
Abstract
Background:
Alzheimer’s disease (AD) biomarkers are emerging as critically important for disease detection and monitoring. Most biomarkers are obtained through invasive, resource-intense procedures. A cognitive marker, intra-individual cognitive variability (IICV) may provide an alternative or adjunct marker of disease risk for individuals unable or disinclined to undergo lumbar puncture.
Objective:
To contrast risk of incident AD and mild cognitive impairment (MCI) associated with IICV to risk associated with well-established biomarkers: cerebrospinal fluid (CSF) phosphorylated tau protein (p-tau181) and amyloid-β 42 (Aβ42) peptide.
Methods:
Dispersion in cognitive performance, IICV, was estimated with a published algorithm, and included Trail Making Test A and B, Rey Auditory Verbal Learning Test (RAVLT), and the American National Adult Reading Test (ANART). CSF biomarkers were expressed as a ratio: p-tau181/Aβ42, wherein high values signified pathognomonic profiles. Logistic regression models included longitudinal data from 349 Alzheimer’s Disease Neuroimaging Initiative (ADNI) participants who completed lumbar puncture. All subjects were cognitively healthy (n = 105) or diagnosed with MCI (n = 244) at baseline. We examined odds of conversion associated with baseline elevations in IICV and/or ratio of CSF p-tau181/Aβ42.
Results:
When included in models alone or in combination with CSF p-tau181/Aβ42, one standard IICV unit higher was associated with an estimated odds ratio for incident AD or MCI of 2.81 (95% CI: 1.83–4.33) in the most inclusive sample, and an odds ratio of 3.41 (95% CI: 2.03–5.73) when restricted to participants with MCI. Iterative analyses suggested that IICV independently improved model fit even when individual index components were included in comparative models.
Conclusions:
These analyses provide preliminary support for IICV as a marker of incident AD and MCI. This easily-disseminated, non-invasive marker compared favorably to well-established CSF biomarkers
Keywords
INTRODUCTION
As the prevalence of Alzheimer’s disease (AD) rises, strategies to address the disease have shifted toward prevention, targeting the disease when it is active but pre-symptomatic [1]. Effectively monitoring AD in preclinical phases requires the use of disease biomarkers. Among the most promising biomarkers are cerebrospinal fluid (CSF) levels of phosphorylated tau protein (p-tau181), amyloid-β 42 (Aβ42) peptide, or the ratio of these analytes (e.g., p-tau181/Aβ42). Although CSF analytes are considered among the most direct measures of the disease’s hallmark neuropathological features [2–4], collection of CSF biomarkers is invasive and aversive to many potential research participants, driving a need to develop non-invasive, convenient markers[5, 6].
We recently demonstrated a relationship between a potential cognitive marker of preclinical disease, intra-individual cognitive variability (IICV), and another robust neuroimaging biomarker, longitudinal hippocampal volume loss (HVL) [7]. The proposed cognitive marker represents the within-person standard deviation across cognitive tests completed during a single session. This approached used by Holtzer et al. [8] is grounded on the principle put forward by many others [9–16] that a high level of within-person cognitive variability is a marker of brain pathology.
Like Holtzer et al. [8], our approach to estimating IICV emphasizes detection of differences in cognitive performance across domains measured in a single assessment. We selected indices which could be expected to diverge early in dementia due to AD. For example, performing poorly on executivefunctioning tasks (e.g., Trail Making Test B) in the context of a strong performance on a simple attentional task (e.g., Trail Making Test A) would suggest that an individual is exhibiting executive dysfunction unrelated to simple processing speed and visual scanning [17]. A disparity in performance between the tests would identify someone with very early executive dysfunction yet well-preserved sensory motor abilities, as is typically observed in early AD.
Adding to other investigations of IICV and risk for dementia [8–11, 14], we found that IICV predicted incident AD and mild cognitive impairment (MCI) similar to HVL and Apolipoprotein E (APOE) ɛ4 status [7]. Similarly, using data from the Wisconsin Registry for Alzheimer’s Prevention (WRAP), we noted IICV measured in a younger, i.e., middle-aged cohort, predicted incident cognitive decline occurring approximately a decade later [18].
In the present analysis of Alzheimer’s Disease Neuroimaging Initiative [19–21] (ADNI) data, we contrasted associations of IICV and p-tau181/Aβ42 to incident AD and MCI. Consistent with our overall goal to examine the utility of a non-invasive, easily implemented alternative strategy to traditional biomarkers, we hypothesized that IICV would compare favorably to an established biomarker of underlying AD pathology, i.e., p-tau181/Aβ42. Secondly, using a larger sample of ADNI participants, not limited to those with CSF analyte data, we examined whether individual IICV predicted risk of conversion over and above the individual components of IICV, hypothesizing that IICV would survive a stepwise backward selection analysis, comparing the summary index to its individual components.
MATERIALS AND METHODS
Study design
In an ex-post facto designed analysis, cross-sectional measurement of IICV and p-tau181/Aβ42 were used to predict our primary longitudinal outcome: conversion from cognitive health to MCI or AD, or from MCI to AD.
Description of ADNI
Data used in the preparation of this article were obtained from the ADNI database (http://adni.loni.usc.edu). The ADNI was launched in 2003 as a public-private partnership led by Principal Investigator Michael W. Weiner, MD. The primary goal of ADNI is to test whether serial magnetic resonance imaging (MRI), positron emission tomography (PET), other biological markers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and early AD. For information, see http://www.adni-info.org [19–21].
Participants
Participants were enrolled at ADNI sites in the United States and Canada during three ADNI funding cycles (ADNI-1, ADNI-2, and ADNI-GO) [19–21]. All subjects were between age 55 and 91 at baseline; English or Spanish language speakers; non-depressed; and in one of three diagnostic categories: early AD, MCI, or cognitively healthy. Cognitive status was confirmed using cut-off scores from the Clinical Dementia Rating Scale, Mini-Mental State Examination (MMSE), and Wechsler Memory Scale Logical Memory II. Complete ADNI exclusion criteria are found at http://www.adni-info.org [22]. For the first 24 months, evaluations occurred every 6 months, and every 12 months thereafter, with a mean total follow-up time of 78.2 months (SD = 29.7). Results of cognitive assessments, physical examinations, and MRI scans were considered in determining diagnostic status.
Figure 1 depicts the derivation of the analytic sample. The initial subject pool included 1,729 participants with visits up to 10/15/2016. We excluded subjects with fewer than 2 visits, missing demographic data, or baseline diagnosis of AD. After exclusionary criteria were applied, 1,307 participants remained in the sample. An analysis comparing the contribution of the components of the IICV to the index itself was performed using this sample. Only a limited number of subjects had CSF data available, resulting in a CSF analytic subsample of 349.
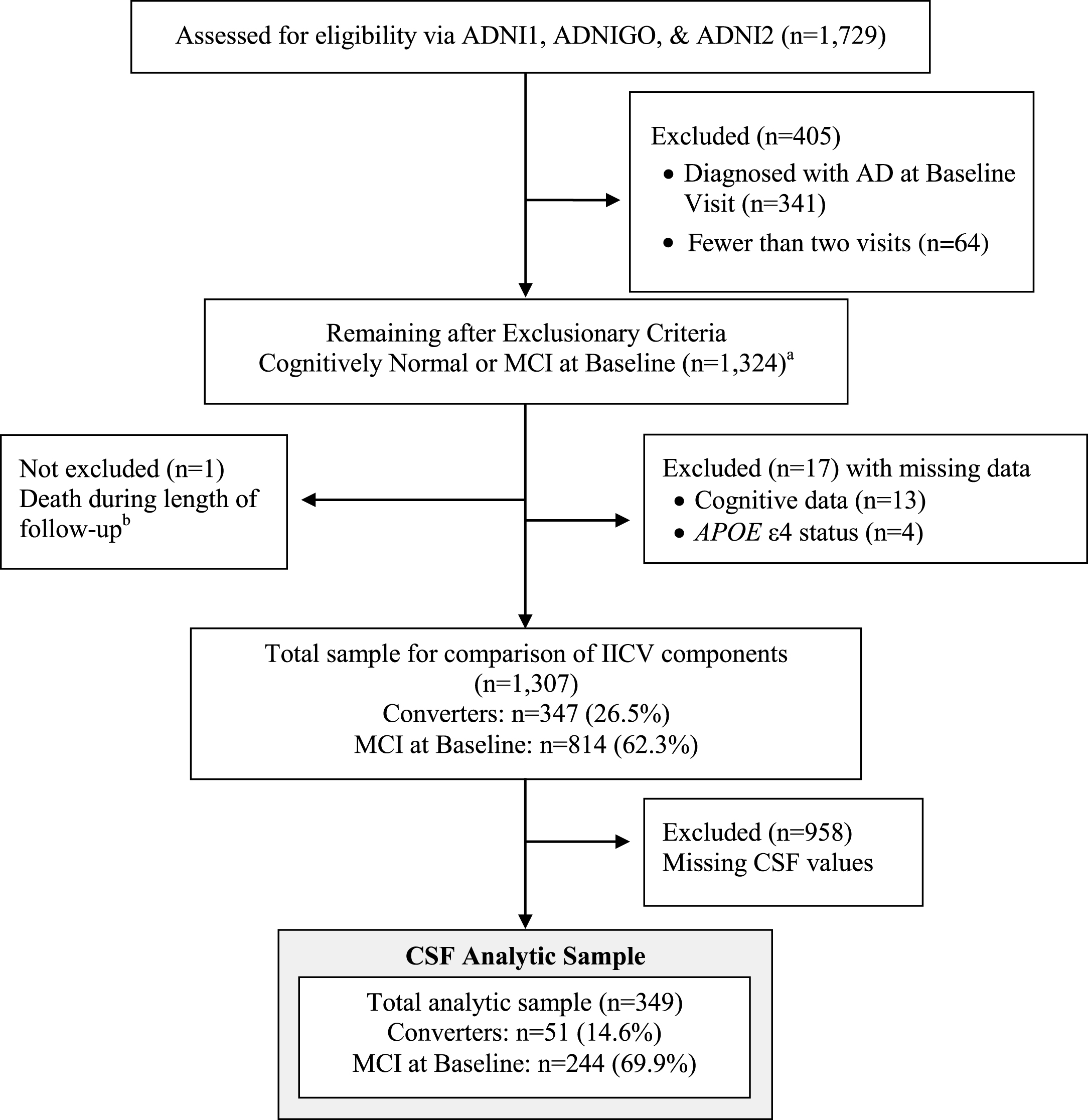
CONSORT Diagram –Sample derivation for logistic regression model including subjects with complete longitudinal and APOE ɛ4 and CSF data. Analytic model included baseline age, years of education, APOE ɛ4 status, years of follow-up, and baseline diagnosis. aThe distributions of cognitive test scores from 1,324 participants were used to derive IICV estimates. bOne subject died during length of follow-up. The subject was included; brain autopsy was used for the final diagnosis instead of clinical examination.
Participants provided written, informed consent per ADNI protocols; study sites obtained approval by the local institutional review boards, ensuring that procedures involving experiments on human subjects were done in accord with the ethical standards.
Cognitive variability
An IICV index, depicting variability at a single time point, was calculated following a previously applied method [8]. Briefly, four test scores were selected to detect across-domain “peaks and valleys” typical in early AD. Specific indices included: Rey Auditory Verbal Learning Test (RAVLT) Total of Learning Trials (memory), American National Adult Reading Test total score (ANART; crystallized reading ability), and Trail Making Test A and B (TMT A and B; speeded attention and executive function, respectively). Prior to calculating baseline IICV index, individual test scores were standardized to mean = 0 and SD = 1 using score distributions based on the most inclusive sample (n = 1,324). In addition, standardized TMT scores were multiplied by −1 so that positive z-scores represented better performance for all four test scores. The IICV index corresponded to the standard deviation of fourz-transformed baseline scores. Consistency between test scores, regardless of value, resulted in low IICVs, whereas extreme highs and lows between test scores produced high IICVs.
CSF measurement
CSF data were from the ‘UPENNBIOMK5_10_31_13.csv’ dataset, using CSF aliquots from ADNI-GO and ADNI-2. Details of CSF biomarker analyses are available on the ADNI website [23]. Briefly, CSF Aβ42 and p-tau181 were measured using an xMAP Luminex platform (Luminex Corp) and Innogenetics/Fujirebio AlzBio3 immunoassay kits, following published protocols [24], and standardized withreplicate aliquots.
Primary outcome: diagnostic conversion
At each visit, participants were evaluated and diagnosis determined by ADNI clinical investigators. In our analyses, we compared diagnosis at baseline to diagnosis at last available follow-up visit. Conversion was defined as change in diagnosis from cognitively healthy status to MCI or AD, or from MCI to AD.
Statistical analysis
We previously reported results from survival models including IICV and HVL [7]. In the current project, logistic regression models (R version 3.2.3. [25]) were used to examine whether IICV and ratio of CSF analytes were associated with odds of conversion from a cognitively healthy state to MCI or AD, or MCI to AD, through subjects’ entire follow-up. After cases with missing data were excluded, the IICV analytic sample included 1307 participants. A sub-sample for whom CSF findings were available included n = 349. Comparisons of participant demographics by baseline diagnostic groups were performed with Mann-Whitney U tests forcontinuous variables and Fisher’s exact tests forcategorical data.
In logistic regression models, our “base model” included predictors: baseline age, years of education, APOE ɛ4 status, baseline diagnostic status (MCI or cognitively healthy), and total post-baseline follow-up time. Response was conversion status at end of total follow-up time. We tested the following models: 1) base model plus IICV; 2) base model plus ratio of CSF p-tau181/Aβ42, and 3) base model with IICV and CSF p-tau181/Aβ42. Models were tested with subjects whose baseline diagnostic status was either MCI or cognitively healthy, and in a sample restricted to individuals with baseline diagnosis of MCI. Due to low rate of conversion in subjects who were cognitively healthy at baseline, an analysis restricted to this subset was not attempted. Only ten of the 105 individuals in the CSF analytic subsample who were cognitively healthy at baseline (9.5%) converted diagnostically.
To allow for direct comparison of regression coefficients, IICV and CSF ratio values were standardized for analyses (mean of zero and SD = 1). For each item, 1 standard deviation increase in the item’s raw value represented an estimated odds ratio (OR) of conversion of exp(β), where β is the estimated logistic regression coefficient for that item. When not standardized to a z-score scale, the standard deviations of IICV and CSF ratio in these data were 0.405 and 0.201, respectively.
To examine whether individual components of IICV account for associated risk more than variability between scores, we tested a model including base model predictors, IICV, and the individual IICV components (TMT A and B, ANART, and RAVLT raw scores). In other words, does IICV add explanatory power over and above its individual component scores. A stepwise backwards selection was performed on 5 cognitive items (4 individual component scores and IICV), using an Akaike Information Criterion (AIC) [26]. AIC was utilized over other backward selection methods in effort to prioritize relative proximity to the true data generating model, favoring inclusion over exclusion of convergent variables. The AIC method examines the degree to which removal of any component scores or IICV reduced the AIC index and simplified model fit for prediction. An iterative process continued until: (1) removal of a component or IICV score did not reduce AIC or (2) all 5 cognitive predictors were removed.
RESULTS
Participants were average age 72.4 years (SD= 7.09) at baseline, and well-educated (mean = 16.2 years). Table 1 lists participant characteristics by baseline diagnosis. Most participants were white, n = 325 (93.1%), and non-Hispanic n = 341 (98.8%). Compared to the larger pool of ADNI Participants included in the CSF analytic subsample were slightly younger than individuals included in the full IICV analytic sample, and less impaired on the Rey AVLT with lower IICV scores (data not included).
Participant characteristics at baseline
APOE, Apolipoprotein E; MCI, mild cognitive impairment; AD, Alzheimer’s disease; IICV, intra-individual cognitive variability; ANART, American National Adult Reading Test; RAVLT, Rey Auditory Verbal Learning Test. Statistical tests: P-values are from Mann-Whitney U tests for continuous items and Fisher’s Exact test for categorical items. Note: The CSF analytic sample is a subset of the full IICV dataset, precluding group comparisons.
Mean length of follow-up was 2.32 years (SD = 0.682). In total, 42 (12.0%) of the 349 subjects who contributed CSF converted to AD and 9 (2.6%) converted to MCI (Table 1). Converters differed from non-converters in an expected pattern. They were older, performed more poorly on cognitive measures, and demonstrated lower levels of CSF Aβ42 and higher levels of CSF tau181. Results from logistic regression models suggest that an increase in IICV elevated an individual’s odds of incident AD and MCI. Figure 2 depicts the positive association of IICV with the proportion of participants who converted diagnostically. The association occurred across the range of IICV values. Regression models in Table 2 indicate an association of CSF with conversion odds in the full sample (n = 349) and when the sample is restricted to individuals with a baseline diagnosis of MCI (n = 244). Specifically, inclusion of IICV alone resulted in ORs between 2.39 (95% CIs 1.60 to 3.56) and 2.77 (95% CIs 1.72 to 4.46), depending on whether cognitively healthy adults were included in the analytic sample.

IICV versus Conversion status with local smoothing trend (LOESS). Data are jittered around conversion status to better illustrate data densities. Panel A includes participants with MCI and those who were cognitively healthy at baseline (n = 349). Panel B includes only those individuals with MCI at baseline (n = 244). Notes: IICV, intra-individual cognitive variability. Used raw IICV score for comparison. Conversion is a dichotomous variable: Converters versus Non-converters. The trend line is smoothed using LOESS in order to illustrate the relationship between conversion and IICV score without linearity assumptions. Additionally, IICV scores are jittered to more clearly see the number of participants obtaining individual IICV scores.
Logistic regression models
Notes: Base Model included baseline age, baseline education, APOE e4 status and years of follow-up. For analyses including cognitively healthy participants and those with MCI, base model also includes baseline diagnostic status. IICV was estimated using baseline data. MCI, mild cognitive impairment; IICV, intra-individual cognitive variability; CSF, cerebrospinal fluid; OR, odd ratio; CI, confidence interval.
Similarly, estimated OR’s of conversion for 1 standard deviation increase in CSF ratio p-tau181/Aβ42 are 2.13 to 2.16, depending upon the subsample (95% CIs span 1.49 to 3.13). Figure 3 depicts the association of the ratio of standardized CSF p-tau181/Aβ42 and conversion. Like analysis of IICV and conversion, elevated ratio of p-tau181/Aβ42 corresponded to elevations in diagnostic conversion.
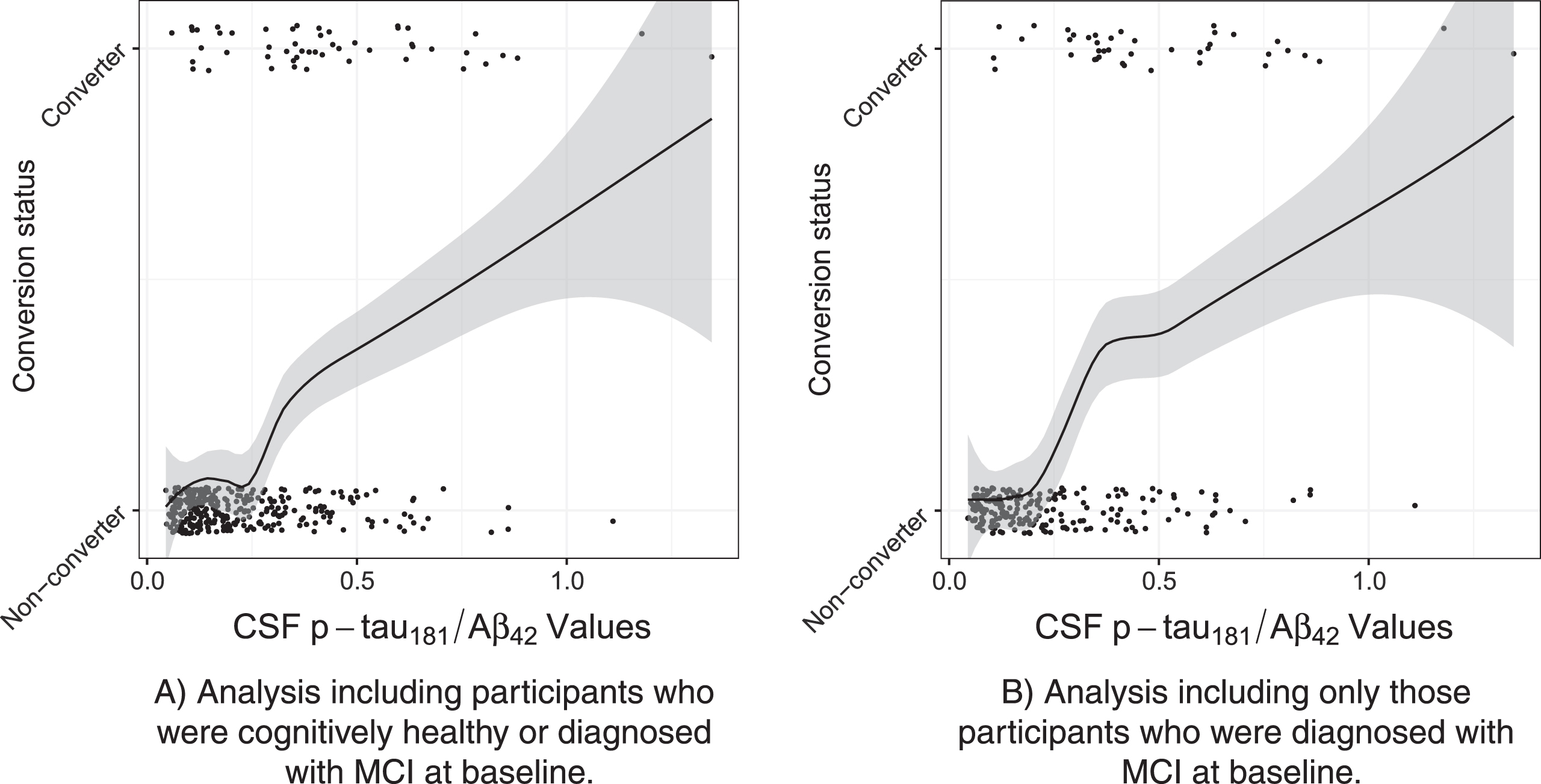
Ratio of CSF p-tau181/Aβ42 versus Conversion status with local smoothing trend (LOESS). Data are jittered around conversion status to better illustrate data densities. Panel A includes participants with MCI and those who were cognitively healthy at baseline (n = 349). Panel B includes only those individuals with MCI at baseline (n = 244). Notes: Conversion is a dichotomous variable: Converters versus Non-converters. The trend line is smoothed using LOESS in order to illustrate the relationship between conversion and CSF biomarkers without linearity assumptions. Additionally, values for the ratio of CSF analytes were jittered to more clearly see the number of participants obtaining individual ratio values.
When IICV and the ratio of CSF analytes were included in the model together, IICV continued associate with conversion odds (See Table 2). When the ratio of CSF analytes was added to models including IICV, the association between IICV and conversion appears to increase, with estimated ORs between 2.81 (95% CIs 1.83 to 4.33) and 3.41 (95% CIs 2.03 to 5.73), depending on whether cognitively healthy individuals were included in the analysis.
Lastly, we examined whether the individual components of IICV outperformed the overall estimate of variability (i.e., IICV) in predicting conversion to MCI or AD, using a larger analytic sample, not restricted to participants with CSF data (n = 1,307). Subject characteristics for this group of subjects are provided in Supplementary Table 1. An initial examination comparing conversion status with mean test performance revealed that conversion was not related to overall performance on cognitive tests (see Supplementary Figure 1). Nonetheless, the importance of IICV over and above its individual test components were compared using an AIC backward selectionprocess.
Table 3 displays the backwards selection results comparing IICV with its component tests. Overall, it appears that TMT A does not provide additional explanatory information compared to other items. Importantly, IICV was not excluded in this iterative analysis, and the final model was restricted to ANART, RAVLT, TMT B, and IICV. IICV was associated with odds of conversion over and above the tests used to calculate IICV. Thus, IICV appears to provide additional explanatory information beyond its component tests when predicting conversion.
Comparison of IICV components to IICV. Used Akaike Information Criterion (AIC) stepwise backward selection to examine contribution of IICV and individual components of IICV to model fit
Note: P-values provided by AIC models indicate whether predictors offer predictive value, not the magnitude of added value. MCI, mild cognitive impairment; IICV, intra-individual cognitive variability; ANART, American National Adult Reading Test; RAVLT, Rey Auditory Verbal Learning Test; AIC, Akaike Information Criterion.
DISCUSSION
In these analyses of ADNI data, IICV, an indicator of dispersion between cognitive test scores, was associated with elevated odds of conversion from MCI to AD or from a cognitively healthy state to MCI or AD. The IICV index used here characterized dispersion in cognitive abilities including speeded visual motor sequencing with and without an additional divided attention component, crystalized verbal abilities, and verbal memory. Whether used with or without its individual component tests, or the ratio of CSF p-tau181/Aβ42, IICV obtained at a single time point was associated with increased odds of developing incident AD and MCI.
We have previously shown in survival analyses that IICV predicted time to diagnostic conversion. Specifically, our models suggested that an estimate of IICV predicted time to incident AD and MCI even after accounting for a neuroimaging biomarker, HVL and a genetic risk factor, APOE ɛ4 status [7]. Similarly, in a middle-aged cohort enrolled in WRAP study, we noted IICV measured at midlife predicted incident cognitive decline approximately a decade after baseline [18]. In the current analyses we sought to examine how IICV compared to CSFbiomarkers.
As anticipated, the ratio of CSF values of phosphorylated tau (p-tau181) and Aβ42 were associated with elevated odds of conversion. These findings are consistent with previously published ADNI analyses, revealing associations between clinical symptoms, incident disease and CSF analytes [27, 28]. A recent summary analysis of multiple studies examining CSF biomarkers for AD-associated neurodegeneration suggested that CSF analytes are robust indicators of underlying disease pathology [2]. In particular, CSF Aβ42, p-tau, total tau (t-tau), and neurofilament light protein emerged among several candidate CSF biomarkers as the most useful for differential diagnosis. While unquestionably valuable, these data can only be obtained via lumbar puncture. This invasive procedure must be performed by trained medical personnel in a clinical research setting. Moreover, based on historical research abuses, like the Tuskegee Study of Untreated Syphilis in the Negro Male [29], the lumbar puncture procedure is associated with one of the most egregious and symbolic cases of research misconduct for African Americans [30]. For participants unwilling to complete a lumbar puncture, IICV may offer an alternative.
Obtaining a reliable IICV is dependent upon having trained examiners. This would require concerted but not insurmountable effort. Moreover, it is possible that IICV would lend itself to laptop or tablet platforms, reducing the skill level needed to collect data. Altogether, there is justification to explore IICV and other alternatives to CSF biomarkers, especially low-cost, easily disseminated alternatives, not associated with burdensome procedures, especially aversive for African Americans.
When models included both the ratio of CSF p-tau181/Aβ42 and IICV, the odds of incident AD or MCI associated with elevations in IICV remained relevant. Indeed, odds ratios for these predictors remained relatively stable in iterative models, suggesting unique predictive contributions from both IICV and ratio of CSF analytes. Indeed, there appears to be little correlation between the two predictors. Supplementary Figure 2 shows a plot of IICV to the ratio of CSF p-tau181/Aβ42. Although studies examining the association of cognitive performance and CSF analytes in pre-clinical or cognitively healthy subjects have reported somewhat mixed findings, Pettigrew et al. [31] and others [4] found associations between cognitive factors and CSF amyloid and CSF tau. Analyses presented here suggest that the processes underlying cognitive variability and those sub-serving CSF amyloid and tau abnormalities may differ, possibly explaining inconsistences in findings, and why others have reported that CSF amyloid and especially tau findings were uncoupled from cognition in the preclinical stages (e.g., Li et al. [32] and Rolstad et al. [33]). Moreover, the finding that neither IICV and CSF biomarkers appeared to suppress the effect of the other when both were included in the model, suggests that the two predictors of risk could be used together in models examining risk for AD.
The concept that dispersion in performance signifies underlying disease is an established and deep-rooted theory in cognitive psychology [9–16]. Many others have examined the relationship between cognitive variability and neurological and psychiatric illnesses, including dementia [7–11, 34–36]. Explanations for the link between inconsistency and brain disease include impaired neural networks, impaired functional connectivity, as well as executive dysfunction [37, 38]. The premise of these theories is that disease results in a disrupted ability to maintain consistent mental efforts.
Like Holtzer et al. [8], our approach to estimating IICV focused on consistency across cognitive domains, rather than consistency between trials of the same task. We intentionally selected indices which could be expected to diverge early in the AD course, e.g., TMT B was contrasted to TMT A. TMT A requires a person to connect a series of numbered circles as quickly as possible; whereas in TMT B, the individual must alternate between numbers and letters, connecting the circles as rapidly as possible. A disparity in performance between the tests would identify someone with very early executive dysfunction yet well-preserved sensory motor abilities, as is typically observed in AD.
The remaining two cognitive tests contributing to the IICV index used here were included to maximize detection of early AD-related disparities in cognitive performance. A list learning test (RAVLT), selected as a measure of hippocampal-based learning [39], was contrasted with a test of reading ability estimating baseline crystallized intelligence (e.g., semantic knowledge) [40]. In total, the cognitive indices included in our measure of variability were selected if they were likely to either reflect a typically well-preserved ability or a typically diminished ability, representing the peaks and valleys in a cognitive profile.
The older participants included in these analyses were followed for an average of 2.32 years. It is unknown how early cognitive variability appears prior to a diagnosis. Holtzer et al. [8] found that IICV predicted incident dementia on average 3.3 years after initial evaluation. Participants were ∼79 years of age and cognitively normal at baseline. In our two previously published papers, we demonstrated IICV’s predictive utility in two different groups, over disparate time periods. Similar to Holtzer et al., we found that older ADNI subjects (∼74 years) who were cognitive normal or diagnosed with MCI on average evidenced cognitive variability 30.81 months prior to diagnosis [7]. In contrast, Koscik et al. demonstrated the utility of IICV in a much younger cohort (∼53 years) over a period of 8 to 10 years [18]. In total, variability in cognitive performance appears to indicate elevated risk for later cognitive impairment and/or dementia. The exact time frame for prediction is not yet clear and may depend on how IICV is estimated and/or the characteristics of the cohort being examined.
In our final analysis, we sought to examine the overall contribution of IICV to elevated risk versus the risk for conversion associated with the components of IICV. IICV survived an iterative examination, wherein elements were individually removed from models, suggesting that IICV informed risk for conversion, over and above the contribution of its components alone.
Among the limitations in our analyses, we highlight that incident cognitive impairment in this ADNI sample primarily represented conversion from MCI to AD, i.e., conversion within a clinical population. Given the low rate of conversion in cognitively healthy subjects (n = 10), we are unable to make definitive statements regarding detection of preclinical risk. However, in our previous analysis of WRAP data, our sample was middle-aged and cognitively healthy at baseline [18]. IICV predicted incident cognitive decline in the preclinical WRAP cohort. Nonetheless, we emphasize the need for replication, especially in younger cohorts, more remote from conversion. Notably, ADNI participants with MCI were selected for inclusion based on their poor performance on memory measures in the presence of spared global cognition [22]. At the outset, individuals with MCI included in this analysis would demonstrate greater cognitive variability than the general population. Finally, an additional limitation is the relative homogeneity of the sample. Subjects were predominantly non-Hispanic and white, reflecting a selection bias toward those willing to enroll in a longitudinal study involving lumbar puncture. IICV may not be associated with diagnostic conversion for Hispanic, non-white groups or for cases of mixed or non-AD dementias.
Conclusions
If replicated, our IICV findings provide support for a practical alternative to traditional biomarkers. This option would be especially important when patients and subjects are unable or unwilling to travel to research settings, or averse to invasive procedures like lumbar punctures. Moreover, a cognitive marker could be widely disseminated with minimal effort or equipment demands. Altogether, using IICV may permit broader ability to identify at-risk individuals than traditional biomarkers.
Footnotes
ACKNOWLEDGMENTS
Contributions by first author CEG and co-authors DN, NMD, DTW and RLK are supported by funding from NIH-NIA for African Americans Fighting Alzheimer’s at Midlife (AA-FAIM, R01 AG054059) and the Wisconsin Alzheimer’s Disease Center (P50 AG033514). For coauthors MW, SCJ, CMC, RLK and SA efforts were also supported by funding from the NIH-NIA for the Wisconsin Alzheimer’s Disease Center (WRAP, P50 AG033514). Additional support in the form of statistical and scientific collaboration was provided for co-authors RLK, SCJ and CMC by the Wisconsin Alzheimer’s Institute.
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Disease Cooperative Study at the University of California, San Diego.ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of SouthernCalifornia.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Disease Cooperative Study at the University of California, San Diego.ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of SouthernCalifornia.
This is GRECC Manuscript number: 2017-07