
Abstract
Background:
Systemic inflammation is known as a risk factor of cognitive decline.
Objective:
To investigate the effects of propolis on cognitive decline and systemic inflammation in elderly people living at high altitude.
Methods:
Sixty participants (average 72.8 years) living at altitude (2,260 meters) were randomized to receive propolis (0.83 g, n = 30) or placebo (n = 30) for 24 months. Cognitive outcomes were assessed using MMSE and serum cytokine levels were measured for 24 months in a double-blind study.
Results:
MMSE scores were 26.17 at baseline and 23.87 at 24 months in placebo group. Compared to placebo group, improvements of MMSE scores were significant in propolis-treated subjects (p = 0.007) with a response emerging over time (time points×group interaction, p = 0.016). In addition, the serum IL-1β and IL-6 levels were significantly different across treatments (p < 0.0001) showing upward and downward trends in placebo- and propolis-treated subjects, respectively (p < 0.0001). Serum levels of TNF-α were not significantly different across treatment (p = 0.0528) but with a response emerging over time (time points×group interaction, p = 0.016). In contrast, serum levels of TGFβ1 were significantly different across treatments (p < 0.0001) showing downward and upward trends in placebo- and propolis-treated subjects, respectively. Serum levels of IL-10 were significant for the effect of groups (p = 0.0411). Furthermore, MMSE scores correlated with the decrease in IL-1β and the increase in TGFβ1 in serum.
Conclusion:
Elderly people living at high altitude developed to MCI in 24 months with exacerbation of systemic inflammation. Ingestion of propolis (>12 months) protected against cognitive decline after systemic inflammation was reduced.
Keywords
INTRODUCTION
Alzheimer’s disease (AD), which is the most common cause of dementia, is a global problem in aging societies [1]. Mild cognitive impairment (MCI) is a state between normal aging and AD, and is associated with a relative risk of AD [2]. Since no effective cure for AD has been established, attention should be paid to alternative interventions in MCI that can reduce the risk of AD.
Neuroinflammation has been implicated as the key contributor to the cognitive decline in AD and MCI, because microglial-triggered neuroinflammation promotes neuronal damage as well as the deposition of Aβ [3 –6]. Epidemiological research has suggested that anti-inflammatory agents protect against the development of AD by restraining neuroinflammation [7]. Systemic inflammation has been shown to induce age-dependent microglial-mediated neuroinflammation in animal experiments [8, 9], and clinical studies have shown that systemic inflammation exacerbates the cognitive decline [10, 11].
The benefits of natural products that can improve the cognitive function in humans has been reported [12, 13]. Propolis, a resinous substance produced by honey bees as a defense against intruders [14, 15], has anti-oxidative and anti-inflammatory effects [15, 16]. The content of the active ingredients in propolis depends on the local flora at the site of collection [17, 18]. Brazilian green propolis contains mainly prenylated derivatives of cinnamic acid, among which artepillin C is known to be a major component (Yamada Bee Company, Inc., Okayama, Japan).
We have found that propolis reduces the monocyte/macrophage-related systemic inflammation and microglial-mediated neuroinflammation [19, 20], and propolis has been shown to have neuroprotective effects [21, 22]. People living at high altitude are exposed to a hypoxic environment, resulting in an increase in oxidative stress [23], which is related to systemic inflammation and brain dysfunction. We determined whether propolis protects the cognitive function of elderly people living in Qinghai-Tibet Plateau, who are susceptible to high altitude-associated cognitive decline [24].
MATERIALS AND METHODS
The study design and participants
The study population included elderly people living in Xining in the province of Qinghai, China (altitude: 2,260 meters). The exclusion criteria were as follows: inflammatory disease, chronic or acute infection, neoplasia, treatment with non-steroid anti-inflammatory drug or corticosteroids, CRP >10 mg/L, vascular dementia, or other physical or chemical factors causing dementia such as intracranial lesions, or refusal to participate. Based on our pilot study, the sample size was calculated using the software program MedSci Sample Size tools (MSST), with the “2-Sample Superiority” model. The standard deviation of difference was 7.72, the superiority margin was 0.28, and α was 0.05 at a power of 80%. The participants were randomly divided into two groups: the participants received 6 placebo capsules (placebo group, n = 30) or 6 propolis capsules (0.83 g, propolis group, n = 30) per day for 24 months in a double-blind study. Each propolis capsule, containing propolis ethanol extract, was standardized to include minimum 11.0 mg Artepillin C. Capsules of propolis and placebo were obtained from Yamada Bee Company, Inc. (Okayama, Japan). Assessments were made at baseline, and after 6, 12 and 24 months of taking propolis or the placebo at the Institution of Geriatric of Qinghai Provincial Hospital during the period of December 2013 to November 2015. The subjects were rated by two medical doctors, neurologists with more than five years of clinical experience, who had further received unified training in a three-month-cycle in order to ensure consistent results. A flow diagram of the study is shown in the Fig. 1.

The study design and participants.
Ethical considerations and study approval
The protocol was approved by the Qinghai Medical Ethics Committee (No. 2011B0282). All of the participants gave their written informed consent to participate in the present study.
Outcomes
The primary outcome of the study was the cognitive function. The differences in the changes in the cognitive function of the patients in the propolis and control groups was assessed according to their Mini-Mental State Examination (MMSE) scores at baseline, and after 6, 12, and 24 months of treatment. The secondary outcome were the systemic cytokine levels. Blood samples (10 ml) were collected from the participants at the same time points as MMSE. The serum samples were immediately centrifuged at 4degC and stored within 2 h at –80degC. The IL-1β, IL-6, TNF-α, IL-10, and TGFβ1 levels were measured by an enzyme-linked immunosorbent assay (ELISA kit, R& D Neobioscience Technology Company, USA) in accordance with the manufacturer’s instructions. For the IL-1β ELISA, the intra- and inter-CV were calculated as 3.3% and 4.1%, respectively, the LLOD was 1 pg/mL, and the recovery was 95%. For the IL-6 ELISA, the intra- and inter-CV were calculated as 4.4% and 3.7%, respectively, the LLOD was 3.1 pg/mL, and the recovery was 86%. For the TNF-α ELISA, the intra- and inter-CV were calculated as 5.2% and 7.4%, respectively, the LLOD was 15.6 pg/mL, and the recovery was 94%. For the TGFβ1 ELISA, the intra- and inter-CV were calculated as 2.9% and 6.4%, respectively, the LLOD was 31.2 pg/mL, and the recovery was 96%. For the IL-10 ELISA, the intra- and inter-CV were calculated as 5% and 7.3%, respectively, the LLOD was 7.8 pg/mL, and the recovery was 92%.
In addition, physical examinations were performed, which included assessments of the vital signs and blood pressure. Laboratory tests were performed, which included serum chemistry, hematology, and urinalysis. The serum ALT, AST, GGT, uric acid, creatinine, and beta-2 macroglobulin were tested using the respective kits (BECKMAN COULTER, USA) and detected with an automatic biochemical analyzer (Toshiba, Japan). These analyses were conducted during the study period to evaluate the safety of propolis and the placebo.
Statistical analyses
The SPSS for Windows Ver.11.5 software program was used to perform the statistical analyses. Pearson’s correlation was used for the linear correlation analysis. All of the data are shown as the mean±standard deviation (SD). Multiple group comparisons were made using a repeated two-way analysis of variance. p values of <0.05 were considered to indicate statistical significance. The correlations between cytokines (IL-1β and TGFβ1) and MMSE scores were calculated using the t-test. p values of <0.05 were considered to indicate statistical significance.
RESULTS
Characteristics of the participants
There were no significant differences in age, gender or education level between the placebo and propolis groups at baseline (Table 1). The participants underwent follow-up examinations at 6, 12, and 24 months (Fig. 1).
Characteristics of participants
Data are given as the mean±SD. SD, standard deviation; Pla, placebo; Pro, propolis.
Cognitive outcomes
The MMSE score in the propolis group was 28.19 at 24 months, significantly better than placebo (p = 0.007). Whereas in placebo-treated MMSE scores gradually declined, in propolis treated subjects a gradual improvement was observed (p = 0.016) (Table 2). Compared to the placebo group, improvements of MMSE scores were significant in propolis-treated subjects (p = 0.007) with a response emerging over time (time points×group interaction, p = 0.016). The observations indicate that the cognitive function of elderly people living at high altitude progressed to MCI within 24 months, and that propolis improved the cognitive function.
Cognitive outcomes
MMSE, Mini-Mental State Examination; Data are given as the mean±SD. Repeated two-way ANOVA was used. The effect of time points: F(3,87) = 0.863, p = 0.464; The effect of Pla and Pro group: F(1,29) = 8.323, p = 0.007; The time points×groups interactions: F(3,87) = 3.634, p = 0.016.
Systemic inflammation levels
The serum cytokine levels and cognitive assessments were made at the same timepoints, because the systemic inflammatory level (SIL) is closely related to the cognitive function. The baseline levels of pro-inflammatory cytokines, including IL-1β, IL-6, and TNF-α did not differ between placebo and propolis groups (Table 3). The serum IL-1β and IL-6 levels were significantly different across treatments (p < 0.0001) showing upward- and downward- trends in placebo- and propolis-treated subjects, respectively (p < 0.0001). The serum levels of TNF-α were not significantly different across treatment (p = 0.0528) but with a response emerging over time (time points×group interaction, p = 0.016) (Table 3). In contrast, the serum levels of TGFβ1 were significantly different across treatments (p < 0.0001) showing downward and upward trends in placebo- and propolis-treated subjects, respectively. Serum levels of IL-10 in the propolis group were significant higher than in the placebo group (p = 0.0411), while there were not significantly different across treatments (p = 0.0813) in placebo- and propolis-treated subjects, respectively (Table 4). The observations indicate that the SIL of elderly people living at high altitude shifted to a pro-inflammatory profile within 24 months, and that propolis regulates the SIL after it has been administered.
Serum pro-inflammatory cytokines
SD, standard deviation; Pla: placebo; Pro: propolis. Data are given as the mean±SD. Repeated two-way ANOVA was used. IL-1β, the effect of time points: F(3,144) = 10.79, p < 0.0001; the effect of Pla and Pro group: F(1,48) = 32.95, p < 0.0001; the time points×groups interactions: F(3,144) = 41.13, p < 0.0001. IL-6, the effect of time points: F(3,144) = 9.073, p < 0.0001; the effect of Pla and Pro group: F(1,48) = 41.13, p < 0.0001; the time points×groups interactions: F(3,144) = 29.84, p < 0.0001; TNF-α, the effect of time points: F(3,144) = 1.837, p = 0.143; the effect of Pla and Pro group: F(1,48) = 3.943, p = 0.0528; the time points×groups interactions: F(3,144) = 22.96, p < 0.0001.
Serum anti-inflammatory cytokines
SD, standard deviation; Pla: placebo; Pro: propolis. Data are given as the mean±SD. Repeated two-way ANOVA was used. TGF-β1, the effect of time points: F(3,144) = 0.5092, p = 0.6766; the effect of Pla and Pro group: F(1,48) = 32.15, p < 0.0001; the time points×groups interactions: F(3,144) = 11.43, p < 0.0001. IL-10, the effect of time points: F(3,144) = 1.835, p = 0.1435; the effect of Pla and Pro group: F(1,48) = 4.406, p = 0.0411; the time points×groups interactions: F(3,144) = 2.286, p = 0.0813.
Relationship between the cognitive outcomes and the systemic inflammation levels
To further prove the benefit of propolis for SIL and the cognitive outcomes, we analyzed the correlation directly between the cytokine findings and the MMSE scores. As shown in Fig. 2A, the analysis of the correlation between the serum concentrations of IL-1β and the MMSE scores in the placebo group demonstrated negative correlations at months 12 and 24 (r = –0.46, p < 0.05; r = –0.48, p < 0.05), while no significant relationship was observed at months 0 and 6 (r = 0.3, p > 0.05; r = 0.01, p > 0.05). Similar results were obtained in the propolis group (Fig. 2B) showing negative correlations at months 12 and 24 (r = –0.47, p < 0.05; r = –0.39, p < 0.05) but no significant relationship at months 0 and 6 (r = 0.01, p > 0.05; r = 0.2, p > 0.05). These results indicate that higher serum IL-1β levels tend to be associated with lower MMSE scores, whereas lower serum IL-1β levels tend to be associated with higher MMSE scores. In contrast, the analysis of the correlation between the serum concentrations of TGFβ1 and the MMSE scores in the placebo group revealed positive correlations at months 12 and 24 (Fig. 3 A, r = 0.36, p < 0.05; r = 0.37, p < 0.05) but no significant relationship at months 0 and 6 (r = 0.07, p > 0.05; r = 0.17, p > 0.05). Similar results were obtained in the propolis group (Fig. 3B), showing positive correlations at months 12 and 24 (r = 0.41, p < 0.05; r = 0.45, p < 0.05) but no significant relationship at months 0 and 6 (r = 0.24, p > 0.05; r = 0.17, p > 0.05). These results indicate that higher serum TGFβ1 levels tend to be associated with higher MMSE scores, and higher serum IL-1β levels tend to be associated with lower MMSE score. Taken together, these findings suggest that the benefit of propolis on cognitive outcomes may depend on SIL improvement.

Correlation between the serum concentration of IL-1β and the MMSE scores in placebo- and propolis-treated subjects.
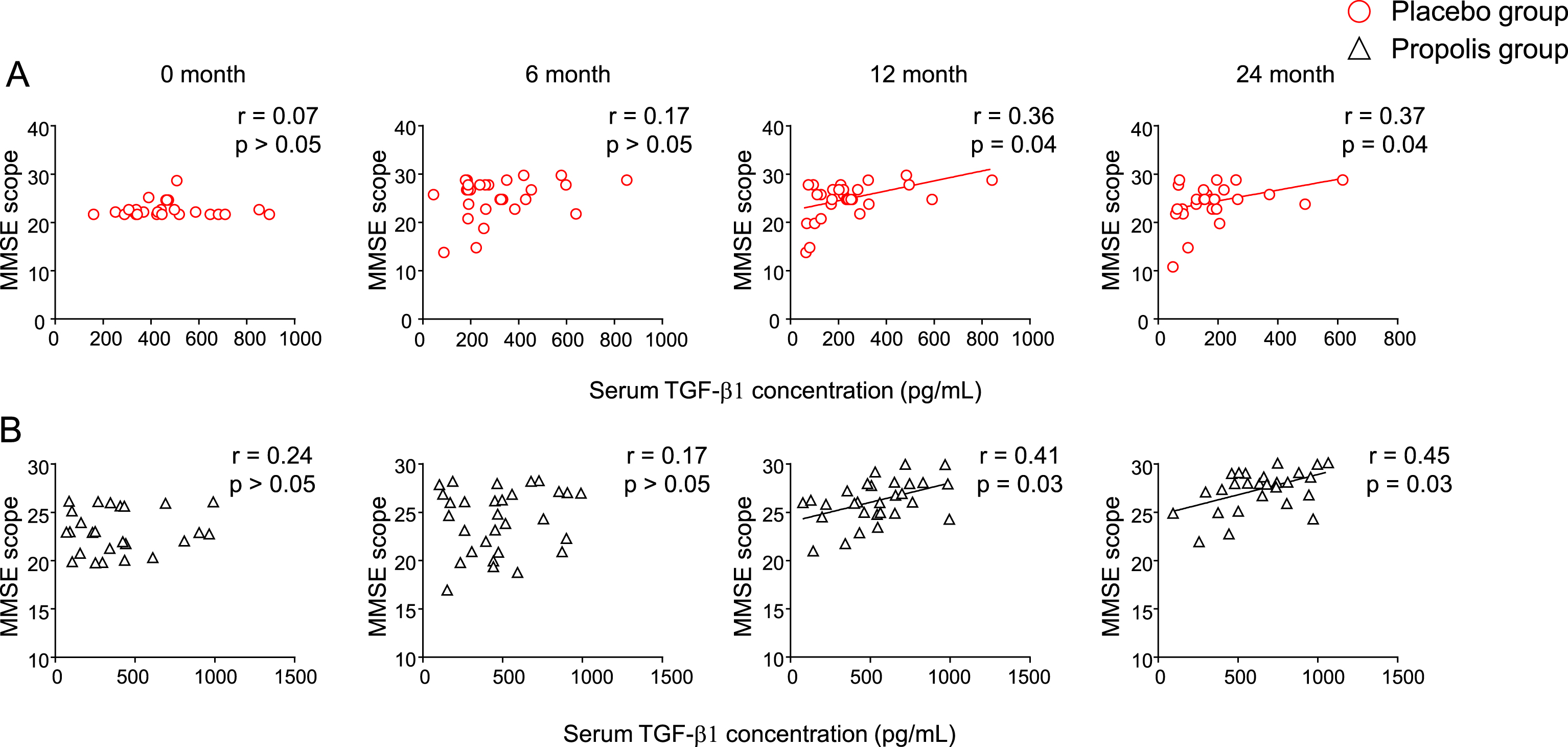
Correlation between the serum concentration of TGFβ1 and the MMSE scores in placebo- and propolis-treated subjects.
Clinical adverse events
The serum levels of ALT, AST, and GGT, and the serum levels of uric acid, creatinine and -2-macroglobulin and creatinine were assessed at the same time points as the assessments of cognitive function and SIL in order to evaluate the safety of propolis and the placebo, specifically in relation to the function of the liver and kidneys. The serum levels of ALT, AST, and GGT fluctuated within the normal ranges during the 24-month study period, and no significant differences in these indices were found between the propolis and placebo group at the baseline, 6-, and 12-month time points. On comparing the placebo group with the propolis group, significance for the effect of time points×group interactions (p = 0.0303) was found in the serum levels of ALT but not those of AST (p = 0.0628) or GGT (p = 0.1798) (Table 5). At baseline, the serum levels of uric acid, β-2-macroglobulin and creatinine were within the normal ranges in both the propolis and placebo groups; there were no significant changes in these indices during the 24-month study period (Table 6). Furthermore, the baseline blood levels of glucose (Supplementary Table 1), total cholesterol and LDL-cholesterol (Supplementary Table 2) were within the normal ranges in both the propolis and placebo groups, and showed no significant differences during the 24-month study period. These findings demonstrate the safety of the trial and the usage of propolis for 24 months. To the best of our knowledge, this is the first study to show the safety of propolis using laboratory data.
Serum liver function markers
SD, standard deviation; Pla: placebo; Pro: propolis, ALT, Alanine transaminase; AST, Aspartate aminotransferase; GGT, γ-glutamyl transpeptidase. Data are given as the mean±SD. Repeated 2 way ANOVA was used to analyze in each markers. ALT, F(3, 232) = 3.027, p = 0.0303; AST, F(3, 232) = 2.468, p = 0.0628; GGT, F(3, 232) = 1.645, p = 0.1798.
Serum renal function markers
Uric Acid normal range: 178.4–498.7(μmol/L); β-2-macroglobulin normal range: 0.8–2.4 (mg/L); Creatinine normal range: 40–120 (mmol/L). SD, standard deviation; Pla: placebo; Pro: propolis, Data are given as the mean±SD. Repeated 2 way ANOVA was used to analyzed in each markers. Uric Acid, F(3, 232) = 1.117, p = 0.3429; β-2-macroglobulin, F(3, 232) = 0.4946, p = 0.6864; Creatinine, F(3, 232) = 1.39, p = 0.2467.
DISCUSSION
The present 24-month randomized, placebo-controlled, double-blind study of elderly people living at high altitude without dementia revealed the following findings: 1) the MMSE scores of elderly people declined to the point of MCI in the 24-month study period in association with an increase in their serum levels of inflammation markers from 6 months; and 2) propolis improved the MMSE scores from 12 months, which was followed by a decrease in their serum inflammation marker levels from the 6-month time point. The findings demonstrated the importance of low SIL in maintaining the cognitive function of elderly individuals.
MCI is a known risk factor for dementia and a represents a prodromal phase of the condition [25]; however, population studies have shown that up to 55% of patients with MCI show a return to normal cognition [26, 27], while clinical studies report that up to 15% of patients with MCI show a return to normal cognition [28]. The MCI stage is therefore considered to be the optimum stage for intervening with preventative therapies [29]. The MMSE is used to screen for MCI, which is indicated by scores of <25 [25 , 31]. The setting of the present study was a high-altitude location, where a higher percentage of the elderly population suffers from cognitive decline [24]. The baseline MMSE scores were 26 in both the placebo and propolis groups; however, the MMSE scores showed a significant decrease to 23.86 at the 24-month time point in the placebo group. The longitudinal observations suggest that the cognitive functions of elderly people living at high altitude decline to the point of MCI within 24 months without any intervention because MMSE scores of <25 are used to screen for MCI [25 , 31]. This observation agreed with previous studies showing that individuals living at high altitude are more susceptible to MCI [32]. We used the MMSE scores to evaluate the effects of propolis on cognitive outcomes, because MMSE scores are used to determine the cognitive benefits of supplements in patients with MCI [33]. In comparison to the placebo group, the MMSE scores showed significant improvement from the 12-month time point and was observed to have continued to improve at the 24-month time point in the propolis group. In comparison to the baseline, the MMSE scores were significantly improved at the 24- month time point in the propolis group. The longitudinal and sectional observations demonstrate that the intake of propolis improved the subjects’ cognition. The observations suggest that early intervention using natural products may be of benefit in helping patients with MCI return to normal cognition and/or delay the progression of MCI to AD [33, 34].
SIL depends on the balance of multiple cytokines in the circulation. High serum levels of pro-inflammatory cytokines, including IL-1β, TNF-α, and IL-6, are associated with increased cognitive decline, particular in AD [10, 35]. High serum levels of IL-1β, a key molecule for driving the inflammatory cascade, amplify the inflammatory cytokine cycle [36], and high serum levels of TNF-α lead to an increased cognitive decline in AD patients [10]. In addition, the serum level of IL-6 is more robustly associated with cognition [11], which suggests that it is a sensitive and appropriate marker for SIL [37]. In the present study, the cognitive decline of the participants was found to occur after the increase in the serum levels of IL-1β, TNF-α, and IL-6 in the placebo group. In contrast, cognitive improvements were found after the decrease in the serum levels of IL-1β, TNF-α, and IL-6 in the propolis group. These observations demonstrate that early intervention by administering propolis to reduce the SIL by ameliorating the circulatory levels of multiple inflammatory cytokines may help to improve cognitionfunction.
TGFβ1 is a multifunctional anti-inflammatory cytokine with immunomodulatory activities, and regulates cell proliferation, growth, and differentiation. In the present study, the cognitive decline to MCI was found to occur after a decrease in the serum level of TGFβ1. This was supported by previous studies, which showed that a low serum level of TGFβ1 was a predictor of cognitive decline in patients with MCI and AD [38 –40]. The present study revealed, for the first time, that cognitive outcomes were improved following an increase of serum levels of TGFβ1, which occurred after the intake of propolis. The findings strongly suggest that high levels of TGFβ1 in serum may improve the cognition function in patients with MCI. The elevation of TGFβ1 may affect the SIL by reducing the levels of multiple pro-inflammatory cytokines, including IL-1β, TNF-α, and IL-6. Furthermore, TGFβ1 may protect the cerebral vessels that are damaged by systemic inflammation, because the damage of the cerebral vessels marks the start of the cognitive decline [38, 41].
The serum levels of ALT, AST, and GGT are tested routinely in the clinical setting. In addition to their role as liver function markers, they also reflect the level of oxidative stress. Indeed, GGT is used as an early marker of oxidative stress, as it degrades extracellular glutathione, the body’s master antioxidant [42], resulting in the levels of GGT being the exact opposite of the levels of antioxidants in serum [43]. Oxidative stress is known to be closely linked to SIL, and oxidative stress in liver, the largest organ in the body, is considered to largely affect SIL. Therefore, the significant decrease in the liver function markers in the propolis group at 24 months suggests that a reduction in the oxidative stress in the liver may underlie the propolis-induced decrease in SIL [44, 45].
Depending on the content of lipid soluble active ingredients, including p-coumaric acid [22], propolis might affect microglial-mediated neuroinflammation, which damages neurons and is a key contributor to cognitive decline [3 , 19]. We have demonstrated that propolis inhibits the NF-κB activation-dependent secretion of pro-inflammatory cytokines and the generation of ROS from the mitochondria in microglia [5]. Indeed, clinical research has shown that treatments to reduce neuroinflammation result in cognitive improvement [7]. Propolis may assist in maintaining synaptic plasticity. Using cultured human neuronal SH-SY5Y cells, we found that propolis induced the production of Arc, the critical immediate-early gene for the maintenance of synaptic plasticity and long-term memory, which declines with aging. Furthermore, propolis upregulated the expression of BDNF mRNA, which induces the expression of Arc, and reversed the impairment of the BDNF-induced Arc expression by both Aβ and IL-1β in cultured human neuronal SH-SY5Y cells [22]. Furthermore, propolis may also affect perivascular macrophages, a possibility that needs to be explored in the future. Thus, propolis has effects on both the periphery and the brain.
Propolis is a resinous substance produced by honeybees as a defense against intruders, which has been used, for its therapeutic properties, since ancient times. The chemical composition of propolis depends on the local flora at the site of collection [17, 18], and Brazilian green propolis contains artepillin C, a major component that has been shown to have anti-inflammatory [19, 38] and neuroprotectiveeffects [22].
Our findings need to be considered in light of the strengths and limitations of the present study. A key strength of the present study is that it measured multiple inflammation-related cytokines, which reflect the SIL and which are therefore associated with the cognitive function. The high-altitude setting is another strength because elderly people living in a hypoxic environment are more susceptible to cognitive decline. A further strength is the use of appropriate chemical indices to evaluate the safety profile of the ingestion of propolis over a 24-month period, because most studies to investigate the effects of herbal medicines in the treatment of MCI have been limited to 3–12 months. Longer studies are necessary to properly determine the benefits of intervention and the safety of natural products [13].
The present study is associated with some limitations, including the small study population that lived in a special region; thus, it was not fully representative of the general population. A further limitation is that we only measured the levels of two anti-inflammatory markers. Although TGFβ1 and IL-10 are widely measured, it remains unclear whether there are anti-inflammatory cytokines that are more relevant to cognitive improvement. A further study in a larger population is needed to confirm the effects of propolis in the population at sealevel.
In conclusion, our observations demonstrate that the cognitive function of elderly people living at high altitude declined to MCI after an increase in the SIL, propolis improves the cognitive function by reducing the SIL. Taken together with the findings that propolis ameliorated microglial-mediated neuroinflammation and maintained synaptic plasticity, natural products, such as propolis, could be used as alternative treatments for the cognitive decline in MCI and for reducing the risk of AD.
Footnotes
ACKNOWLEDGMENTS
This study was supported by Grants-in-Aid for Scientific Research (16H05848, 17K17093), Yamada Research Grant (N0.0183) and Study abroad personal science and technology activity project of Ministry of Human Resources and Social Security of the People Republic of China (NO:(2012)258). The authors would like to thank the Institution of Geriatrics for its support and all members in the Centre laboratory of Qinghai Provincial Hospital for performance and feedback throughout this study. We would like to thank all the participants and their guardians for participating in this study.