
Abstract
Background:
Anticholinergic challenge can induce odor identification impairment that indicates Alzheimer’s disease pathology.
Objective:
To determine if decline in odor identification ability with anticholinergic challenge can predict improvement with donepezil, a cholinesterase inhibitor (ChEI), in patients with mild cognitive impairment (MCI).
Methods:
At baseline, the University of Pennsylvania Smell identification Test (UPSIT) was administered before and after an anticholinergic atropine nasal spray challenge. Donepezil was started at 5 mg daily, increased to 10 mg daily if tolerated, and then the dose was kept constant for 52 weeks. Main outcomes were change in Selective Reminding Test (SRT) total immediate recall and ADAS-Cog total score from baseline to 26 and 52 weeks.
Results:
In 37 participants, mean age 70.4 (SD 9.8) y, greater atropine-induced decrease in UPSIT score at baseline was associated with greater improvement in SRT total recall score from baseline to 26 and 52 weeks (p < 0.03). This effect remained after adjusting for time, age, education, gender, APOE ɛ4 status, and baseline cognitive score (p < 0.05). Decrease in UPSIT score was associated with global improvement (CIBIC-plus) over 52 weeks (p < 0.02). After excluding patients with congential anosmia, increase in UPSIT score from 0 to 8 weeks showed a trend-level association with improvement on the ADAS-Cog (p = 0.07).
Conclusions:
Anticholinergic challenge-induced odor identification decline was associated with cognitive improvement, and short-term improvement in odor identification tended to predict longer term cognitive improvement. These simple inexpensive strategies have the potential to improve selection of patients with MCI for ChEI treatment.
INTRODUCTION
Neurofibrillary tangles develop in the olfactory bulb in early pathological stages of Alzheimer’s disease (AD) [1 –3]. Odor identification impairment in AD reflects pathology in the olfactory bulb and olfactory projection areas, including the anterior olfactory nucleus, piriform cortex, amygdala, entorhinal cortex, hippocampus, and orbitofrontal cortex [4, 5]. In mild cognitive impairment (MCI), odor identification impairment demonstrates utility similar to episodic verbal memory impairment in predicting the transition from MCI to the clinical diagnosis of AD [6 –8] and for the transition from cognitively normal to MCI [8, 9].
Neurons and synapses that use acetylcholine are damaged in AD [10]. Neurons with choline acetyltransferase are detected in all olfactory bulb layers [11, 12], cholinergic synapses are concentrated on dendrites of olfactory periglomerular or granule cells [11], and olfactory bulb function is enhanced by acetylcholine and impaired by anticholinergic agents [11, 13]. In mice, treatment with donepezil, a cholinesterase inhibitor (ChEI), rescues medial septal cholinergic neurons from neurodegeneration induced by olfactory bulbectomy [14]. Olfactory bulb cholinergic receptors are mainly muscarinic [15].
In a preliminary study of patients with AD, donepezil treatment was associated with improvement in odor identification and improvement in global functioning [16]. In another pilot study, impaired odor identification was associated with improved episodic verbal memory after donepezil treatment in depressed patients with MCI [17]. Therefore, odor identification impairment may help to identify which patients with MCI will benefit from ChEI treatment. In another report, greater worsening in odor identification test performance following an intranasal challenge with atropine correlated with left hippocampal volume and was associated with the apolipoprotein E (APOE) ɛ4 genotype [18].
In a preliminary open-label trial in MCI, we examined the acute decrease in odor identification scores induced by an intranasal atropine challenge to block cholinergic transmission, and increase in these scores from baseline to 8 weeks, as predictors of cognitive improvement over one year of ChEI treatment.
METHODS
Participants
Patients were recruited for this IRB-approved study from the Memory Disorders Center at the New York State Psychiatric Institute/Columbia University Medical Center and by advertising in local media. Inclusion criteria were age 55–95 years and diagnosis of amnestic MCI based on the presence of subjective memory complaints, score >1.5 SD below norms on either the WMS-III Logical Memory subtest immediate or delayed recall, or the Free and Cued Selective Reminding Test (FC-SRT) immediate or delayed recall [19], and without functional impairment consistent with dementia. Patients with amnestic MCI, either solely amnestic or amnestic with additional cognitive domain deficits, were included. Other inclusion criteria were Folstein Mini-Mental State Exam (MMSE) ≥ 23/30 [20], Clinical Dementia Rating (CDR) score of 0.5 [21], and availability of an informant.
Exclusion criteria included current use of cholinesterase inhibitors, history of intolerance or contraindication to donepezil, and use of medications with anticholinergic properties including diphenhydramine, tricyclic antidepressants, and antipsychotics. Other exclusion criteria were specific neurological disorders including Parkinson’s disease, multiple sclerosis, stroke with residual neurological deficits, psychotic disorders including schizophrenia, bipolar disorder and schizoaffective disorder, alcohol/substance dependence in the past 6 months, and current major depression. Benzodiazepine use in lorazepam dose equivalents less than 1 mg daily was permitted. Exclusion criteria for olfaction testing were current smoker >1 pack daily, current upper respiratory infection, nasal trauma or sinus surgery, and head trauma with loss of consciousness.
The screening visit comprised a medical, psychiatric, and neurological evaluation, cognitive assessment to determine inclusion criteria, and blood draw for hematocrit, electrolytes, liver, kidney and thyroid function tests, folate and vitamin B12 levels, and urinalysis to exclude primary medical causes of cognitive impairment.
The subsequent baseline (week 0) visit involved assessment with the two main cognitive outcome measures: Alzheimer’s Disease Assessment Scale-Cog (ADAS-Cog, 11-item version) [22] and 12-item 6-trial Selective Reminding Test (SRT) [23]. For diagnostic purposes, neuropsychological tests in the National Alzheimer’s Coordinating Center-Uniform Data Set (NACC-UDS) battery were administered: Wechsler Memory Scale (WMS)-III digit span forward and backward, Wechsler Adult Intelligence Scale-Revised (WAIS-R) digit symbol, Trail Making A and B, verbal fluency for controlled word association using the letters C, F, and L and animal, vegetable and fruit list generation, and Boston Naming Test (60 items). The study physician completed the NACC clinical assessment, Clinician’s Interview Based Impression of Change-plus (CIBIC-plus) and Clinician Interview Based Impression of Severity (CIBIS) global assessment ratings, CDR, and the Treatment Emergent Symptoms Scale (TESS) that evaluates 26 somatic side effects. An informant completed the Pfeffer Functional Activities Questionnaire (FAQ). APOE genotyping was conducted at Prevention Genetics, a reference laboratory.
The University of Pennsylvania Smell Identification test (UPSIT) was administered. This standardized scratch and sniff test consists of 40 booklet pages with a single odor embedded in a microcapsule on each page. Scratching with a pencil releases the odor and one of 4 choices is checked, e.g., chocolate, banana, onion, fruit punch. The total UPSIT score ranges from 0 (all incorrect) to 40 (all correct). Immediately following UPSIT administration, atropine 1 mg, with the dose divided approximately equally between the two nostrils, was administered using the “squirt system” [24]. The patient then assumed the “Mecca” position for 2 minutes to ensure that the atropine crossed the cribriform plate into the olfactory bulb [18]. The UPSIT was repeated 45 min later to ensure sufficient time for the atropine effect.
Research assessments were repeated at 8, 26, and 52 weeks with the exception of the diagnostic neuropsychological battery that was repeated only at 26 and 52 weeks. At baseline, donepezil was started at 5 mg daily followed by assessment at 4 weeks for tolerability before increasing the dose to 10 mg daily. This dose was kept constant for the rest of the 52-week study. Patients who could not tolerate donepezil 10 mg were maintained at 5 mg; if the 5 mg dose could not be tolerated the patient was switched to galantamine or rivastigmine. Nine patients received galantamine or rivastigmine during the trial; their data were combined with donepezil data for analysis. Two experienced raters (Drs. Devanand and Pelton) made a consensus diagnosis at baseline and 52 weeks blind to scores on predictor (UPSIT) and cognitive outcome (ADAS-Cog total score and SRT total immediate recall) measures. The study physician completing the CIBIC-plus and CIBIS also remained blind to these measures.
The main hypotheses were that the acute decrease in UPSIT scores from pre- to post-atropine nasal spray challenge, which indicates greater cholinergic deficiency, would be associated with cognitive improvement on donepezil from baseline to 26 weeks and 52 weeks, and that the increase in UPSIT scores from baseline to 8 weeks (improved olfaction ability on donepezil) would be associated with cognitive improvement from baseline to 26 and 52 weeks. Conversion to the clinical diagnosis of dementia based on CDR and consensus diagnosis, as well as changes in the CIBIC-plus and FAQ, were secondary outcomes examined in exploratory analyses.
Statistical analyses
Variables measured at baseline were summarized using means and standard deviations for continuous measures and percentages for categorical measures. Hypotheses were assessed using linear mixed effects models with a random intercept for each subject. In each model the response was change in cognitive score (either ADAS-Cog or SRT total immediate recall) from baseline. All models included the covariates of time (a binary indicator of whether the change in score was a change from baseline to 26 or 52 weeks), change in UPSIT (either acute change after atropine challenge or from baseline to 8 weeks), and baseline score (either SRT total immediate recall or ADAS-Cog). History of smoking (n = 16, 43%) was not associated with UPSIT scores and was not included as a covariate. There were 2 current smokers who each smoked less than 1 pack daily. Models that additionally adjusted for age, education, gender, and APOE ɛ4 status were also evaluated. With the models parametrized in this way, the parameter for the time effect corresponds to the adjusted mean difference between change score at week 52 and change score at week 26, while the parameter for the change in UPSIT score corresponds to an adjusted mean increase or decrease in cognitive change score (either ADAS-Cog or SRT total immediate recall) for a one point increase or decrease in change in UPSIT. All subjects with at least one outcome measure available post-baseline were included in the analysis. For the exploratory analyses, we fit similar mixed effects models for the change in FAQ and CIBIC-plus outcomes while generalized linear fixed effects models with a cumulative logit link were employed for the change in CDR outcome. Models for CIBIC-plus adjusted for baseline MMSE; there was no baseline for the CIBIC-plus change score. For the secondary outcomes of change in executive function score (Trail Making B time minus Trail Making A time) and change in WAIS-R digit symbol score, both measured only at baseline and week 52, we used linear regression models, adjusting for the same covariates as above, except for time.
Before testing the specified hypotheses, we examined whether the effect of change in UPSIT score (either acute pre-post atropine challenge at baseline or over 8 weeks) on cognitive change score depended on time by including an interaction term consisting of the product of time and change in UPSIT score in each model. No interactions were significant, thus supporting direct testing of the study hypotheses. A level of 0.05 was used as the threshold for significance. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC), and we used PROC GLIMMIX for fitting all mixed effects models.
RESULTS
Of 175 individuals assessed for eligibility, 118 did not meet inclusion/exclusion criteria and 15 who met criteria declined to participate. Of 41 patients who signed consent, 4 patients withdrew consent and 37 patients completed baseline evaluation. Of these 37 patients, 32 completed the 52-week study (3 could not be contacted and 2 refused to return to clinic). Complete baseline data were available for 37 patients (Table 1 and Fig. 1). The ethnic breakdown was White 20, African-American 12, Hispanic 1, Asian 1, mixed race 2, and other race 1. Mean age was 70.35 (SD 9.76) years, 54.05% were male, mean education was 15.86 (SD 3.64) years, and the APOE ɛ4 allele was present in 38.9% of patients. At baseline three patients were taking benzodiazepines and at week 52 one patient was taking a benzodiazepine, all at lorazepam equivalent dose ≤ 1 mg daily. Mean baseline UPSIT score was 26.81 (SD 7.43). Cognitive performance improved over 52 weeks of ChEI treatment with a decrease in ADAS-Cog scores and an increase in SRT total recall scores (ps < 0.01 from paired t-tests). ADAS-Cog score changed from 10.67 (SD 4.15) at baseline to 10.27 (SD 3.83) at 8 weeks, 8.80 (SD 3.69) at 26 weeks, and 10.09 (SD 4.68) at 52 weeks. SRT-total recall score changed from 33.61 (SD 8.15) at baseline to 36.23 (SD 9.27) at 8 weeks, 36.81 (SD 9.22) at 26 weeks, and 37.13 (SD 10.59) at 52 weeks. Baseline UPSIT score was not associated with changes in either ADAS-Cog or SRT total recall.
Baseline characteristics of patients with mild cognitive impairment (n = 37)
ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognitive (11 items, higher scores indicate worse cognitive performance); SRT, Selective Reminding Test 12-item 6-trial version (higher scores indicate better cognitive performance); UPSIT, University of Pennsylvania Smell Identification test (40 items, range 0-40).
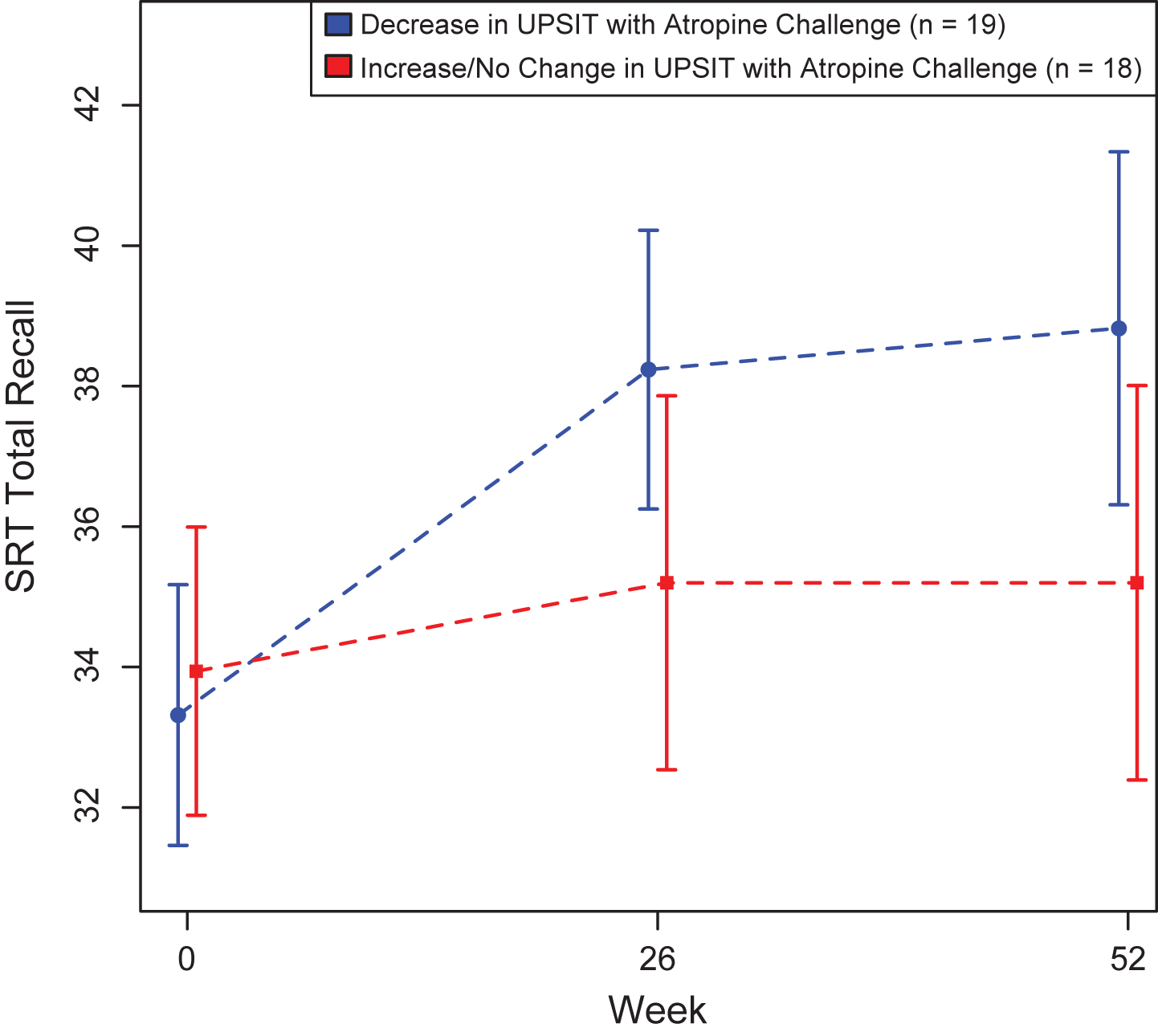
Mean Selective Reminding Task (SRT) total score over the 52-week trial grouped by type of change in the University of Pennsylvania Smell Identification Test (UPSIT) with atropine challenge.
Acute decrease in UPSIT scores with atropine challenge
From pre- to post-atropine challenge, UPSIT scores decreased an average of 0.32 (SD 3.84) points. Figure 1 shows the raw mean SRT Total recall scores at 0, 26 and 52 weeks stratified by whether UPSIT score after atropine challenge decreased (blue) or increased/remained the same (red).
Greater decrease in UPSIT score from pre to post-atropine challenge was associated with greater increase in SRT total recall score from baseline to 26 weeks and 52 weeks (F1,30 = 5.41, p < 0.03; Fig. 1). This effect remained significant after adjusting for covariates (F1,30 = 4.54, p < 0.05). This model suggests that a one-point greater decrease in UPSIT score corresponds to a 0.58 point greater increase in SRT total recall score (greater improvement) on average, adjusting for covariates. In the entire sample, APOE ɛ4 status was not a significant predictor of change in SRT total recall score in the adjusted model (F1,30 = 1.00, p = 0.32).
The acute change in UPSIT score (post-pre) was not associated with change in ADAS-Cog from baseline to 26 weeks or 52 weeks (F1,30 = 0.47, p = 0.50). Similar results held after adjusting for age, sex, education, and APOE ɛ4. APOE ɛ4 allele positive status was associated with improvement in cognition measured by a greater decrease (greater cognitive improvement) in ADAS-Cog scores (F1,29 = 4.26, p < 0.05), adjusting for change in UPSIT with atropine challenge and the other covariates.
Greater decline in UPSIT scores with atropine challenge was associated with improvement in CIBIC-plus scores over 52 weeks (F1,30 = 6.43, p < 0.02), and this effect remained significant after covariate adjustment (F1,30 = 6.22, p < 0.02). Greater decrease in UPSIT scores with atropine challenge was associated with improvement in executive function score over 52 weeks adjusting for baseline difference between Trail Making B time and Trail Making A time, age, sex, education, and APOE ɛ4 (F1,25 = 4.81, p < 0.04). Change in UPSIT scores with atropine challenge was not associated with change in WAIS-R digit symbol score over 52 weeks (F1,25 = 2.09, p = 0.16).
Change in UPSIT scores from 0 to 8 weeks
From baseline to week 8, UPSIT scores decreased an average of 0.35 (SD 4.38) points. Change in UPSIT score from 0 to 8 weeks was not associated with change in SRT total recall (F1,30 = 0.14, p = 0.71) or CIBIC-plus scores (F1,30 = 0.23, p = 0.63) from baseline to 26 weeks and 52 weeks for the total follow-up sample. Greater increase in UPSIT score from 0 to 8 weeks was not associated with change in ADAS-Cog from baseline to 26 and 52 weeks after adjusting for age, sex, education, APOE ɛ4 status, and time (F1,29 = 2.04, p = 0.16). After exclusion of patients with congential anosmia with UPSIT score <14 (n = 4), there was a trend-level association (F1,28 = 3.68, p = 0.07), adjusting for the same covariates in both analyses [25]. For patients with UPSIT score ≥ 14, a one-point greater increase in UPSIT score from baseline to week 8 corresponds to a 0.29 point greater decrease in ADAS-Cog (cognitive improvement) at 26 and 52 weeks on average, adjusting for age, sex, education, APOE ɛ4 status, and time.
APOE ɛ4 status was not a significant predictor of change in SRT total recall in the adjusted model (F1,30 = 0.66, p = 0.42). APOE ɛ4 allele positive status was associated with improvement in cognition measured by a greater decrease in ADAS-Cog scores (F1,29 = 4.67, p < 0.04), adjusting for change in UPSIT from 0 to 8 weeks, age, sex, education, and time.
Change in UPSIT score from 0 to 8 weeks also was not associated with change in executive function (F1,25 = 0.02, p = 0.89) or WAIS-R digit symbol score (F1,25 = 1.74, p = 0.20) from baseline to 52 weeks. Similar results held after the exclusion of individuals with UPSIT scores <14 [25], adjusting for the same covariates in each of these analyses. When the sample was restricted to patients who received donepezil only (n = 23), the results from the main analyses were in the same directions though not statistically significant, perhaps due to reduced sample size.
We also fit separate sets of linear regression models with either change in the cognitive measure from baseline to week 26 as the outcome or change in the cognitive measure from baseline to week 52 as the outcome, using the same covariates as the mixed effects models but without time as a covariate. The magnitudes and directions of the adjusted association between change in UPSIT (either acute or over 8 weeks) and change in cognitive score (either ADAS-cog or SRT) were consistent across the separate models and consistent with those from the mixed effects models.
Functional impairment and diagnosis of dementia
FAQ score at baseline was not significantly associated with change in UPSIT scores, either with the atropine challenge or from 0 to 8 weeks. Of the 32 patients followed for 52 weeks, based on consensus diagnosis, 24 patients remained at a CDR score of 0.5 (questionable dementia), 4 improved to CDR 0 (12.5%), and 4 declined clinically to meet a diagnosis of dementia (12.5%). All 4 patients with dementia were diagnosed with probable AD. The UPSIT predictor measures were not associated with the outcome of dementia or AD. Analyses were limited by the small number of patients with these diagnoses. TESS scores, defined by the sum score of 26 possible physical side effects, decreased over time from 2.19 (SD 2.12) at baseline to 1.59 (SD 1.37) at 26 weeks and 1.47 (SD 1.80) at 52 weeks. There were no adverse effects of intranasal atropine reported or observed in any patient.
DISCUSSION
The decrease in odor identification test scores with the atropine challenge was associated with improved SRT total recall and improvement in CIBIC-plus scores but not with improvement in the ADAS-Cog. Cholinergic transmission is a key element underlying memory function [14, 18]. The association between the atropine-induced decrease in odor identification test scores and improvement in episodic verbal memory over 52 weeks suggests that patients with MCI who have a cholinergic deficit with incipient AD are more sensitive to the anti-cholinergic effects of atropine nasal spray and that memory test performance is more likely to improve with donepezil treatment. Evaluating olfactory function with this challenge procedure may have utility in predicting improvement in memory with ChEI treatment, but larger studies are needed before it can be recommended for clinical use as a predictor of improvement with ChEI treatment.
The increase in UPSIT scores during 8 weeks of ChEI treatment was associated with improvement in ADAS-Cog test performance at trend-level when patients with low scores consistent with congenital anosmia were excluded. The finding of cognitive improvement on donepezil being greater in patients with the APOE ɛ4 allele is consistent with the large-scale donepezil-vitamin E study in MCI in which APOE ɛ4 positive patients showed the strongest response to donepezil [26]. The findings here suggest that the predictive utility of odor identification deficits for improvement with ChEI may apply particularly to patients with MCI who have the APOE ɛ4 allele.
It is difficult to identify which patients are experiencing benefit from ChEI treatment because of the small effect size of treatment and lack of impact on the longer term clinical course in MCI, where trials have been negative [26, 27]. Heightened olfactory impairment in response to intranasal atropine may be a better marker of underlying AD pathology in patients with MCI than olfactory test performance alone. If replicated in a larger sample, change in odor identification test performance with anticholinergic challenge may improve the selection of patients who receive clinical treatment with ChEI and avoid needless exposure to an ineffective ChEI with the risk of side effects in patients without AD brain pathology.
There were limitations to this study. Effects were not strong, and this may be related to the limited efficacy for ChEI in these patients. Improvement in memory scores may have been related to practice effects, particularly in patients without AD pathology and who were less likely to decline cognitively. Larger studies, especially placebo-controlled studies, that can account for practice effects are needed [28]. Odor identification impairment is not specific to AD and occurs in Parkinson’s disease, dementia due to Lewy bodies, schizophrenia, and other conditions [29]. In patients with Lewy body dementia, improvement with ChEI treatment has been demonstrated but its association with impaired odor identification has not been studied in a clinical trial [30].
Olfactory deficits are related to the presence of neurofibrillary tangles in both the olfactory bulb and olfactory projection pathways to limbic structures. Cerebrospinal fluid assessment of tau and p-tau levels, and tau imaging using PET, can estimate the degree of tau pathology and potentially the response to anti-tau treatments. Evaluation of anticholinergic challenge-induced odor identification decline, and short-term improvement in odor identification, may provide cost-effective alternatives or possible incremental benefit to the use of these expensive and invasive biomarker assessments. More broadly, these olfactory measures may be useful predictors in clinical trials of other agents in MCI, and AD, because the presence of odor identification impairment is an indicator of underlying AD brain pathology and the severity of this olfactory impairment is related to the severity of cognitive deficits and dementia [29, 31].