
Abstract
Background:
Delayed Matching-to-Sample Task 48 (DMS48), a brief tool measuring visual recognition memory, is valid to identify the early stage of Alzheimer’s disease (AD) in Caucasians. However, little data is available in Chinese.
Objective:
To develop norms and optimal cutoff points for the DMS48 in Chinese elders.
Methods:
A cross-sectional study was conducted in seven memory clinics from five cities across China. DMS48 was applied to 369 Chinese aged 50 or older (138 cognitively normal [CN], 112 mild cognitive impairment due to AD (MCI-A), and 119 mild AD dementia). The demographic factors which influence DMS48 scores were investigated and the norms were established considering those factors. Receiver operating characteristic (ROC) analysis was used to determine the optimal cutoff points.
Results:
Age was shown to influence DMS48 scores (r = –0.36, p < 0.05), and we presented the age-stratified normative data for the DMS48. The optimal cutoff point is 42/43 for identifying cognitive impairment (MCI-A and AD dementia) against CN (sensitivity 97.80% and specificity 89.13%) and MCI-A against CN (sensitivity 86.60% and specificity 94.20%). A cutoff of 39/40 obtained good sensitivity (100.00%) and specificity (94.90%) in discriminating AD dementia from CN. The age-stratified optimal cutoff points for identifying MCI-A were 43/44 for individuals aged 50 to 59 years old, 42/43 for 60 to 69 years old, 41/42 for 70 to 79 years old, and 40/41 for 80 or older, respectively (sensitivity 84.80% and specificity 95.70%).
Conclusion:
This study proved that DMS48 is of good validation in screening MCI-A in elderly Chinese.
Keywords
INTRODUCTION
Alzheimer disease (AD) is the most common cause of cognitive impairment, bringing a great burden on both families and society [1, 2]. Mild cognitive impairment (MCI) is an intermediate state between normal cognition and dementia [3, 4]. MCI due to AD (MCI-A), one of the subtypes of MCI, is the early stage of AD [5]. Identifying MCI-A is of vital importance for early management of AD.
Memory impairment is the hallmark of typical AD and MCI-A. Tests coordinating encoding and retrieval paradigms such as the Free and Cued Selective Reminding Test have been proven to be sensitive in identifying very mild AD [6, 7]. Visual recognition memory (VRM) deficit could be caused by lesions of subhippocampal structures [8], where neurofibrillary tangles initially formed in AD [9, 10]. Thus, VRM impairment is suggested to be a special sign presented at the early stage of AD and tools assessing VRM may be helpful in screening for MCI-A [10]. However, visual memory assessments are not widely used in China. The Rey-Osterrieth Complex Figure [11], one of the few tools in use, is a pencil-and-paper task which restrained its use in physical impairment subjects. In addition, the Rey-Osterrieth Complex Figure relies on recall and executive function and requires drawing skills, all of which hinder an accurate assessment for memory storage [12]. It is important to search for new simple tools to simplify the usage.
The Delayed Matching-to-Sample task 48 (DMS48) is a relatively new and brief VRM accessing tool which consists of 48 targets (color pictures) [13]. In the encoding phase, subjects are asked to consecutively look at the pictures and to say whether each contained more or less than three colors (incidental encoding). Then two sets of recognition tasks are completed two minutes later and one hour later, respectively. With acquisition being facilitated and recall being ruled out, performance on the DMS48 is hypothesized to assess mainly memory storage ability which is the hallmark of MCI-A and AD. Studies showed that MCI patients who failed in the DMS48 task shared similar neuroimaging characteristics to that of early AD in terms of hypoperfusion [14], grey matter loss [15] and metabolic changes [16]. Similar profile of cognition was also shared by patients who failed in the DMS48 task and early AD patients [17]. A six-year follow-up study showed that DMS48 task deficit can be a predictor for AD conversion from MCI patients, with the sensitivity of 80% and specificity of 90.9% [18]. It is proved that DMS48 is of good validity to measure VRM and was recommended by International Working Group-2 (IWG2) [19] for the early identification of AD. However, DMS48 has not been evaluated in China. The present study aimed to establish Chinese DMS48 norms considering significant influential factors and determine the optimal cutoff points for screening MCI-A in elderly Chinese.
METHODS
Recruitment of participants
A multicenter study was conducted from January 2015 to September 2016. As China is a vast country with marked differences in geography, culture, and economy among regions, we chose seven memory clinics from five cities located in four representative regional centers across China (Ha’erbin for Northeast China, Beijing and Tianjin for North China, Hangzhou for East China, and Chongqing for Southwest China). MCI-A and mild AD dementia participants were recruited in these memory clinics. CN participants were residents from the local communities or spouses of the cognitive impaired patients. For all participants, detailed data on demographic characteristics, lifestyle, medical history, current medications, and family history were collected. Questions about cognitive impairment including the time and mode of onset, possible triggers, affected domains, progression pattern, influence on daily activities, changes in mood or behavior, and response to treatment were inquired and recorded. A battery of neuropsychological and functional evaluations was then performed to all participants. General cognition was assessed using the Chinese version of Mini-Mental State Examination (MMSE) [20], Montreal Cognitive Assessment (MoCA) [21], and the Clinical Dementia Rating scale (CDR) [22]. Memory was assessed with the World Health Organization–University of California Los Angeles Auditory Verbal Learning test (WHO-UCLA AVLT) [23]. Functional Activities Questionnaire (FAQ) [24] was administered for social functioning. The Center for Epidemiologic Studies Depression Scale (CESD) [25] was adopted for mood assessment. Hachinski Ischemic Index (HIS) [26, 27] was used to exclude vascular etiologies. Laboratory tests such as thyroxin and treponema pallidum haemagglutination (TPHA) were conducted to exclude any other conditions which may result in cognitive impairment. Brain MRI scans were arranged and undertaken for all participants except those who had undergone scans within 3 months before the cognitive assessments. All data collected were reviewed by a panel of neurologists and psychologists specialized in cognitive disorders, who assigned diagnoses by the end of each day.
The clinical core criteria of MCI due to AD proposed by the National Institute on Aging-Alzheimer’s Association workgroups (NIA-AA) [5] was utilized to recruit MCI-A patients with some operable adjustment: 1) memory impairment with an insidious onset and gradual progression; 2) scored at least 1.5 standard deviations below the age and education adjusted norms on the WHO-UCLA AVLT [23] long-delayed free recall; 3) scored higher than the cutoff points for dementia in MMSE: >17 for illiteracy, >19 for primary school, >24 for middle school and above [20], or Global CDR score of 0.5 [22]; 4) ability preserved to perform daily activities and social functions; 5) neuroimaging features consistent with incipient AD (i.e., hippocampus and entorhinal cortex atrophy) and no other lesions; and 6) no other medical or neuropsychiatric conditions that could account for the cognitive impairment. AD dementia was diagnosed according to the clinical core criteria of AD dementia proposed by NIA-AA [28] and only mild AD dementia participants with global CDR score of 1 [22] were included. Cognitive impairment referred to MCI-A and mild AD dementia in this study. Cognitively normal (CN) was assigned when participants achieved a normal score in all assessments and scored 0 on the CDR.
Apart from the excluded participants (18 missing any data which could influence the evaluation; six with mood disorders or psychiatric conditions severe enough to account for cognitive dysfunctions, 20 diagnosed as mixed cognitive impairment, and 42 diagnosed as moderate or severe AD dementia), 369 participants were finally included in the present study, consisting of 138 cognitively normal people, 112 patients with MCI-A, and 119 with mild AD dementia. The formal education was stratified into three groups: Illiterate, 1–6 years of formal education, and 7 or more years of formal education. Age of participants was stratified as 50–59, 60–69, 70–79, and ≥ 80 years. This study was approved by the Ethics Committee of Xuan Wu Hospital of the Capital Medical University. Written informed consents have been obtained from all subjects or their guardians.
DMS48
DMS48 was applied to all participants by trained raters who were blinded to the diagnosis and other neuropsychological results. The materials for DMS48 are 48 pictures consisting of 16 abstract items, 16 paired items, and 16 unique items. The test was administered to participants as described by Barbeau who, together with his colleagues, developed the DMS48 [13]. The patients were not told that this was a memory task. Firstly, all subjects were asked to consecutively look at 48 pictures and to say whether each contained more or less than three colors (encoding phase). Then a recognition task was completed two minutes later with a first set of 48 distracters (Set 1). A second recognition task was conducted one hour later with a different set of distracters (Set 2). No modification was made but the English instruction and recording sheet were translated into Chinese. In the western version, most results were discussed in reference to Set 2, as delayed recognition was given more attention [13]. Accordingly, we took the number of correct answers in Set 2 as the final score of DMS48. The score ranges from 0 to 48, and higher score stands for better performance (chance level = 24).
Statistical analysis
Pearson’s χ2 test was used to detect the differences of categorical variables (gender and education) among CN, MCI-A and AD dementia groups. ANOVA and post hoc test was used for the difference of continuous variables (age, scores of MMSE, MoCA, WHO-UCLA AVLT, and DMS48). Stepwise multiple linear regression analyses were performed to assess the contributions of the demographic variables on the DMS48 scores. Then, the distribution of the DMS48 was stratified by the demographic variables that had significant effects on the DMS48. Finally, ROC analysis was used to determine the optimal cutoff scores of the DMS48 in cognitive impairment screening with the maximum value of (sensitivity + specificity - 1). With adjusted cutoff points, psychometric values for the DMS48 were calculated in detecting MCI-A and AD dementia, including the specificity, sensitivity, positive likelihood ratio (PLR), and negative likelihood ratio. All statistical analyses were performed using the SPSS statistical package version 18.0 (SPSS Inc.; Chicago, IL, USA)
RESULTS
Demographics and psychometric value
Demographic characteristics, MMSE scores, MoCA scores, WHO-UCLA AVLT scores, and DMS48 scores are presented in Table 1. Patients with MCI-A and AD dementia were significantly older than CN group. Percentage of males was significantly higher in the AD dementia group, followed by MCI-A group. Patients with MCI-A were better educated than patients with AD dementia but less educated than CN. MCI-A group performed worse than CN group but better than AD dementia group in all assessments including DMS48, MMSE, MoCA, and WHO-UCLA AVLT.
Demographic characteristics and psychometric results
CN, cognitively normal people; MCI-A, mild-cognitive impairment due to AD; AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; DMS48, Delayed Matching-to-Sample Task 48. aCN <MCI-A and CN <AD, p < 0.001; no significant difference was identified in the MCI-A and AD, p = 0.357; bCN <MCI-A <AD, p < 0.001; cdistribution among CN, MCI-A and AD, p < 0.001; dCN >MCI-A >AD, p < 0.001.
Demographic factors influencing the DMS48
Stepwise multiple linear regression analyses were performed to assess the contributions of the demographic variables (age, gender, and education) on the score of DMS48 Set 2 in CN group. Age was found to be negatively correlated with the score of DMS48 Set 2 (r = –0.36, 95% CI [–0.67] –, p < 0.05). Education level was related with the score using Spearman correlation coefficient (p < 0.05), but failed in stepwise multiple linear regression analyses.
Age stratified norms of DMS48 Set 2 scores
According to the demographic variables’ effect, age was considered in the calculation of normative values of the DMS48 Set 2. Age stratified norms of DMS48 Set 2 scores were listed in Table 2.
Age stratified norms of DMS48 set 2 scores
Optimal cutoff points and validity of the DMS48
Firstly, we evaluated the cutoff points of DMS48 Set 2 scores without stratifying age. ROC analysis revealed that the areas under the curve (AUCs) (95% CI) for detecting cognitively impaired (MCI-A and AD dementia) against CN, MCI-A against CN, and AD dementia against CN were 0.980 (95% CI, 0.970–0.991), 0.966 (95% CI, 0.946–0.986), and 0.994 (95% CI, 0.988–1.000), respectively. Using the recommended 1-point correction, a cutoff of 42/43 obtained good sensitivity and specificity in discriminating cognitively impaired from CN and MCI-A from CN and a cutoff of 39/40 obtained good sensitivity and specificity in discriminating mild AD dementia from CN (Table 3).
Optimal Cutoff Points and Validity of the DMS48
Considering the correlation between age and DMS48 Set 2 scores, age stratified cutoff points for screening MCI-A were then calculated. ROC analysis revealed that the AUCs (95% CI) for detecting MCI-A against CN for age 50 to 59 group, 60 to 69 group, 70 to 79 group, and 80 or elders group were 0.984 (95% CI, 0.955–1.000), 0.955 (95% CI, 0.912–0.988), 0.984 (95% CI, 0.960–1.000), and 0.877 (95% CI, 0.739–1.000) respectively (Fig. 1). The optimal cutoff was 43/44 (sensitivity 91.7% and specificity 91.9%) for 50 to 59 group, 42/43 (sensitivity 85.3% and specificity 96.3%) for 60 to 69 group; 41/42 (sensitivity 88% and specificity 100%) for 70 to 79 group, and 40/41 (sensitivity 68.8% and specificity 100%) for 80 or elders. Applying the age stratified cutoff points the sensitivity and the specificity for identifying MCI-A from CN were 84.8% and 95.7% respectively (Table 4).
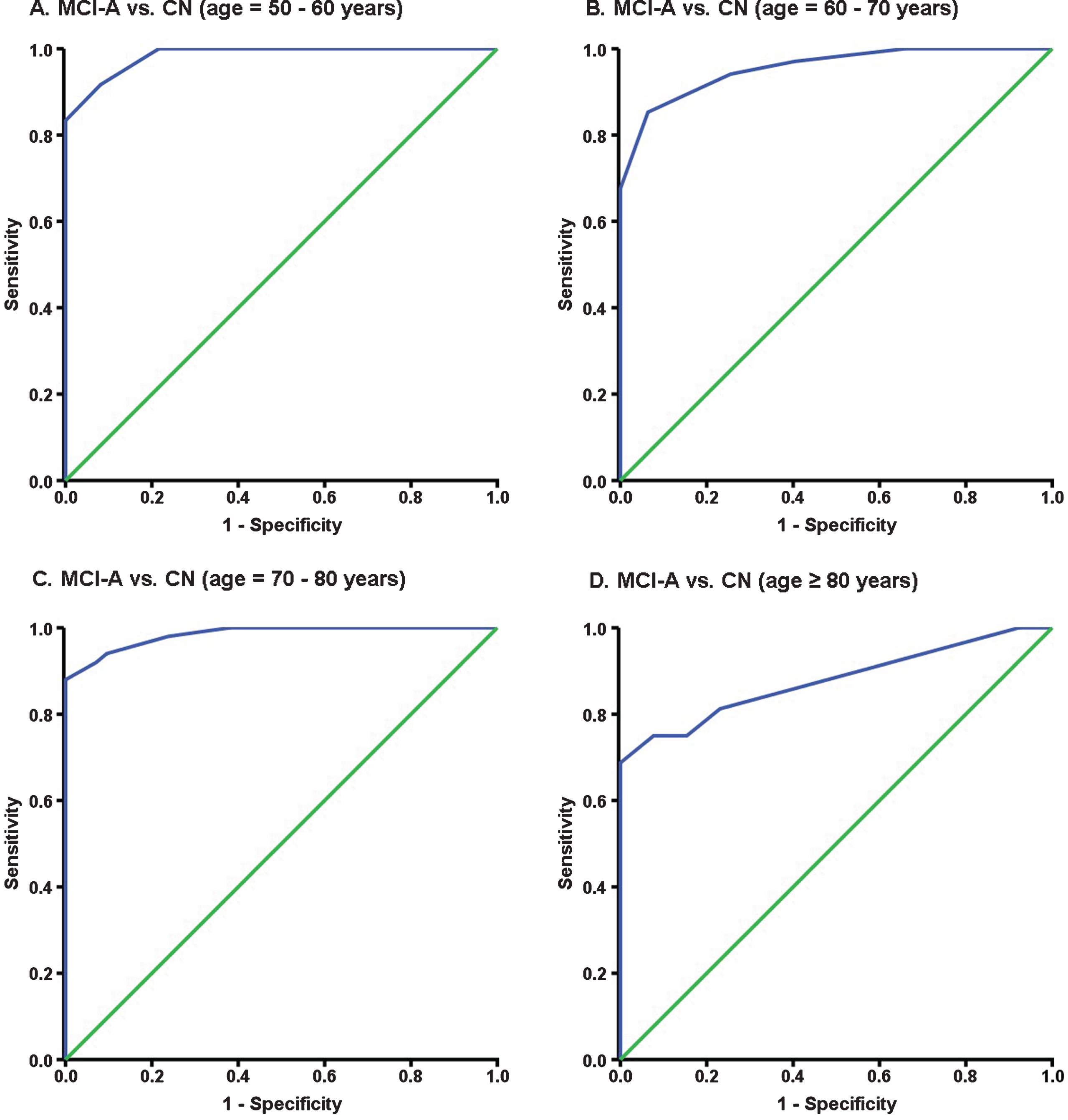
Receiver–operating characteristic (ROC) curves of DMS48 Set 2 for the detection of MCI-A from CN adjusted by age. The area under the curve (AUC) for individuals aged 50–60 years old, 60–70 years old, 70–80 years old, and 80 years or older was (A) 0.984 (95% CI, 0.955–1.000); (B) 0.955(95% CI, 0.912–0.988); (C) 0.984(95% CI, 0.960–1.000); and (D) 0.877 (95% CI, 0.739–1.000).
Age stratified optimal cutoff points and validity of the DMS48 for detecting MCI-A versus CN
CN, cognitively normal people; MCI-A, mild-cognitive impairment due to AD; NLR, negative likelihood ratio; PLR, positive likelihood ratio.
DISCUSSION
Although DMS48 is recommended in IWG2 criteria [19] as a scale for identification of AD, it is not used globally and rarely used in China. In this study, we applied the DMS48 to individuals from seven memory clinics among four representative regions in China and determined the optimal cutoff points for screening MCI-A in Chinese elders.
Validity of cognitive screening tools can be influenced by demographic variables. One previous study conducted in French revealed no effect of age, gender, educational level, or interaction between these factors on the performance of DMS48 task in CN [13]. However, another larger study identified age as an influential factor in French [29]. In present study, age also showed significant effect on the DMS48 scores. Older age correlated with worse performance. Aging has always been verified to be an important risk factor for cognitive decline [30–32], which explained why the average age of both MCI-A group and AD dementia group were older than that of CN group. Education often influences the performance of cognition screen tools, such as MoCA [21] and MMSE [20], and limited their applicability in Chinese elderly. One previous study showed an association between education and DMS48 performances [29]. However, Barbeau and his colleagues found no effect for education on the DMS48 assessment [13]. The present study revealed no relation between DMS48 and education either, possibly because it is an incidental encoding memory task in which subjects were not asked to remember the pictures but spontaneously encoded each picture without paying much attention [13]. With no limitation caused by poor education, DMS48 could be widely applied to population with all level of education.
When determining the optimal cutoff points, both sensitivity and specificity should be considered. Accordingly, present study determined the cutoff points by ROC analysis, and the scores with the maximum value of (sensitivity + specificity – 1) were chosen as the optimal cutoff points. Good validation was obtained. A cutoff of 42/43 could detect 97.80% of cognitively impaired participants (MCI-A and AD dementia) with a specificity of 89.13%, and detect 86.6% of the MCI-A participants with a specificity of 94.2%. The results are comparable to studies on western versions of the DMS48, which showed that a cutoff score of 42.7 (correct rate: 89%) could correctly classify 92.5% of CN [13] and predict AD with high validity (sensitivity: 80%, specificity: 91%) [18]. The consistency between present study and those on western version further indicates that there is less cultural difference in DMS48 performance and DMS48 is suitable for multicultural studies [13].
Identifying MCI-A would contribute to the early diagnosis and intervention of AD. We further calculated the cutoff points stratified by the influential factor (age) for detecting MCI-A against CN. Applying the age stratified cutoff points, the sensitivity was 84.8% and the specificity was 95.7%. Though the sensitivity and specificity are not significantly different from those of the unstratified one, the positive likelihood ratio is improved, indicating better validity. Like most studies, cutoff points separating MCI-A from AD dementia were not given because the main difference between the two conditions is in the dependence of daily activities instead of certain DMS48 score.
MCI patients with visual memory deficit are more likely to convert to AD [15, 34]. However, the most popular neuropsychological methods for MCI-A screening in China are MoCA, WHO-UCLA AVLT, and CDR, which assess verbal memory only. Visual memory assessment tools are used less because they are usually complicated, requiring high collaboration from the subjects. Our study proved the validity of DMS48 for identifying MCI-A. The following advantages may further guarantee a wide use of DMS48 : 1) it is a brief, short-time taking, and easily applied tool. Besides, the procedure of recognition causes minimal distress [13]. It is more acceptable for patients and would improve their compliance; 2) with no influence of education, DMS48 would improve the validity of MCI-A screening in less educated population, particularly in developing areas; and 3) less cultural differences enable DMS48 to be used in multicultural studies or international collaborative studies.
There were several limitations in this study. Firstly, the number of participants recruited is qualified for statistical analysis. However, elders aged more than 80 years are less likely to come to memory clinics. Thus, there are fewer participants in the group aged 80 or older. The findings from this stratum might be less reliable. Secondly, the clinical core criteria of MCI due to AD and AD dementia were utilized to recruit MCI-A patients and AD patients in the present study. We did not conduct biomarker tests such as cerebrospinal fluid (CSF) amyloid-β (Aβ) 42, CSF tau, and amyloid imaging demanded by the research criteria [5, 28]. Therefore, the AD pathology could not be confirmed because of the absence of Aβ biomarkers. However, the stringent clinical criteria help us to minimize false recruiting as much as possible.
In summary, we established the first DMS48 norms considering significant demographic factors for elderly Chinese and developed optimal cutoff points. With age stratified cutoff points, DMS48 is proven to be a valid instrument for MCI-A screening in Chinese eldery. It will contribute to the screening of MCI-A, particularly in the less developed regions where people are less educated. We plan to verify the cutoffs in a new Chinese sample for the next work. Future works are also needed to verify the validity of DMS48 for discriminating MCI-A from cognitive impairment with other origins. Comparisons between DMS48 and verbal tests or the combination of them also deserve further studies.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the Key Project of the National Natural Science Foundation of China (81530036), the National Key Scientific Instrument and Equipment Development Project (31627803), Mission Program of Beijing Municipal Administration of Hospitals (SML20150801), Beijing Scholars Program, and Beijing Brain Initiative from Beijing Municipal Science & Technology Commission (Z161100000216137), CHINA-CANADA Joint Initiative on Alzheimer’s Disease and Related Disorders (81261120571), Key medical professional development plan of Beijing Municipal Administration of Hospitals (ZY201301).
We gratefully acknowledge the support of our colleagues and collaborators and the assistance of the hospitals, Beijing Geriatric Hospital, Tianjin Huanhu Hospital, First Affiliated Hospital of Chongqing Medical University, Zhejiang Provincial People’s Hospital, Sir Run Run Shaw Hospital, First Affiliated Hospital of Harbin Medical University.