memory and Cognitive Impairment Unit of University Hospital de la Princesa (Madrid, Spain) between February and April 2016, which included a total of 260 patients with cognitive impairment. The inclusion criteria were the patients’ attendance to a medical consultation during the study period and verification of the dementia clinical criteria according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) [9]. Of the total sample, 216 patients met the inclusion criteria. We also classified the patients included in the study according to the presence or absence of SS based on verification of SS in all medical reports on the patient. SS was defined as the onset or increase of behavioral symptoms in the late evening or during and after sunset, including when SS was specifically identified or when it was simply described in this way. Figure 1 presents a flow diagram that identifies the study population.

Study population.
The study data were entered into a database, complying with the confidentiality regulations according to Organic Law 15/1999 on the protection of personal data. The study protocol was approved by the corresponding Drug Research Ethics Committee. We assessed epidemiological variables, general life functioning, patterns of institutionalization, caregiver’s burden, etiology, and severity of the dementia (using Reisberg’s Global Deterioration Scale [GDS] and the Mini-Mental State Examination [MMSE] questionnaire), behavioral symptoms (referenced in Cummings’ Neuropsychiatric Inventory [NPI] scale), the presence of sleep disorders (insomnia conciliation/early morning awakening and hypersomnia), vitamin D deficiency, and other concomitant diseases (neurological, psychiatric, sensory, endocrine, metabolic, and systemic) and the treatments employed, all during the period with SS.
For the etiological diagnosis, the following criteria were used: Alzheimer’s disease (NINCDS-ADRDA) [10], vascular dementia (NINDS-AIREN) [11], frontotemporal dementia (behavioral variant of frontotemporal dementia) [12], semantic dementia and primary progressive nonfluent aphasia [13], Lewy body dementia [14], normal pressure hydrocephalus [15], dementia due to Parkinson’s disease [16], and the remaining etiologies based on the criteria of the DSM-IV [9].
In addition to these variables, patients with SS were assessed for the time when the phenomenon started in relation to sunset (based on the timing of the onset of SS recorded in the patient’s medical history and the official table of the National Astronomical Observatory of Spain for sunsets on the visit dates), the behavioral symptoms associated with the phenomenon (based on the NPI scale), the treatments employed and the percentage of responders to them (Supplementary Material 1).
Statistical method
The quantitative values were described using the descriptive statistics of the mean, standard deviation, ranges, and confidence intervals for the mean. For data that did not follow a Gaussian distribution, we used the median and interquartile range. The distributions of the categorical variables were described using absolute frequencies and percentages of distribution. We employed the chi-squared contrast test and Fisher’s exact test to detect differences between the groups. To check the relation between binary variables and ordinal level variables, we used the Cochran-Armitage trend test. The relationship between quantitative variables and group variables was determined using Student’s t-test. For cases in which we could not assume conditions of normality, we used the Mann-Whitney U test. Multivariate analysis was performed using a logistic regression model through a stepwise variable selection, indicating an entry significance level of 0.15 and a permanence of the variable in the model of 0.10. In all cases, the significance level for rejecting the hypothesis was 5%. Taking into account the variables identified in the multivariate model, we created a predictive nomogram for the presence of SS in patients with dementia [17]. The apparent and expected optimism of the model were calculated with internal validation (bootstrap iterations, 500) (Supplementary Table 1) [18, 19]. The statistical analysis was performed using the software SAS Versión 9.4. Copyright (c) 2002–2012 by SAS Institute Inc., Cary, NC, USA.
RESULTS
Of the 216 patients with dementia included in the study, 41 (19%) had SS (95% CI 13.98–24.86). At total of 18 patients (43.9%) patients clearly exhibited SS in the hours just prior to sunset; one of these patients (2.4%) also showed an additional onset at noon (around 12:00 pm). The other 23 patients (56.1%) showed a later time pattern, when sunset had already begun. Table 1 shows the sociodemographic and clinical characteristics of the included patients, for the total sample and the comparison between patients with and without SS. SS is more common among women, but without reaching statistical significance. Patients with SS were older (p = 0.0001), with a mean age of 80.49 years for those with SS versus 74.45 years for those without SS. In general, patients with SS have less educational level although without reaching statistical significance. With regard to general life, the percentage of dependent patients for basic daily life activities was higher in those with SS (63.4% versus 28%, p < 0.0001). There was also a higher rate of caregiver burden for patients with SS (43.9% versus 9.1%; p < 0.0001) and a higher percentage of formal caregivers for patients with SS (34.15% versus 14.3%; p = 0.0013). In fact, the presence of SS was associated with institutionalization (p < 0.0001).
Clinical characteristics of the assessed population and comparison between groups with and without sundown syndrome (SS)
*We excluded patients who provided no information as to their education level.
In terms of dementia severity, the mean score on the GDS was 4.9±0.8 for patients with SS and 4.2±0.9 for those without it (p < 0.0001). A semiquantitative analysis confirmed that the percentage of patients with an elevated GDS score was higher in the patients with SS (Cochran-Armitage Trend test; p < 0.0001) (Fig. 2A) and a lower mean MMSE score (Cochran-Armitage trend test, p = 0.0029) (Fig. 2B).
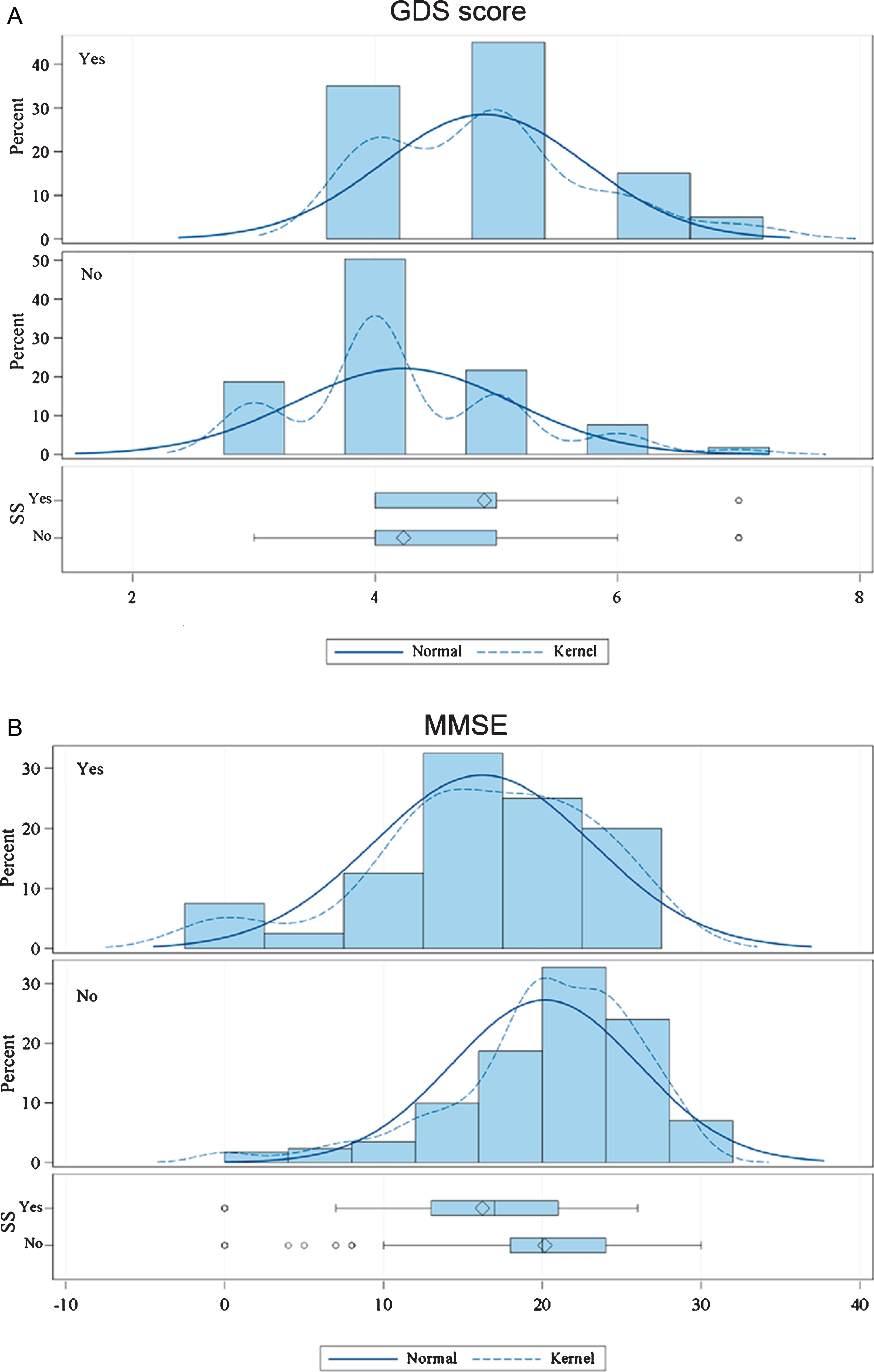
Distribution according to the study population’s score on the GDS and MMSE questionnaire, according to whether sundown syndrome (SS) was present or not.
We observed a significantly higher degree of insomnia (conciliation and/or early morning awakening) and hypersomnia among the patients with SS (Table 1).
There were no statistically significant differences in terms of vitamin D deficiency between groups. There was also no association of SS with other diseases (e.g., depression, hypoacusis, vision loss, hyperthyroidism, hypothyroidism, fibromyalgia, alcoholism, protein-calorie malnutrition). Although we found an association between SS and Parkinsonism in the neurological exploration, it did not reach significance (p = 0.07) (Supplementary Table 2).
Table 2 shows the distribution of behavioral symptoms in the total sample and separately in patients with and without SS. A higher rate of anxiety, restlessness, delirium, hallucinations, aggressiveness, and obsessive or repetitive behavior was observed in patients with SS. There were no differences in irritability, vocalizations, sadness, depression, apathy, or hypersexuality. Table 3 shows the percentages of each dementia etiologies in patients with and without SS. AD is the most common type of dementia but the most associated one with SS is Lewy body dementia (LBD) (in the statistically significant range [p = 0.05]).
Behavioral symptoms in the study population with dementia and comparison between groups with and without sundown syndrome (SS)
*Corresponds to Fisher’s exact test.
Types of dementia in the study population and comparison between groups with and without sundown syndrome (SS)
*Corresponds to Fisher’s exact test.
Table 4 shows the type of drug used in patients with dementia and the comparison between patients with and without SS. Donepezil was the most frequently used for the patients without SS (p = 0.04), whereas rivastigmine (p = 0.004), neuroleptics (quetiapine, risperidone, haloperidol) (p < 0.0001), and melatonin (p = 0.0003) were most often used for patients with SS. The combined effectiveness of the prescribed treatment in terms of controlling SS in the patients who presented it was 51.2% (95% CI 35.1–67.1). When we evaluated the relative effectiveness rate for each treatment as shown in the patient’s medical history progress, drugs that were most effective in these patients were memantine (61.1%; 95% CI 35.8–82.7), gabapentin (60%; 95% CI 14.7–94.7), and neuroleptics (57.1%; 95% CI 39.4–73.7). Nevertheless, these data should be interpreted with caution because, most of the time, multiple treatments were applied.
Drugs administered to the study population with dementia and comparison between groups with and without sundown syndrome (SS)
*Corresponds to Fisher’s exact test.
The univariate analysis identified various factors related to the presence of the SS phenomenon, including age, dependence in general life functioning, GDS score, MMSE score, presence of sleep disorders, and pattern of institutionalization (Table 5). Other related factors include taking melatonin, donepezil, rivastigmine, and neuroleptics. The possible relation between the use of some drug products and SS does not, however, imply a causal relationship. The education level, type of dementia, and vitamin D deficiency were not significant determinants of the presence of SS. Protective factors against developing SS were an age younger than 75 years, a GDS score of 3–4, and not being institutionalized. The multivariate analysis established that the variables that independently best defined the presence of SS were age, GDS score, and insomnia/hypersomnia. The regression analysis helped establishing a predictive nomogram for developing SS, taking into account the identified independent variables (Fig. 3). This nomogram establishes a total score that identifies a risk of developing SS, defined by total points between 0.2 and 0.9. This model’s predictive capacity is 80.1%, with an area under the ROC curve of 83.8% (Fig. 4).
Univariate and multivariate analyses of the factors affecting the presence of sundown syndrome (SS) in patients with dementia
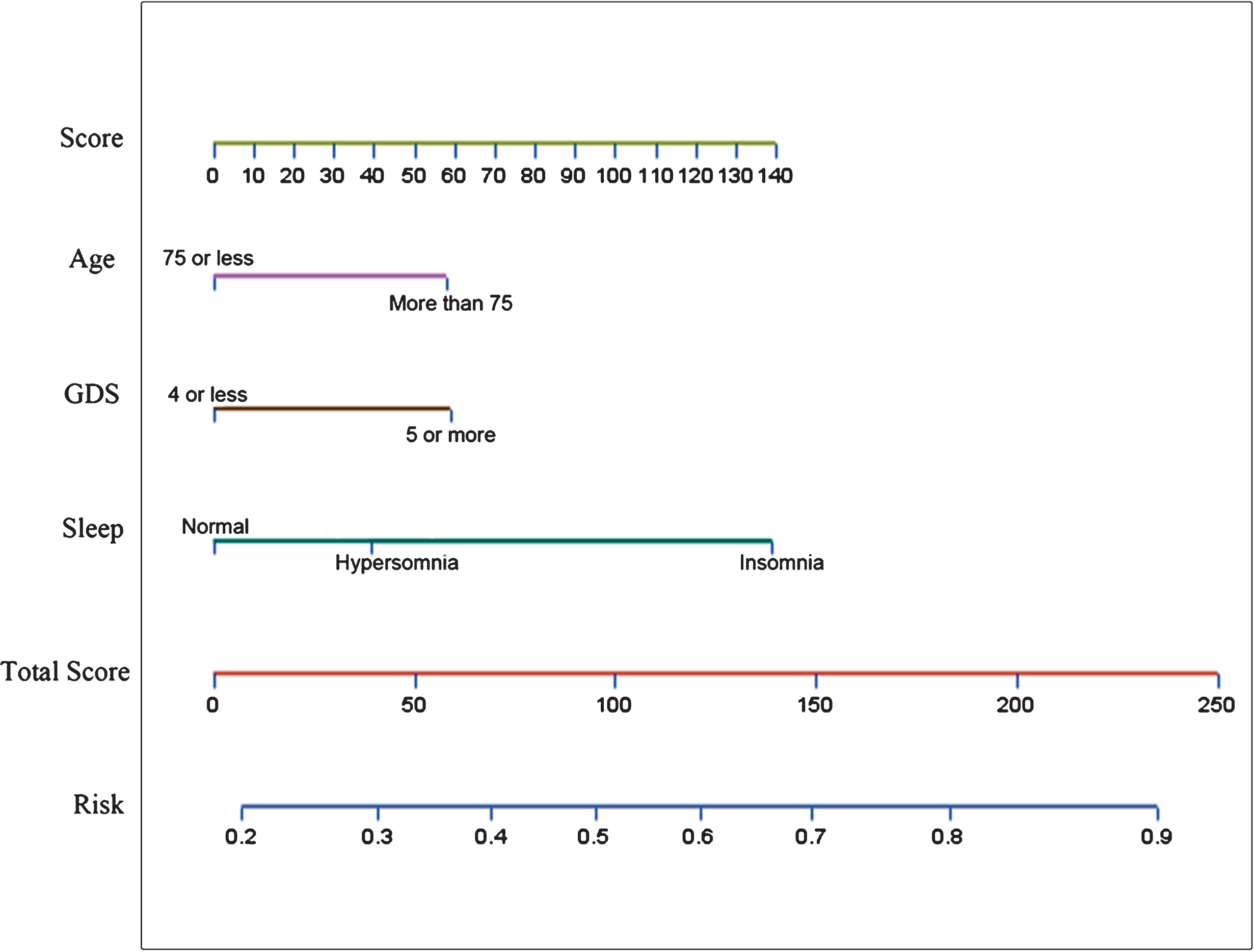
Predictive nomogram for the development of sundown syndrome (SS) in patients with dementia based on the identified independent variables.

ROC curve of the predictive model.
DISCUSSION
Neuropsychiatric symptoms in patients with dementia are common and entail a significant burden for patients and their families. The clinical approach to these types of phenomena is loaded with problems, due to the inherent individuality and the interaction between certain variables and mechanisms that hinder the clinical characterization of this process. SS is a descriptive term and not a neurological or psychiatric diagnosis. SS describes a set of neuropsychiatric symptoms that occur in elderly patients, mainly those with dementia, in the afternoon or when night begins [4]. In line with previous findings, the prevalence of SS ranges from 2.5% to 66% of patients with dementia, depending on the study design, the patients’ underlying diseases and the methods employed for the diagnosis [2, 3]. In our setting, SS occurred in almost 20% of patients with dementia attending to a specialized consultation in a hospital environment.
Approximately half of the registered patients with SS have AD, which was expected considering to the high rate of this type of dementia [20]. However, we also detected the phenomenon in with other dementia types. In our setting, we observed an association between SS and LBD. To our knowledge, this relation has not been previously reported. This finding is consistent with a greater frequency of psychotic symptoms characteristic of this pathology [21]. We also know that LBD and AD are associated with a severe sleep disorder but this alteration is different in both pathologies. While AD is characterized by fragmented nocturnal sleep, with increased awakening and reduced III/IV and REM phases, LBD has behavioral disturbances during REM sleep and periodic limb movement disorder [22]. In fact, those patient with AD and the most severe forms of SS, delayed temperature acrophases have been found, as well as a lower correlation between the circadian rhythm of temperature with the 24 h cycle and a lower amplitude of the temperature curve [6]. These findings suggest the importance of circadian rhythms in the etiopathogenesis of SS [6, 23]. Moreover, the antipsychotic drugs used in managing patients with dementia can affect circadian rhythms [24]. A better understanding of the changes in circadian activity patterns could help us understanding this phenomenon and improving its clinical and therapeutic management.
With regard to the clinical characterization of SS, there is a greater presence of this phenomenon among female and older patients. These patients’ educational level is an inconclusive epidemiological datum. The data regarding general life functioning, type of caregiver and institutionalization were related to the already known predisposing factor of having SS, which represents the severity of the cognitive impairment [3, 4]. We confirmed greater dependence for basic activities of daily life and a greater presence of formal caregivers and institutionalization for the patients with SS. All of this involves greater overload for the caregiver, as already routinely described among these types of patients and their relatives [4, 25]. Agitation in these patients has been related to the cause of their institutionalization [4]. Based on our data, however, we cannot confirm that SS is the direct cause of institutionalization for patients with SS in that situation in our study.
We should emphasize the importance of the association between the severity of the dementia and the presence of SS [3, 4]. This finding was confirmed in our study, through the patients’ GDS and MMSE questionnaire scores. In fact, this phenomenon is predominantly concentrated in GDS4 and GDS5 (mainly the latter), resulting from moderate and moderate-severe cognitive impairment and with greater frequency than in cases of severe or highly severe cognitive impairment. The study design also does not help us determine whether the SS is also related to faster deterioration of the dementia. If this is the case, the SS itself could be used as a marker of frailty, as suggested by others studies [7, 26].
The relationship between SS and the presence of sleep disorders, such as insomnia and hypersomnia, was a determinant variable in our analysis. Although the most commonly reported disorder was insomnia [6, 23], both were established as independent risk factors. As described above, the circadian rhythm is responsible for regulating the sleep/wake cycle, enabling nighttime rest, and it is frequently altered in elderly institutionalized patients [27]. Recent lines of research have suggested an especially interesting relationship between reductions in sleep and the development of neurodegenerative diseases through a lymphatic system dysfunction [28]. These findings could explain the role of insomnia as a risk factor for dementia and a determinant of its severity and not only a consequence of dementia [23, 29]. The relationship between hypersomnia and SS is even less understood, although it could also be based on circadian rhythm impairment, which provokes daytime drowsiness and increased nighttime activity [4]. The use of neuroleptics and anxiolytics in patients with SS represents without a doubt another confounding factor.
We studied the possible relation between SS and vitamin D deficiency in our patients with this phenomenon, considering the possible relationship between the phenomenon and reduced light exposure, previously suggested among the environmental factors identified by other authors [1, 2]. Anyway, in our study, we did not obtain results in favor of this possible hypothesis. Due to the retrospective nature of the study, we were unable to assess other environmental factors, such as increased fatigue after daytime activity and excessive environmental stimulation (noises or untidiness). However, there are studies that suggest an association between these factors with the pathophysiology of SS [3, 4]. We also did not detect a relation between SS and other concomitant diseases. In fact, we did not confirm the potential associations suggested in other studies regarding hearing loss, vision loss, and pain [3]. There was an interestingly high prevalence of depression among the study patients with dementia (1 out of 3), although this finding was not associated with the presence of SS in our environment. Other authors have suggested a worsening of mood in the late afternoon among patients with major depression, which could be identified as a cause of SS [4].
From a clinical point of view, we detected a set of behavioral symptoms whose onset or exacerbation was associated with SS, including anxiety, restlessness, delirium, hallucinations, aggressiveness, and obsessive and repetitive behavior. In contrast, we observed apathy more frequently among patients with dementia without SS, although this finding did not reach statistical significance. The detected symptoms are consistent with those identified by other authors, including confusion, disorientation, wandering, vocalizations, anxiety, agitation, aggressiveness, and psychomotor restlessness [1, 4]. The most differential behavioral symptom in this series among those already described is possibly the presence of obsessive and repetitive behavior, a disorder that is common in the psychological sphere of these patients. Some examples observed in our series would be: ordering and accumulating objects, verifications, and recurring religious or sexual ideas.
In this study, we did not attempt to show causal relationships for the onset of SS and treatment patterns for the patients with dementia, although the high use of neuroleptics in the patients with SS compared with those not affected by this phenomenon is worth noting. It is also noteworthy that rivastigmine was more used than donepezil in patients with SS. This greater use of rivastigmine for LBD could be related to the greater evidence for effectiveness in managing cognitive and neuropsychiatric symptoms in this type of dementia [30] and to a greater use of the drug (in transdermal patch form) for treating AD with pronounced behavioral impairment, based on its better therapeutic adherence [31]. The use of melatonin is greater in these patients than in patients without SS, because it represents a recurring treatment for the phenomenon due to its theoretical etiological relationship with the hormone disorder in SS [32].
Given that this was a descriptive retrospective study, it was also not possible to correctly assess the effectiveness of the treatments. However, according to the data recorded in the medical history, we observed that the relative effectiveness of memantine, gabapentin, and neuroleptics (quetiapine, risperidone, and haloperidol) was apparently greater in controlling the process. Neuroleptic drugs have recognized effectiveness in controlling limiting behavioral symptoms, particularly when faced with the failure of nonpharmacological strategies. However, this effectiveness is questioned by several studies and is a subject of debate due to the high simultaneous risk of adverse effects [33, 34]. Continuous monitoring should always be conducted when using these drugs [35]. Among the antiepileptic drugs, low doses of gabapentin are used to try to control agitation and aggressiveness in patients with dementia when this is refractory to other treatments or has adverse effects [36, 37]. Memantine shows evidence of effectiveness in reducing fragmented sleep and improving behavioral and psychological symptoms in patients with AD [38]. The use and effectiveness of gabapentin and memantine is new to SS in the scientific literature, but however it makes sense to be considered, as described above, both can be effective in patients with behavioral disturbances and dementia. Further studies specifically designed to understand the effectiveness of this type of treatment in patients with dementia and SS are needed. The acetylcholinesterase inhibitors in this study did not appear to be more effective than other drugs, although they are used to improve cognitive function, behavioral symptoms, and SS, especially in LBD [3, 4]. Also worthy of note is the scarce relative effectiveness of melatonin in our experience, despite the fact that this is the only drug for which randomized clinical trials in patients with SS have been performed; however, these studies have shown inconclusive and conflicting results [39–41]. We lack data on the use of light and hydration therapies, when faced with the possible relationship between SS and the loss of neuronal energy and oxidative stress proposed by new lines of research [2].
The regression analysis showed that the patient’s age, degree of cognitive impairment evaluated by the GDS, and the presence of sleep disorders (insomnia and hypersomnia) were independent factors that predicted the onset of SS in patients with dementia. Other related elements, such as sex, the use of various drugs and institutionalization (either in a hospital or day care center), were not independent predictors of the onset of SS. With these data, we established a risk model that helps define a nomogram for patients with dementia. This nomogram has a high predictive capacity but should be validated in an independent series of patients with dementia to confirm its clinical usefulness.
This study’s limitations include its retrospective character and the fact that the information was obtained from the patients’ medical history. Therefore, in some cases, the data could be incomplete, especially considering the severity of the cognitive deficit in many of these patients. The relative effectiveness of the treatments was recorded by the physician who treated the patient, and this was not based on predefined variables. Nevertheless, having been implemented in a specific memory and cognitive impairment unit, the evaluated data were highly reliable and were recorded by a limited number of experienced practitioners. Another important consideration is that the patients did not undergo polysomnography to confirm the presence of insomnia or hypersomnia or to assess other disorders that could have been relevant, such as restless leg syndrome or REM sleep behavior disorder.
Conclusion
SS is a neuropsychiatric disorder, which is not uncommon to find in patients attended in a Memory Unit, particularly in those who suffer from dementia. After completing our study, we can report a possible differential clinical profile for patients with dementia and SS. We detected that age, a higher score on the GDS, and the presence of insomnia or hypersomnia were independent predictors for developing SS. The nomogram we developed could help clinicians detecting patients with a greater risk of presenting the phenomenon.
SS is associated with greater caregiver burden and increased patient institutionalization. Early recognition of SS after a directed case history review and subsequent early treatment can greatly improve the patients’ and caregivers’ quality of life.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/17-0488r3).