
Abstract
Ghrelin is a stomach-derived circulating hormone. In addition to its function as an orexigenic stimulant, the role of ghrelin in the consolidation of learning and memory has been implicated in recent years. However, the status of circulating acylated ghrelin (AG, that is, the functional form of ghrelin) in the symptomatic predementia stage of Alzheimer’s disease (AD) has rarely been investigated. In the current study, we examined the serum levels of acylated and total ghrelin in 22 patients with mild cognitive impairment (MCI) and 30 cognitively normal controls. We have found that patients with MCI had significantly increased serum AG levels, which were inversely associated with defected short- and long-term memory as well as language skills. Of note, the levels of total circulating ghrelin were similar between the two groups. Intriguingly, serum AG but not total ghrelin was associated with AD risk factors including the age, hypertension, and hyperlipidemia. Therefore, circulating AG may serve as a potential early systemic biomarker for AD-related cognitive impairments. Nevertheless, the simplest interpretation of the results is that the levels of circulating AG are associated with cognitive impairments in patients with MCI, thereby forming the groundwork for our future studies on the systemic mechanisms of AD pertaining to the ghrelin system.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a chronic neurodegenerative disorder characterized by progressive learning and memory decline [1]. Although the prevailing opinion is that AD is primarily a neurological disease, increasing evidence has suggested that the etiology and pathology of AD, in particular in its sporadic form, might involve some degree of systemic factors [2]. In this regard, to understand AD pathogenesis and to determine AD biomarkers at a systemics level have been highlighted in recent years. Of note, the diagnosis of AD at a very early stage is of paramount importance for the early control of this chronic disorder. Therefore, it is a long-standing scientific task to recognize systemic biomarkers that reflect the etiology and/or neuronal injury of AD at the mild cognitive impairment (MCI) stage, which is generally considered to be the predementia transition period of AD [3].
Ghrelin, a 28 amino peptide hormone, is a stomach-derived brain-gut peptide that activates the growth hormone secretagogue receptor 1a (GHSR1a) [4]. In addition to its metabolic role in regulating food intake, body weight, and adiposity [5], the non-metabolic function of ghrelin has recently been linked to the synaptic plasticity and transmission of hippocampal neurons [6] and the resultant consolidation of learning and memory [7–10]. Circulating ghrelin exists in the forms of unacylated ghrelin (des-acyl ghrelin or DAG) and acylated ghrelin (AG). Having the ability to cross the brain-blood barrier and to bind GHSR1a [11], AG facilitates learning process and memory [12] and potentiates neurogenesis in hippocampus [13]. Therefore, AG is generally accepted to be the functional form of ghrelin. So far, the relationship of circulating ghrelin and AD is still under debate. Previous studies have shown no change in circulating ghrelin levels in AD patients [14, 15], while some suggested a decrease of the area-under-the-curve (AUC) for total circulating ghrelin in male AD cases [15]. Notably, little is known about the status of circulating ghrelin and its functional form in patients at the MCI stage, which warrants our current study.
MATERIALS AND METHODS
Participants
22 patients with MCI and 30 cognitively normal controls were enrolled from the YangGu Study in the province of Shandong, China. The demographics of the involved subjects including the age, gender, and education levels as well as lifestyle (smoking and alcohol use) were collected. Medical history was obtained via a checklist and self-report questionnaires. The neuropsychological test batteries, including the Fuld object-memory evaluation (FOM), rapid verbal retrieve, auditory verbal learning test (AVLT), digit span, block design, clock drawing task, were administered by trained neurologists. Patients with the following conditions were excluded from the study: psychological disorders, diagnosed stroke, and/or neurodegenerative diseases including Parkinson’s disease, Huntington’s disease, AD, diffuse Lewy body disease, etc., and those taking acetylcholinesterase inhibitors and/or memantine. The diagnosis of MCI was made in accordance to the “Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for mild cognitive impairment due to AD” [3]. Included patients were diagnosed as affected by MCI with the demonstration of impairment in one or more cognitive domains, while their cognitive changes were mild and did not meet the criteria for the diagnosis of dementia. Cognitively normal controls did not have complaints of changes in cognition from their previous levels with no significant impairment in any tested cognitive domains. All the participants were fully informed of the study procedures and signed the consent form. All the procedures were in accordance to the Declaration of Helsinki.
Study protocol
Fast blood was collected in test tubes without anticoagulant. Serum was separated by a centrifugation at 4000 rpm for 10 min. Serum was subsequently stored at –80°C until further analysis. The levels of total ghrelin (Merck #EZGRT-89K), acylated ghrelin (Merck #EZGRA-88K), and insulin (Merck #EZHI-14K and EZHI-14BK) were measured by using commercial ELISA kits by following the manufacturers’ instruction.
Statistical analysis
Categorical variables were presented as frequency (percentage, %), and continuous variables were presented as mean±standard deviation or median based on the condition of normal distribution. Chi-square test or Fisher’s exact test was performed for categorical variables, and Wilcoxon rank sum test was performed for continuous variables between two groups. General linear model was used to investigate the factors that influence serum levels of acylated and total ghrelin, and the correlation between the scores of neuropsychological tests and serum levels of ghrelin. Values of p < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS and SAS for Windows.
RESULTS
Demographic and clinical characteristics of the study subjects
Demographic and clinical characteristics of the study subjects are shown in Table 1. No difference was observed in sex, age, educational levels, history of smoking, alcohol use, hypertension, hyperlipidemia, diabetes, coronary heart disease, and chronic obstructive pulmonary disease (COPD) between the two groups (p > 0.05).
Demographic and clinical characteristics of the enrolled subjects
COPD, chronic obstructive pulmonary disease.
Levels of circulating total and acylated ghrelin in patients with MCI and the controls
To determine whether the risk factors for AD are associated with the levels of total ghrelin and/or AG, some common risk factors for AD were used in our analysis, including sex [16], age [17], education [18, 19], smoking [20, 21], alcohol use [22, 23], hypertension [21, 24], hyperlipidemia [14, 25], diabetes [21, 22], coronary heart disease [26], and COPD [27].
Patients with MCI demonstrated significantly increased levels of circulating AG (Fig. 1, p < 0.001) with similar levels of total circulating ghrelin (Fig. 2, p > 0.05) in comparison with their cognitive function-preserved controls. Accordingly, patients with MCI demonstrated increased ratio of AG to total ghrelin (Fig. 3, p < 0.01). Further analysis of the data showed a strong association of circulating AG with MCI (Table 2, Model 1, p < 0.001). After the adjustment for sex, age, educational level, insulin level, total ghrelin level, smoking, alcohol use, hypertension, hyperlipidemia, diabetes, coronary heart disease, and COPD, AG levels were negatively related to the known AD risk factors including the age (Table 2, Model 2, p < 0.01), hypertension (Table 2, Model 2, p < 0.05), and hyperlipidemia (Table 2, Model 2, p < 0.05), and had a positive relationship with total ghrelin levels (Table 2, Model 2, p < 0.01). In sharp contrast, such correlation was not observed with the levels of total circulating ghrelin (Table 3).
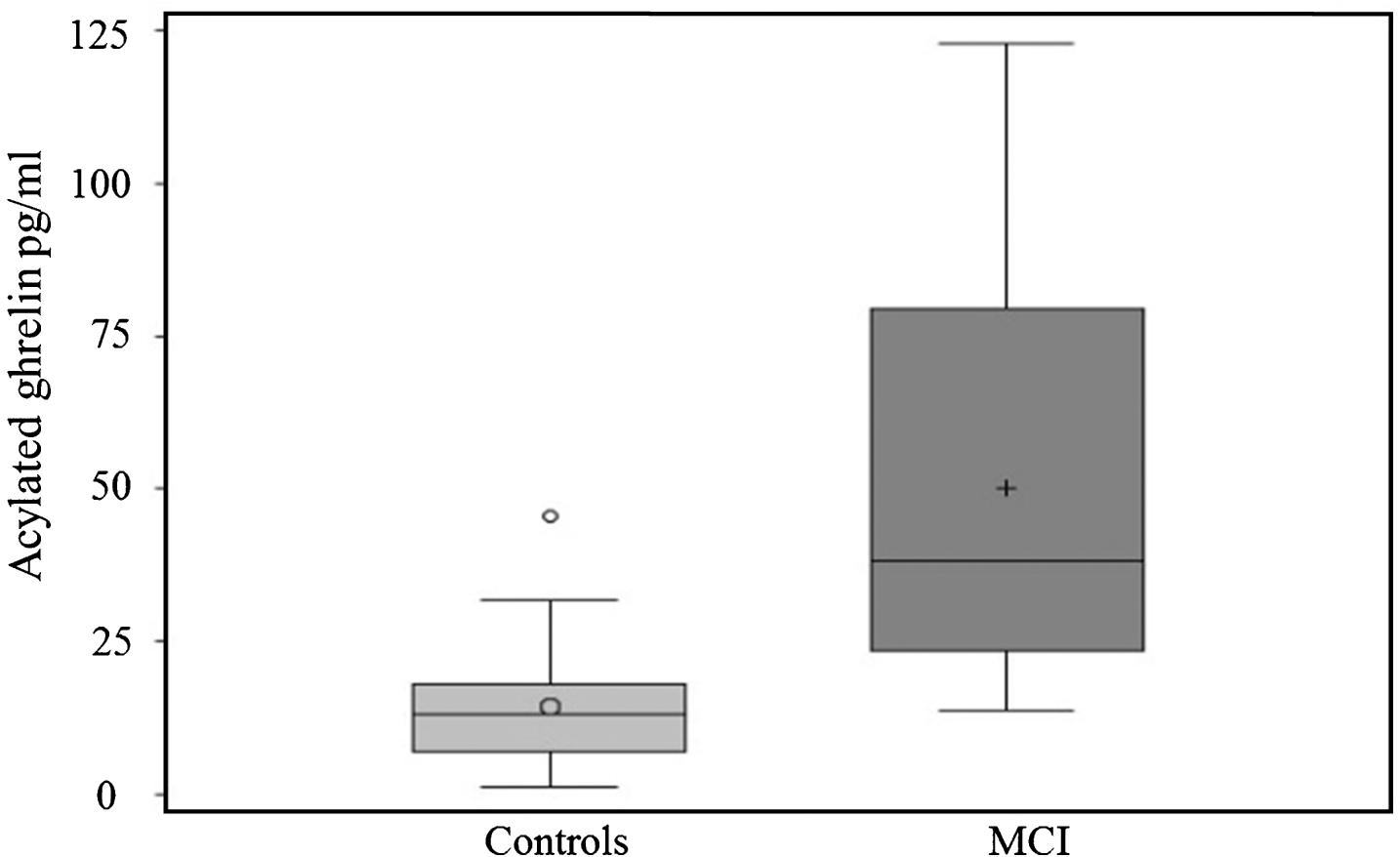
Increased circulating acylated ghrelin in patients with MCI. The data were collected from 22 patients with MCI and 30 cognitive function-preserved controls. p < 0.001.
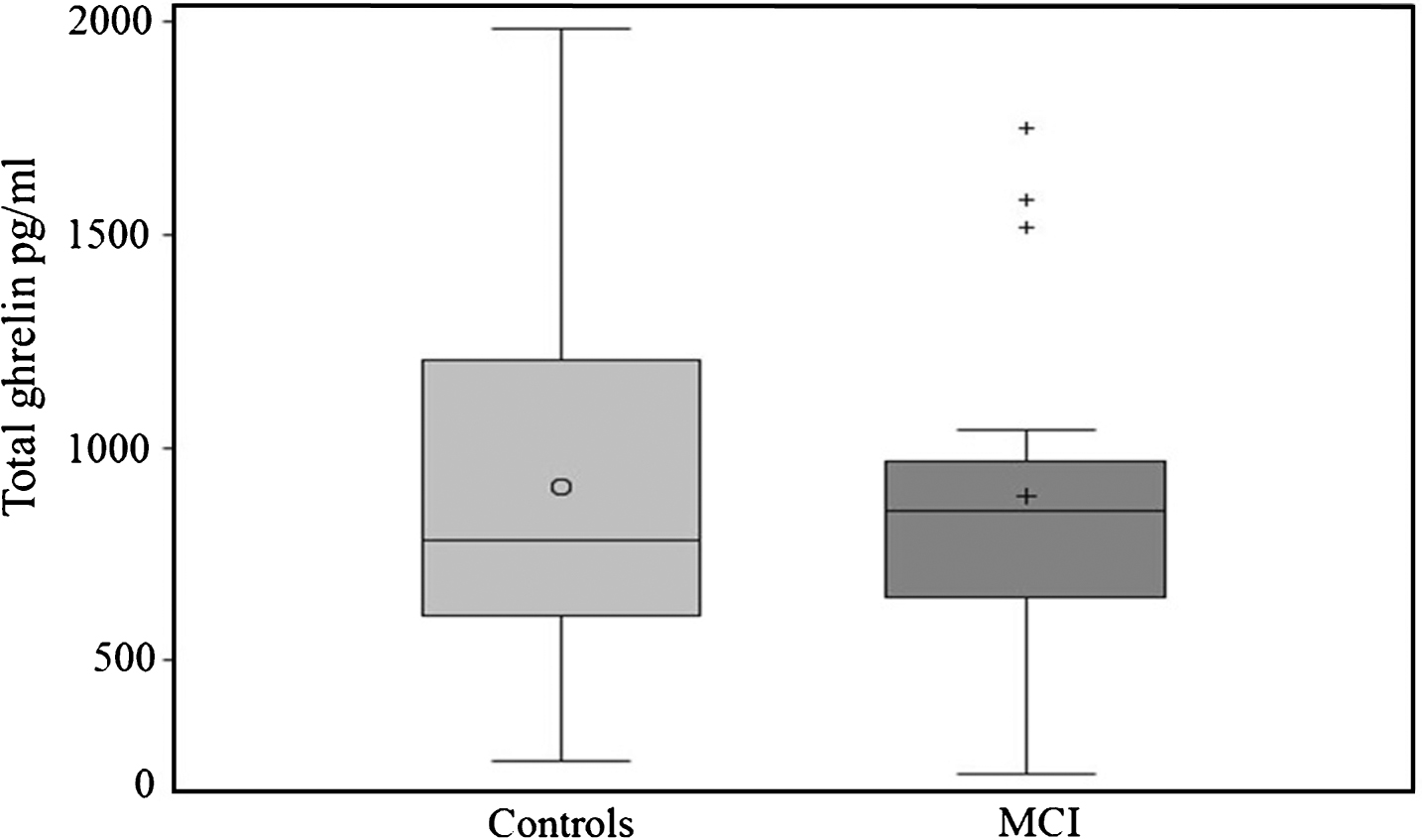
Unchanged total ghrelin levels in patients with MCI. The data were collected from 22 patients with MCI and 30 cognitive function-preserved controls. p > 0.05.

Increased acylated/total ghrelin ratio in patients with MCI. The data were collected from 22 patients with MCI and 30 cognitive function-preserved controls. p < 0.01.
Correlations between acylated ghrelin levels and variables
COPD, chronic obstructive pulmonary disease.
Correlations between total ghrelin levels and variables
MCI, mild cognitive impairment; COPD, chronic obstructive pulmonary disease.
Correlations between circulating ghrelin and neuropsychological performance
To evaluate the correlation between the cognitive function and the serum levels of ghrelin, general linear model was conducted by controlling the variables in different models including no adjustment for variables (model 1), adjustment for sex, age, and educational level (model 2), and adjustment for triglyceride levels based on model 2 (model 3), as well as adjustment for insulin, smoking, alcohol, hypertension, hyperlipidemia, diabetes, coronary heart disease, and COPD, based on model 3 (model 4). Among all the tested neuropsychological measures (Table 4A-C), the analysis showed that after adjusting for the variables AVLT short-term delayed recall (AVLT-SR) scores were negatively associated with AG levels (Table 4A, p < 0.05). Moreover, in all models of FOM and AVLT long-term delayed recall (AVLT-LR), the tests scores were negatively correlated with AG levels (Table 4A, B, p < 0.05). In agreement with the unchanged total ghrelin levels between patients with MCI and the controls, no correlation was determined between the total ghrelin levels with any tested neuropsychological measure except for digit span backward in model 1 and 2 (Table 5A-C). These results indicate that increased levels of AG may be associated with poorer test performance in the aspects of short- and long-term memory as well as language skills, while the levels of total ghrelin may be inversely correlated with attention and short-term memory.
Correlations between acylated ghrelin levels and the scores of FOM, RVR, and AVLT-SR
Correlations between acylated ghrelin levels and the scores of AVLT-LR, CDT, and BD
Correlations between acylated ghrelin levels and the scores of DSF and DSB
FOM, Fuld object-memory evaluation; RVR, rapid verbal retrieve; AVLT-SR, Auditory Verbal Learning Test short-term delayed recall; AVLT-LR, Auditory Verbal Learning Test long-term delayed recall; CDT, clock drawing task; BD, block design; DSF, digit span forward; DSB, digit span backward.
Correlations between total ghrelin levels and the scores of FOM, RVR, and AVLT-SR
Correlations between total ghrelin levels and the scores of AVLT-LR, CDT, and BD
Correlations between total ghrelin levels and the scores of DSF and DSB
FOM, Fuld object-memory evaluation; RVR, rapid verbal retrieve; AVLT-SR, Auditory Verbal Learning Test short-term delayed recall; AVLT-LR, Auditory Verbal Learning Test long-term delayed recall; CDT, clock drawing task; BD, block design; DSF, digit span forward; DSB, digit span backward.
DISCUSSION
Ghrelin is a brain-gut peptide that carries out diverse functions. In addition to its role in the regulation of metabolism and energy homeostasis, recent studies have linked this stomach-derived hormone to critical brain functions including learning and memory, sleep, and some mental state [28]. In the present study, we compared the levels of circulating ghrelin between patients with MCI and the cognitive function-preserved controls. We have found increased circulating AG levels in MCI patients along with no significant difference in the levels of total ghrelin between the two groups. Neuropsychological tests suggest that total ghrelin is negatively associated with short-term memory, which is in agreement with a previous report that serum ghrelin has a negative correlation with verbal delayed recall and recognition, auditory working memory, and confrontation naming cognitive function in cognitively normal elderly [29]. Of note, in comparison with total ghrelin circulating, AG has a stronger inverse relationship with a wider range of cognitive domains including the short- and long-term memory as well as language skills, implying that AG elevation is a more sensitive indicator in reflecting defective cognitive performance. However, such findings seem to contradict the observation of ghrelin supplementation in improving hippocampal function as well as neurogenesis in an AD mouse model [30]. Given ghrelin exerts the function through the activation of its receptor, GHSR1a, we thus speculate the deregulation of GHSR1a in central nervous system (CNS) may underlie such a discrepancy. Indeed, a previous study on biopsied AD brains found significantly decreased GHSR1a along with increased GHSR1b at both gene and protein expression levels in the AD temporal lobe [31]. In view that GHSR1a is activated by AG and GHSR1b blunts GHSR1a function, this finding implicates perturbations in CNS ghrelin receptor in the AD pathological setting. Since MCI is the predementia state which has a high chance to develop into AD dementia, it cannot be excluded that ghrelin receptor deregulation as seen in AD may also occur in MCI subjects though to a less rigorous degree. In this regard, the elevation of circulating AG in MCI cases is probably a compensatory systemic change in response to the ghrelin receptor deficits. In this scenario, it is not surprising that the supplementation of ghrelin at the relatively high dose may exert protective effect on the AD mice. Moreover, although DAG has been considered to be an inert form of ghrelin, recent studies have suggested that DAG has its metabolic function by antagonizing the effect of AG and/or regulating the activation status of ghrelin [32]. Of note, in the current study we have found that the ratio of AG to total ghrelin is increased in MCI patients. Given the unchanged levels of total ghrelin, the results further implicate, although indirectly, lowered levels of DAG in patients with MCI. It is not yet clear whether such changes in DAG may potentially contribute to cognitive deficits. However, given the low affinity of DAG to bind GHSR 1a [32], DAG is unlikely to block GHSR 1a at its physiological concentration. In this case, lowered DAG levels may be just a systemic response to ghrelin activation; otherwise, lowered DAG levels may serve as a driving factor for AG elevation in response to systemic metabolic changes, some AD risk factors, and/or hippocampal synaptic injury. The above questions will be investigated in our future studies.
Another interesting finding merits discussion is the negative correlation of circulating AG with AD risk factors including the age, high blood pressure, and hyperlipidemia. This might be associated with the metabolic function of ghrelin. Previous studies have shown that the ratio of acylated to DAG decreased with age and attribute such change to lowered energy metabolism during the aging process [33]. Indeed, loss of appetite and under-eating are common in the aging population, in particular in those with cognitive impairments and AD dementia. Furthermore, ghrelin plays a critical role in the regulation of body adiposity and blood pressure. The negative correlation of AG with hypertension and hyperlipidemia that we found in this study seems to suggest that defected ghrelin activation by acylating modification underlies the systemic AD risk factors including high blood pressure and lipid dysmetabolism. In this scenario, we propose that lowered ghrelin activation but not total ghrelin levels is a promoting factor for the development of AD. This has raised an intriguing scientific question, that is, how to reconcile the positive association of AG with cognitive impairments with the negative association of AG with AD risk factors. We hypothesize that given aging is the greatest AD risk factor, the aging process implements a strong inhibition of systemic ghrelin activation; while AG elevation is a compensatory response to CNS ghrelin receptor deregulation in MCI patients. Indeed, such hypothesis needs further validation in our future study on the molecular mechanisms of ghrelin system perturbations in patients at the predementia and AD dementia stages.
In summary, in this study we have provided direct evidence showing the strong correlation of increased circulating AG with defects in several cognitive domains in patients with MCI. Such finding suggests that AG is a potential systemic biomarker at least for patients at the symptomatic predementia stage and implicates the involvement of the deregulation of ghrelin system, particularly the ghrelin receptors in the hippocampal region, in the development of cognitive impairments related to AD dementia. Indeed, the relative small size of enrolled subjects and the lack of further mechanistic study at the molecular levels are limits of this study. We will continue our study by enlarging the sample size in a future cohort study, which will allow us to take several variables including the body weight, body adiposity, and other metabolic hormones as well as eating/appetite disorders into consideration. Moreover, the molecular mechanisms underlying ghrelin system changes in MCI and/or AD patients will be emphasized in our further investigation. Nevertheless, the most parsimonious interpretation of the results is that the levels of circulating AG are potentially associated with cognitive impairments in patients with MCI, thereby forming the groundwork for our future studies on the systemic mechanisms of AD pertaining to the ghrelin system.