
Abstract
Background:
There is insufficient available information on behavioral changes in the absence of cognitive impairment as factors increasing the risk of conversion to dementia.
Objective:
To observe and analyze patients with mild behavioral impairment (MBI), mild cognitive impairment (MCI), and a psychiatry group (PG) to compare the risk of progression to dementia.
Methods:
From 677 initially assessed ≥60-year-old patients, a series of 348 patients was studied for a five-year period until censoring or conversion to dementia: 96 with MBI, 87 with MCI, and 165 with general psychiatry disorders, including 4 subgroups: Anxiety, Depression, Psychosis and Others. All patients were assessed with clinical, psychiatric, neurological, neuropsychological, and neuroimaging studies.
Results:
From 348 patients, 126 evolved to dementia (36.2%). Conversion was significantly higher in MBI (71.5%), followed by the MCI-MBI overlap (59.6%) and MCI (37.8%) groups, compared to PG (13.9%) (Log-rank p < 0.001). MCI patients mostly converted to Alzheimer’s dementia, while MBI converted to frontotemporal dementia and Lewy body dementia. Patients in PG converted to Lewy body dementia and frontotemporal dementia.
Conclusion:
Conversion to dementia is significantly higher in patients with neuropsychiatric symptoms. The MBI concept generates a new milestone in the refining of diagnosis of neurodegenerative diseases and the possibility of creating neuropsychiatric profiles. Its earlier identification will allow new possibilities for therapeutic intervention.
Keywords
INTRODUCTION
Even though it is known that neuropsychiatric symptoms (NPS) are common in dementia and are recognized as core to the dementia process by the National Institute on Aging-Alzheimer’s Association (NIA-AA) [1], they still have not been extensively studied in the pre-dementia stage. The NPS NIA-AA core criteria for all-cause of dementia are described as “changes in personality, behavior, or comportment symptoms that include: uncharacteristic mood fluctuations such as agitation, impaired motivation, impaired initiative, apathy, loss of drive, social withdrawal, decreased interest in previous activities, loss of empathy, compulsive or obsessive behaviors, social unacceptable behaviors” [1].
Instead, in mild cognitive impairment (MCI), those NPS have been more characterized and the presence of apathy, depression, agitation, delusions, hallucinations, and sleep disorders has been associated with an increased risk of progression to dementia [2, 3]. With regards to dementia, NPS occur in 80–90% of patients during the clinical course of the disease and fluctuate over time. But, while these symptoms have been evaluated in cross-sectional studies, longitudinal studies are scarce [4].
Since many years ago, there has been greater awareness of the importance of NPS in dementia due to their high prevalence, the increased caregivers’ burden, and the early institutionalization of patients that NPS induce [5–7]. Even more, it has been reported that caregivers’ burden is more related to behavioral disorders than to cognitive impairment [8, 9] and this burden can be psychological and/or physical and/or economic.
NPS are an important manifestation of the dementia syndrome regardless of the underlying disease, and have a strong correlation with the degree of functional impairment. Taragano & Allegri (2003) proposed the existence of a syndrome named “Mild Behavioral Impairment” (MBI) [10]; at the International Conference of Alzheimer’s Disease (2004), it was suggested that many patients convert to dementia with NPS as the first indicators of the development of a neurodegenerative disease [11]. Later (2008), we published that MBI defines a late life syndrome with prominent psychiatric and related behavioral symptoms in the absence of major cognitive symptoms [12] and demonstrated (2009) that MBI is associated with a greater and faster progression to dementia [13].
Objective
The aim of our study was to observe and analyze patients with MBI, MCI, and a psychiatric group to compare the risk of progression to dementia.
MATERIALS AND METHODS
Study population
A 5-year prospective, longitudinal inception cohort study was carried out with ≥60-year-old patients attending to the Neuropsychiatry Research Unit of CEMIC University Hospital between January 2007 and January 2012.
The neuropsychiatry research unit belongs to the Neurology Section of the Medicine Department of CEMIC University Hospital. The research group was a multidisciplinary team composed by neurologists, psychiatrists, gerontologists, neuropsychologists, and psychologists. Patients were diagnosed with MCI, MBI, or general psychiatry disorders.
Diagnosis
MBI was defined as a behavioral disturbance not meeting NINCS-ADRDA [14] criteria for Alzheimer’s dementia, Lund and Manchester criteria [15] for frontotemporal dementia (FTD), and DLB International Consortium criteria [16] for Lewy body dementia (DLB). Additionally, patients must not also meet the DSM-IV criteria [17] for psychosis or another major psychiatric condition.
MBI inclusion criteria
a) Accept to participate in the study and signed inform consent; b) Patients ≥60 years old; c) Presence of a major change in patient behavior this change occurring later in life (≥60) that is persistent (≥6 months); d) No complaint of cognitive impairment by patient/informant; e) Normal occupational and social functioning; f) Normal activities of daily living; g) Absence of dementia.
Major persistent changes in patient behavior that might have led to a diagnosis of MBI are as follows: agitation, anxiety symptoms, apathy, aspontaneity, delusion symptoms, depressive symptoms, disinhibition, emotional lability, euphoria, impulsivity, indifference, irritability, lack of empathy, loss of insight, loss of personal hygiene, loss of social tact, oral/dietary changes, perseverant behavior, sleep disorders.
A patient with major persistent change in behavior but no cognitive complaints from either the patient or the caregiver was considered to have MBI regardless of whether cognitive impairment was subsequently found on testing or not.
MBI exclusion criteria
a) Patients <60 years old; b) Impaired daily activities; c) Presence of Alzheimer’s dementia [14]; d) Presence of FTD [15]; e) Presence of LBD [16]; f) Presence of another concomitant neurological or psychiatric disorder that could better explain disturbances (i.e., epilepsy, major stroke, tumors, schizophrenia, etc.); g) Behavioral disturbances of acute onset; h) Alcohol or substance abuse.
MCI was defined as a cognitive decline meeting Petersen et al MCI criteria [18].
MCI inclusion criteria
a) Accept study participation and signed informed consent; b) Age ≥60 years old; c) Memory complaint or other cognitive complaint; d) Normal activities of daily living; e) Normal general cognitive function; f) Abnormal memory or other abnormal cognitive functions for age; g) Not demented.
Abnormal memory or other abnormal cognitive functions for age were defined as a score on a neuropsychological standardized test 1.5 SD below the mean compared with individuals of the same age and level of education.
A patient with cognitive complaints and psychiatric symptoms was considered to have MCI regardless of whether NPS were subsequently found on testing or not.
MCI exclusion criteria
a) Age <60 years old; b) Impaired daily activities; c) Presence of Alzheimer’s dementia [14]; d) Presence of FTD [15]; e) Presence of LBD [16]; f) Presence of another concomitant neurological or psychiatric disorder that could better explain the cognitive symptoms (i.e., epilepsy, major stroke, tumors, schizophrenia, etc.); g) Acute cognitive disturbances; h) Alcohol or substance abuse.
The psychiatric group
In 2009, we demonstrated that MBI is associated with a higher risk for dementia compared to MCI. In the present study, we aim to verify if the risk of conversion to dementia of the MBI group is different from those patients with general psychiatric disorders (PG).
Psychiatric illnesses were diagnosed according to DSM-IV diagnostic criteria [17]. A complete semi structured neuropsychiatric interview was performed and neuropsychiatric general and focused scales were used.
The following inclusion criteria were applied to define the PG:
Inclusion criteria for the psychiatric group
Age ≥60 years old; Patients with general psychiatric disorders meeting DSM-IV diagnostic criteria for major depression disorder (MDD), generalized anxiety disorder (GAD), schizoaffective disorder (SZD), personality disorder, post-traumatic stress disorder (PTSD), bipolar disorder type I and II (BPD I and BPD II); Patients without suspected or reported dementia; If a patient had cognitive symptoms, a responsible family member or informant should ensure that they were not the first symptoms of the psychiatric illness.
Exclusion criteria for the psychiatric group
Age <60 years old; Impaired daily activities; Presence of Alzheimer’s dementia [14]; Presence of FTD [15]; Presence of LBD [16]; Other neurological problem or psychiatric disorder that could better explain the behavioral symptoms (e.g., epilepsy, tumors, schizophrenia); Acute behavioral disturbances; Alcohol or substance abuse.
Screening procedure
All of the recruited patients signed a written informed consent after they were given a full explanation of the study. The research was performed in accordance with the ICH Good Clinical Practice guidelines, the latest revision of the 1964 Helsinki Declaration (last amended in Seoul 2008), and the Buenos Aires Government Health Authorities regulations.
Patients were assessed using a semi-structured neuropsychiatric interview and were examined at least every 6 months or when necessary. At each visit conversion to dementia was assessed.
Physical examinations and laboratory analysis were performed at baseline and whenever was needed as it is done in usual care.
Vascular risk factors and co-morbidities such as body mass index >30, high blood pressure, high blood cholesterol levels, cigarette smoking, diabetes, sedentary lifestyle, hypothyroidism and coronary heart disease were assessed.
Two scales were used to assess psychiatric symptoms, the Beck Depression Scale [19] and The Neuropsychiatric Inventory (NPI) [20].
An extensive neuropsychological battery to evaluate cognitive ability was administered to each patient: Mini-Mental State Examination (MMSE) [21], Digit span [22], Trail making test “A&B” [23], Boston naming test [24], Semantic and Verbal fluency [25], Signoret memory battery [26], and Wechsler Scale of Intelligence [27].
Methodology used to screen for conversion to dementia
Clinical Dementia Rating Scale (CDR) was used to evaluate the stage of cognitive impairment and dementia [28, 29]. CDR from 0,5 to 1: When a subject convert from the CDR-0.5 score to CDR-1, it was considered a significant clinical milestone in the progression of the disease and was interpreted as the conversion from mild deterioration stage to dementia stage.
Structural imaging (Brain CT scan or MRI) was performed at baseline to all participants for diagnostic purpose.
Functional brain imaging (Tc99SPECT or FDG18PET-CT) was performed only for research purposes and it was planned to be obtained from at least 30% of participants.
Statistical analysis
Variables from patients grouped within MBI, MCI, and PG were compared. Categorical variables were expressed as percentages. For continuous variables, the mean and standard deviations were estimated. For the non-normal distributed variables, the median and percentiles were considered.
Differences in the frequency of distribution were compared using univariate χ tests. Student’s t-test was used to compare groups with continuous variables, while non-parametric Mann-Whitney-Wilcoxon and Kruskall-Wallis tests were used to compare groups with non-normal distributed variables. Kaplan-Meier curves for survival analysis were used to analyze the time from evolution to dementia.
The follow-up period for each patient was from baseline visit to the evolution to dementia, censoring or exclusion from the study. Mann-Whitney-Wilcoxon U test and Cox proportional models were also used to analyze associations between multiple explanatory variables and conversion to dementia. The effects are shown as risk indices with 95% confidence interval. Stata 8.0 software was used for all statistical analyses (StataCorp LP, College Station, Tex.).
RESULTS
Study population
Six hundred and seventy-seven ≥60-year-old patients were initially assessed. Patients with pre-existing dementia were excluded (n = 210), while other 74 patients did not attend to follow up visits. Patients with cognitive or behavioral symptoms not attributable to a specific psychiatric disorder (n = 203) were included: 87 MCI, 96 MBI, and 20 lost follow up. The PG included 190 patients with specific psychiatric disorders: 165 completed the study and 25 were lost in follow up.
Total study sample consisted of 348 patients.
Conformation of the psychiatric group
The PG was divided in four subtypes of psychiatric domains: Anxiety (GAD), n = 33; Depression (MDD), n = 66; Psychosis (SZD), n = 31; and Others (personality disorder, PTSD, BPD I, and BPD II), n = 35.
Demographic data
Demographic data is depicted in Table 1. Considered variables showed no statistical differences between groups.
Patients’ demographic characteristics at initial visit assessment
*Kruskal – Wallis test; †Pearson χ2.
Clinical characteristics
Family background of dementia
Statistical differences were found between MCI, MBI, and PG groups (PG: χ2 = 19.0, df = 2, p < 0.001; Table 2).
Clinical characteristics at initial visit assessment
*Pearson χ2. Archaic reflexes were considered as PRESENT or ABSENT. PRESENT was defined when the patient had one or more of the following reflexes: suck, snout, palmomental, and grasp reflexes, even though if they were found in a mild presentation.
Neurological exam
The distribution of pyramidal, extrapyramidal signs, and archaic reflexes was heterogeneous (χ2 = 75.3, df = 6, p < 0.001) showing a greater frequency of these symptoms in MBI patients (Table 2).
Psychopharmacological treatment
The prescription of psychopharmacological drugs was heterogeneous between groups (χ2 = 42, df = 8, p < 0.001), with the PG group showing the highest prescription of these drugs, followed by the MBI group (Table 2).
Vascular risk factors and co-morbidities
Significant differences were found between groups in the following variables: BMI ≥30 (p = 0.046), coronary heart disease (p = 0.028), diabetes (p = 0.044), sedentary lifestyle (p = 0.001), and dyslipidemia (p = 0.043). On the other hand, there were no significant differences in number of co-morbidities (p = 0.95). More detailed description about these data is out of the scope of this paper.
Behavioral symptoms
Behavioral symptoms were found in almost a quarter of MCI patients (Table 3). Irritability, disinhibition, and delusions followed by nighttime behaviors, depression, and apathy were the predominant symptoms in MBI group while anxiety, irritability, and nighttime behaviors were the predominant symptoms in MCI group. No differences between MCI and MBI groups were observed in scores of Beck Depression Inventory.
Neuropsychiatric symptoms in MCI and MBI patients at initial assessment
*Pearson χ2; †Fisherexact ; ‡Wilcoxon Rank sum test; NPI, Neuropsychiatric Inventory; BDI, Beck Depression Inventory.
Cognitive symptoms
Memory impairment symptoms were found in more than a quarter of MBI patients (27.1%) as shown in Table 4.
Cognitive profile in MCI and MBI patients at initial assessment
*Pearson χ2; †Wilcoxon Rank sum test; ‡t-test; MMSE, Mini-Mental State Examination.
Significant differences were observed in language; verbal, executive and global IQ; attention; executive functions; and total MMSE between MCI and MBI groups (Table 4).
Neuroimaging findings
There were no significant differences (p > 0.05) between MCI and MBI groups in patients with underling vascular disease, atrophy (focal and general) (Table 5).
Neuroimage findings in MCI and MBI patients
*Pearson χ2; †Fisher Exact test.
Conversion to dementia
During the five-year follow-up period, from the total 348 patients, more than a third part (36.2%, n = 126) converted to dementia. A higher proportion of the suspected pre-dementia patients (MBI plus MCI) converted to dementia (56.3%, n = 103) with a cumulative yearly rate of conversion of 10.0% for the first year, 29.0% for the second year, 45.5% for the third year, 50.0% for the fourth year, and 56.3%, finally, for the fifth year. In terms of Kaplan-Meyer analysis, as a result of the converted cases, the survival curve (free of dementia) was higher in the PG (χ2 = 40.2, df = 3, p < 0.001; Fig. 1).

Kaplan-Meier estimate survival by diagnosis: psychiatric group, mild cognitive impairment (MCI), and mild behavioral impairment (MBI). Log-Rank test for the comparison of survival curves upon time, adjusted by age: χ2 = 40.2, df = 3, p < 0.001.
Frequency of conversion to dementia was: MBI group 69.7% (n = 67); MCI group 41.3% (n = 36); and PG 13.9% (n = 23).
According to different degenerative diseases, conversion to dementia was: Alzheimer’s dementia (NINCS-ADRDA criteria [14]): in MCI 83.3% (n = 30), MBI 26.8% (n = 18), and PG 21.7% (n = 5); FTD (Lund and Manchester criteria [15]): in MCI 16.6% (n = 6), MBI 44.7% (n = 30), and PG 30.4% (n = 7); and DLB (DLB International Consortium criteria [16]): in MCI 0%, MBI 28.3% (n = 19), and PG 47.8% (n = 11).
Frequency of conversion to different type of degenerative dementia in each studied group showed a heterogeneous distribution between them (χ2 = 129, df = 6 p < 0.001).
According to different subtypes of psychiatric domains, conversion to dementia was: Anxiety 9.1% (n = 3); Depression 15.2% (n = 10); Psychosis 25.8% (n = 8); and Others 5.7% (n = 2)
Results showed that the distribution of cases that converted to dementia was homogeneous among considered PG subgroups (p = 0.096).
Due to the frequency of NPS in MCI (24.1%), the MCI group was divided in two subgroups: with and without NPS. MCI with NPS symptoms group was defined when at least 1 (one) or more NPS of any domain were found in the NPI. Frequency of conversion to dementia in MCI-with NPS was 52.4% while in MCI-without NPS was 37.8% (Fig. 2).

Kaplan-Meier estimate survival by diagnosis: Psychiatric, mild cognitive impairment (MCI) with and without neuropsychiatric symptoms (NPS), and mild behavioral impairment (MBI) groups. Log-Rank test for the comparison of survival curves upon time, adjusted by age: χ2 = 40.78, df = 3, p < 0.001.
Figure 2 displays Kaplan-Meier analysis adjusted for age showing significant differences between all survival curves as the result of conversion to dementia cases.
Due to the frequency of cognitive symptoms (CogS) found in MBI (27.1%), the MBI group was divided in two subgroups: with and without CogS. MBI with CogS were considered as patients presenting cognitive impairment of more than 1.5 SD in the neuropsychological tests performed after they were included in MBI group. Frequency of conversion to dementia in MBI-with CogS was 65.4% while in MBI-without CogS was 71.5% (Fig. 3).
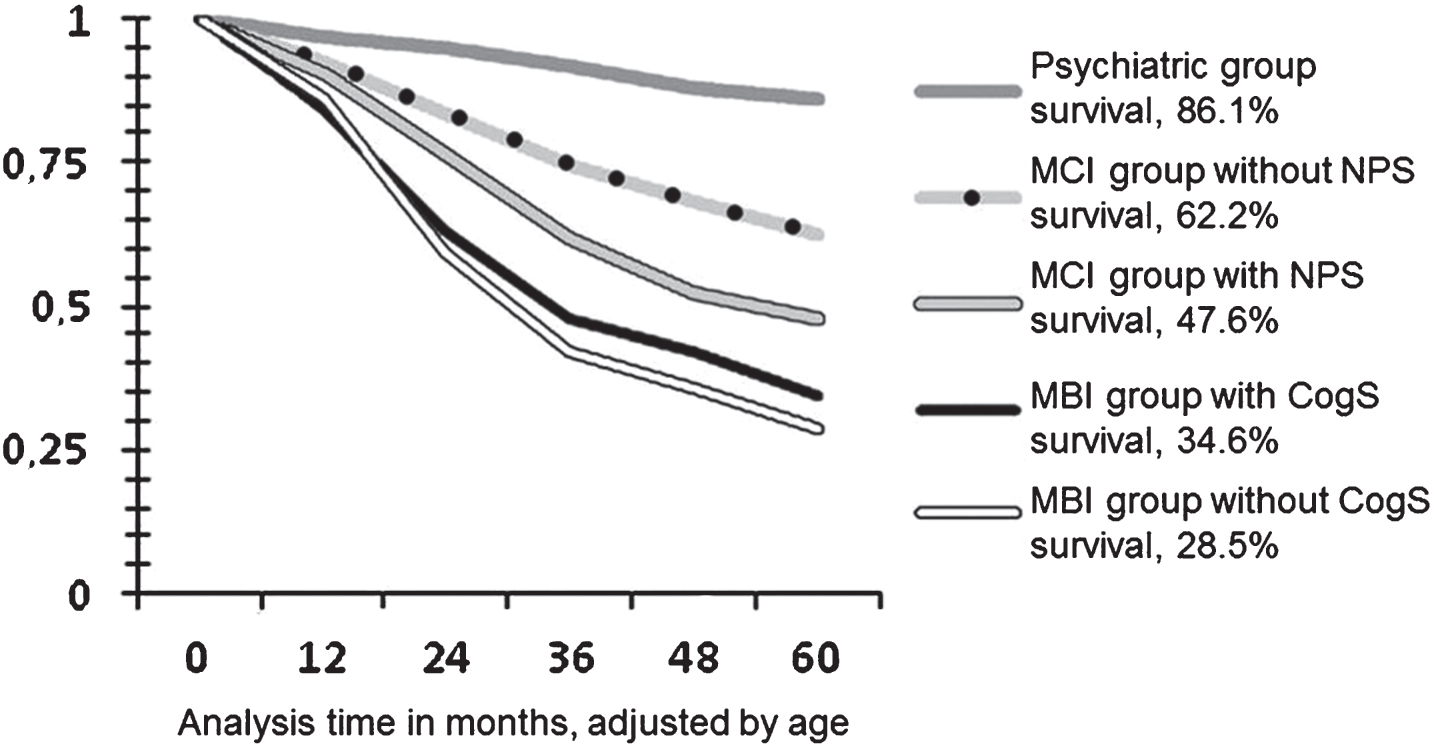
Kaplan-Meier estimate survival by diagnosis: psychiatric group, mild cognitive impairment (MCI) with and without neuropsychiatric symptoms (NPS), and mild behavioral impairment (MBI) with and without cognitive symptoms (CogS). Log-Rank test for the comparison of survival curves upon time, adjusted by age: χ2 = 40.78, df = 3, p < 0.001.
Assuming that MCI with NPS and MBI with CogS could represent the same group or, at least, they should overlap significantly, we regrouped the patients in the following way: MCI, overlapping group (MCI-MBI), MBI, and PG. In this new analysis, we gathered both MCI patients with NPS and MBI patients with cognitive objective impairment: this new group is defined as the MCI-MBI overlap group (Fig. 4).
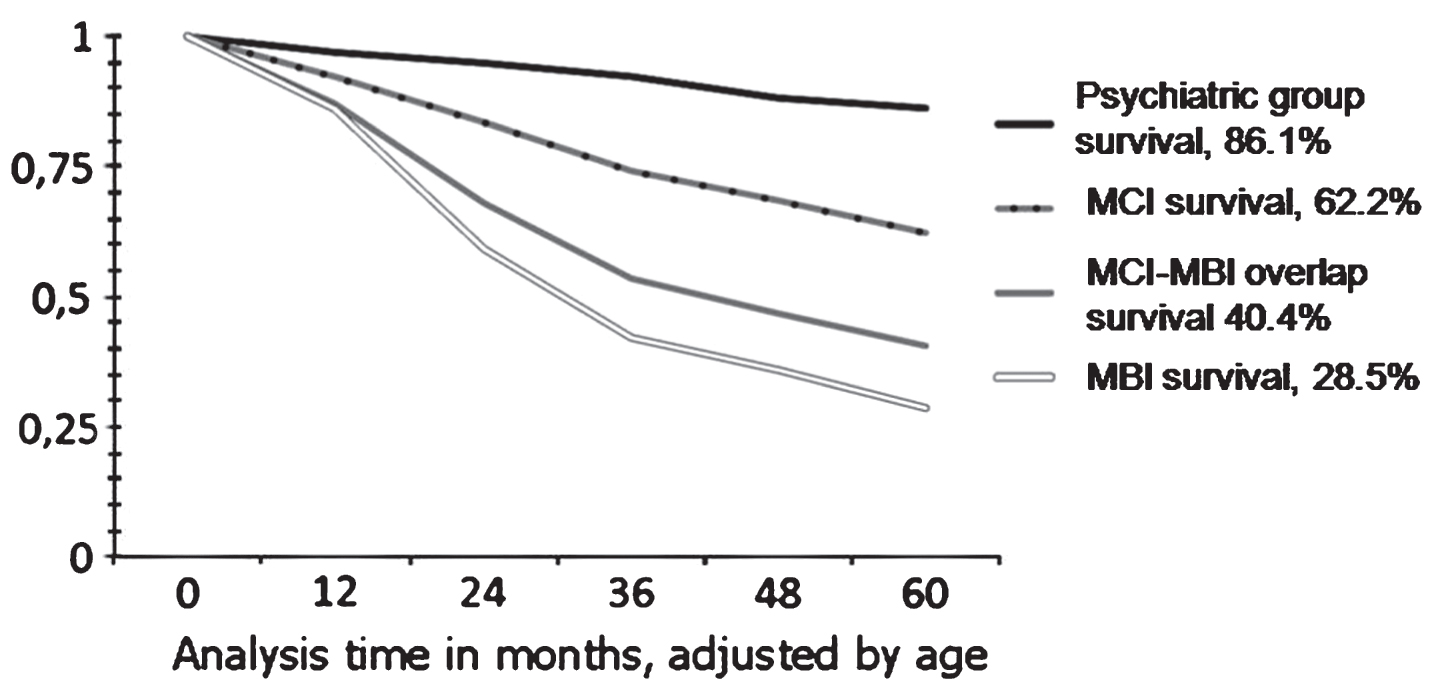
Kaplan-Meier estimate survival by diagnosis: psychiatric group, mild cognitive impairment (MCI), MCI-MBI overlap group, and mild behavioral impairment (MBI). Log-Rank test for the comparison of survival curves upon time, adjusted by age: χ2 = 40.78, df = 3, p < 0.001.
Initial diagnosis and conversion to different types of dementia is depicted in Table 6.
Initial diagnosis and conversion to different types of dementia
Pearson χ2 = 132, df = 15, p < 0.0001.
Discussion
It has long been recognized that behavioral symptoms might be an early manifestation of dementia. In 2003, the International Statistical Classification of Diseases and Related Health Problems (WHO) stated “ ... the impairments of cognitive function are commonly accompanied and occasionally preceded by deterioration in emotional control, social behavior, or motivation ... [30]”.
Since then we have been investigating behavioral changes in elderly patients and their relationship with the development of different types of dementia and, within this context, the concept of MBI was developed as a potential pre-dementia construct.
Identifying an MBI population is a novel approach to study prevention strategies, with the hypothesis that early identification and treatment of behavioral symptoms in neurodegenerative illness could slow or mitigate the presentation of psychiatric complications of dementia. Moreover, the MBI concept may allow current medication or future disease modifying agents to be used earlier in the course of the disease. However, since there is an increased international interest in the MBI concept, as suggested by other authors, it is necessary to be aware of the potential increase of over-diagnosis because of the current lack of evidence showing specific advantages from identifying and targeting MBI [31].
In early 2016, the Alzheimer’s Association International Society to Advance Alzheimer’s Research and Treatment (ISTAART) stated that it was necessary to develop a specifically designed scale for MBI to accurately estimate prevalence and as a later outcome, allow the measurement of preventive therapies [32].
Therefore, ISTAART made explicit the definition of MBI and its differences with MCI. Firstly, the ISTAART MBI criteria requires changes in behavior or personality observed by patient, informant, or clinician, starting later in life (age ≥50 years) and persisting at least intermittently for ≥6 months. Secondly, behaviors are of sufficient severity to produce at least minimal impairment. Thirdly, the impairment in social, occupational, or interpersonal function must be attributable to NPS such as changes in personality and behavior, and not to cognitive decline. Finally, if MBI is diagnosed concurrently with MCI, the functional impairment must be attributed to behavior or personality changes, and not the cognitive impairments, although this may be difficult to ascertain at times. The ISTAART NPS recommends the use of the NIA-AA consensus criteria for MCI and dementia.
Later, the ISTAART expanded on the description of behavioral changes dividing them into five subcategories: motivation, affect, impulse control, social appropriateness, and perception/thought content. MBI subcategories may be correlated with NPI symptoms as follow: decreased motivation (NPI: apathy/indifference); affective dysregulation (NPI: depression/dysphoria, anxiety, elation/euphoria, and irritability); impulse dyscontrol (NPI: agitation/aggression, aberrant motor behavior, and appetite/eating behavior); social inappropriateness (NPI: disinhibition); and abnormal perception/thought content (NPI: delusions and hallucinations).
In accordance with this recommendation, a first scale to measure MBI symptoms has recently been published [33]. The standardization of the assessment of MBI will help to define a target population for new treatment research or potential greater efficacy of older treatments.
In the present study, and as far as we know for the first time in the dementia knowledge field, research was conducted to analyze MBI and MCI patients as well as a psychiatric group (PG) in order to compare their risk of progression to dementia. We followed up 348 patients for a period of five years: 183 suspected of pre-dementia (MCI and MBI) and 165 patients with recognized general psychiatric disorders.
Among considered co-morbidities, significant differences were found between groups. This finding might have importance as there are studies suggesting that, in higher income countries, the incidence of dementia has decreased due to prevention strategies and social changes such as improvement in education and better control of modifiable risk factors [34–36].
Concerning family background, the MBI group was the one who had the highest family history of dementia. Our hypothesis is that MBI patients tend to convert more frequently to FTD and, therefore, they could have more significant family background. On a genetic basis, this could be explained by the fact that approximately 1 to 5% of Alzheimer’s disease (AD) patients could be a consequence of dominant autosomal mutations [37] and, although most cases of FTD are sporadic, 20% to 40% have been described as relatives, most of them presenting an autosomal dominant pattern [38, 39].
Differences found in the neurological exam between groups demonstrate that the MBI group had more neurological signs (pyramidal signs, extrapyramidal signs, and archaic reflexes). Extrapyramidal signs could be explained by pharmacological adverse events, since this group, as it is depicted in Table 2, is the one who significantly used more psychopharmacological medication. Moreover, and regarding all neurological signs, the MBI group presented significant global functional abnormalities and frontal lobe abnormalities in SPECT and PET neuroimages when compared to the other groups. However, there were no significant differences between the MCI and MBI groups with underling vascular disease, and anatomical neuroimaging findings (MRI and CT scan). This matter is not further developed as it is beyond the scope of this paper.
Regarding NPS symptoms, we found that irritability, disinhibition, and delusions followed by depression and apathy were the predominant symptoms in the MBI group, while anxiety and irritability were the most frequent in MCI group.
There are many research studies describing behavioral symptoms of mild type (mostly depressive) associated with MCI [2, 40–43]. The results observed in Beck Depression Inventory in both groups (MCI, MBI) could be related to the fact that this self-administered questionnaire emphasizes more of the cognitive component of depression (decision making, work performance, fatigue/slowing down), since the symptoms of this sphere represent around 50% of the total score of the questionnaire.
Mortby et al. in a recent publication observed that a number of co-morbid NPS in MCI patients and not symptom clusters were associated with increased risk of dementia [44]. These findings highlight the importance of NPS and the need for clinicians to consider the presence of NPS in cognitively normal subjects as a possible risk state.
According to the five subcategories described by the ISTAART about behavioral changes, the symptoms we registered in the MBI group could be related to the following subcategories: affective dysregulation (irritability and depression), impulse control (disinhibition), abnormal perception/thought content (delusions), and decreased motivation (apathy). In the MCI group, observed symptoms (anxiety and irritability) could be classified as affective dysregulation according to the ISTAART criteria.
Although the MBI group included patients with ‘no complaint of cognitive impairment’ by patient/informant, the MBI group had worst cognitive performance in some cognitive domains than the MCI group (for example in MMSE). This might reflect that MBI patients have no awareness and/or perception of their cognitive impairments.
Concerning cognitive symptoms in MCI and MBI groups, MCI is worse on memory impairment while MBI patients with cognitive symptoms performed worse on language domain [Boston Naming Test (p = 0.024) and executive domain (Trail Making B test)].
With regards to the worst performance of MBI patients in the language domain (Boston naming test), one of our hypothesis is that as MBI patients tend to convert in a higher proportion to FTD, some of the cases of FTD could correspond to language variants such as semantic primary progressive aphasia (svPPA). As a recent research study demonstrated that both at baseline and follow-up, svPPA patients exhibited significantly more behavioral disturbances of the type characteristic of behavioral FTD compared with other PPA variants [45].
Moreover, we conducted a research study in PPA patients in 2010 where we observed that patients with PPA may suffer behavioral alterations like apathy, anxiety, and depression, and we wondered if these symptoms could be part of diagnostic criteria of this disorder [46].
Our second hypothesis is that this impairment in language tests in MBI patients could correspond to atypical presentations of AD. Cases of PPA, like semantic dementia with the initial complaint of forgetfulness can be diagnosed as AD [47]. Agrammatic, logopenic, and semantic subtypes, each reflecting a characteristic pattern of language impairment and corresponding anatomical distribution of cortical atrophy, represent the most frequent presentations of PPA. The underlying neuropathology of PPA is, most commonly, frontotemporal lobar degeneration in the agrammatic and semantic forms, while in AD, the logopenic form is the most frequent. AD pathology often displays atypical and asymmetrical anatomical features consistent with the aphasic phenotype [48].
Concerning MBI, worst performance in executive functions; as Cummings and colleagues demonstrated (2004), a high percentage of patients (64%) with AD presented with executive dysfunctional disorder. These performed worse on tests of cognition, dementia severity, and activities of daily living. They also had more frequent symptoms of psychosis at baseline compared with patients with normal executive function [49].
From our total patients, 36.2% converted to dementia. Conversion was significantly higher in MBI 71.5% followed by the MCI-MBI overlap group (59.6%) and MCI (37.8%) group, compared to PG 13.9% (Log-rank p < 0.001).
Our hypothesis for these findings is that patients with NPS symptoms, as early manifestations of neurodegenerative diseases, tend to consult later in the course of the disease. A possible explanation for this idea is that people are generally more concerned about memory problems than in behavioral changes which are usually ignored by the patients or the family members.
From an integrative point of view, the incorporation of neuropsychiatric markers to primary care health may facilitate a synergistic development of preventive interventions. The adoption of the MBI concept along with MCI by the general physician community could lead to an advance in the knowledge of the pre-dementia diagnosis.
Another finding of this research study was that the vast majority of MCI patients tend to convert to Alzheimer’s dementia while MBI patients evolve to a wider range of neurodegenerative diseases, principally FTD, followed by LBD and Alzheimer’s dementia. Instead, patients in the PG evolve to LBD and FTD. Moreover, we observed that all cases of LBD were preceded by NPS (no patients evolved from MCI to LBD).
The strength of our study is the inclusion of the PG that brings novel comparison data for pre-dementia stages of neurodegenerative diseases. The conversion rate to dementia was significantly lower in PG patients (13.9%, p < 0.001) although they present other psychiatric disorders that could predispose to functional impairment or loss of independence. Differentiation between MBI in two subgroups (MBI with and without CogS) and their rate of conversion to dementia is a novel finding.
Our study has several limitations. One of them is that our results are based on a selected group of patients referred for consultation to a dementia unit (Neuropsychiatry Research Unit, CEMIC University Hospital). Another one is that there might be overlap between the MCI with-NPS group described in this research and the MBI with-cognitive impairment group, described in our previous study [13]. Therefore, the “no cognitive complaints criterion” of the MBI diagnosis should be improved in future investigations to better differentiate these groups.
Another limitation to consider is the variability of diagnosis on behavioral impairments due to the different cultural influences. In this way, the report of behavioral symptoms could vary from one population to another but, since our research has been carried out with a homogeneous population, the study maintains cohesion and internal validity.
To conclude, the MBI concept is an advance in the diagnosis of pre-dementia populations and its identification should help in prevention and therapeutic interventions.
This study provides useful data for the diagnosis and management of pre-dementia stages with possible applications for primary care practitioners and other care and social providers in the general population.
Footnotes
ACKNOWLEDGMENTS
The authors wish to acknowledge the economic and scientific support afforded by the National Scientific Research Council (CONICET) from Argentina and the financial assistance of the Neuropsychiatry Research Unit, CEMIC University Hospital, Buenos Aires, Argentina.