
Abstract
Background:
Adynamic speech is characteristic of progressive supranuclear palsy (PSP), but higher language deficits have been reported inconsistently, in the context of clinical and pathological overlaps with progressive non-fluent aphasia (PNFA).
Objective:
The present study tested two hypotheses: 1) PSP and PNFA display impaired single word repetition, object naming, semantic knowledge, and syntactic comprehension; and 2) PSP have reduced speed on timed cognitive tasks.
Methods:
Structured clinical and neuropsychological assessments of language were performed on patients with clinically defined PSP and PNFA. Language was tested using the Sydney Language Battery (SYDBAT) and the Test of Reception of Grammar (TROG).
Results:
In total, 144 participants were studied (PSP 22, PNFA 29, and Control 93). PSP patients had prominent eye movement abnormalities, parkinsonism, and falls. All 4 PSP patients who underwent postmortem examination had 4-Repeat tauopathy, with PSP pathology in 3. The frequency and severity of impairment on the SYDBAT (naming, word comprehension, semantic association), and TROG (syntactic comprehension) did not differ between PSP and PNFA, but PSP were significantly slower on timed non-language cognitive tests.
Conclusion:
Tested formally, aphasia may be seen in PSP, with a severity similar to that seen in PNFA.
Keywords
INTRODUCTION
Progressive supranuclear palsy (PSP) was originally described by Richardson and colleagues (1963) as a parkinsonian disorder characterized by axial rigidity, symmetrical bradykinesia, postural instability, and conjugate gaze paralysis on voluntary eye movement [1, 2]. Over time, movement-based speech and bulbar disturbances were recognized as integral components of the syndrome. In particular, rigidity and bradykinesia affecting bulbar muscles was found to cause dysphagia and hypokinetic dysarthria, with spastic and ataxic dysarthria described less commonly [3–5].
More recently, impaired language production abilities have been reported in so-called atypicalpresentations of PSP. Although large scale systematic studies are lacking, case reports and small case series have described an “adynamic” aphasic syndrome in PSP, characterized by a reduction in verbal output and selective impairment of action verbs, accompanied by reduced cognitive processing speed [5–13]. Other aspects of language, such as single word or sentence repetition and syntactic comprehension [6, 14–17] are thought to be relatively preserved. The overlaps between non-fluent aphasia and PSP are not discussed in the international consensus criteria of primary progressive aphasia (PPA) [18], although recent clinical criteria for the diagnosis of PSP now recognize a speech/language phenotype of thedisease [19].
Progressive non-fluent aphasia (PNFA) is characterized by non-fluent language production and may overlap with PSP in several clinical and pathological respects. For example, apraxia of speech (AOS), which may occur in isolation or as a feature of PNFA, is associated with the eventual development of extrapyramidal signs and/or underlying 4-repeat tauopathy, including pathological PSP [19–27]. Furthermore, patients with PNFA can develop a typical PSP motor syndrome throughout the course of their illness [26]. Finally, PNFA patients may have underlying PSP pathology even in the absence of AOS or PSP motor phenotype in life [20, 27]. These clinical and pathological observations argue against a dogmatic distinction between PSP and PNFA. Furthermore, the pathology of PNFA is heterogeneous, and better biomarkers of specific pathological entities, such as pathological PSP, are needed.
The purpose of the present study was to examine language in PSP and PNFA patients using clinical assessments and neuropsychological tools that were developed to categorize the typical deficits of PNFA. Specifically, we sought to establish whether single word repetition, object naming, semantic knowledge, and syntactic comprehension distinguished PSP from PNFA. Furthermore, we explored whether performance on language tasks correlated with executive abilities. Finally, we sought to examine processing speed on timed cognitive tasks, to determine whether this feature distinguished PSP and PNFA. The following hypotheses were proposed: 1) that PSP aphasia shares many clinical features with PNFA, both being impaired on tests of single word repetition, object naming, semantic knowledge, and syntactic comprehension, but that 2) PSP patients also would have reduced speed on timed non-linguistic cognitive tasks.
MATERIALS AND METHODS
Participants
Consecutive patients with PSP (n = 22) and PNFA (n = 29) were recruited from Frontier, a frontotemporal dementia specific research clinic based at Neuroscience Research Australia (NeuRA, now based at Brain and Mind Centre). The clinic sees a wide range of patients presenting with behavioral, cognitive, and aphasic disorders that are often combined with motor problems. The diagnosis of PSP was made on clinical grounds in accordance with consensus research diagnostic criteria [28, 29], which emphasize motor deficits. These older criteria require a progressive illness, falls early in the course of the disease, and vertical supranuclear gaze palsy or slowing of vertical saccades. Supportive features include symmetric proximal akinesia or rigidity, poor levodopa responsiveness, early dysphagia and dysarthria, and early onset of cognitive impairment. Most PSP patients met criteria for the diagnosis at the initial assessment, although characteristic signs (e.g., gait disturbance, falls, or eye movement abnormalities) developed later in the disease course in a small proportion of patients. The results reported in the present study represent the findings on the initial assessment. The results of language assessment, and formal language tests, were not considered when making the clinical diagnosis of PSP. Pathological diagnoses were available for four cases with clinical diagnosis of PSP. Patients with PNFA exhibited agrammatism and/or impaired syntactic comprehension, despite spared single-word comprehension and object knowledge and variable degree of motor speech apraxia [18]. Patients with primary progressive AOS but no aphasia were excluded from the present study [22].
Where necessary, blood and cerebrospinal fluid examinations were performed to exclude autoimmune or inflammatory disorders. Cerebrospinal fluid markers of Alzheimer’s disease pathology were not routinely tested and amyloid imaging was not part of the imaging protocol. In addition, patients were excluded from the study if they had insufficient command of the English language (used to perform language testing) or if language/cognitive deficits were so severe that detailed testing could not be completed. Patients with a severe burden of vascular disease (e.g., multiple large vessel cortical strokes) were excluded, but minor white matter changes were permitted. Finally, patients with a longstandinghistory of drug and alcohol abuse, major head injury, significant psychiatric co-morbidity, probable Alzheimer’s disease, idiopathic Parkinson’s disease, corticobasal syndrome, or multiple system atrophy were also excluded.
Control participants were recruited from a database of healthy research participants held at NeuRA. All Control participants were free of significant neurological disease at the time of inclusion in the study and performed normally on extensive neuropsychological testing.
Ethical approval for the study was obtained from the South Eastern Sydney Local Health District and the ethics committee of the University of New South Wales. Informed consent was acquired in accordance with the Declaration of Helsinki. If a patient was unable to give informed consent, the patient’s next of kin consented on their behalf.
Clinical assessments
Patients underwent detailed clinical evaluations by experienced behavioral neurologists (JRB or JRH) to assess patients and caregivers on a range of language, cognitive (memory, executive, visuospatial, etc.), and behavioral symptoms. More specifically, language disturbance was examined using a pre-determined series of questions. Symptoms such as word-finding difficulties, misuse of words, comprehension problems, reading problems, and dysgraphia were documented as “present” or “absent”. The presence of adynamism was specifically sought by asking patients and carers whether verbal content and initiation had reduced. In addition, all underwent structured clinical assessment of speech and language abilities, to examine features such as slowed speech, dysarthria, apraxia of speech, phonological errors, syntactic deficits, word-finding difficulties, anomia, single word and sentence repetition, single word and sentence comprehension, surface dyslexia, and dysgraphia [30, 31].
Neurological examination sought signs of parkinsonism, eye movement abnormalities, gait disorder, and impaired righting reflexes. All symptoms and signs were recorded as “present” or “absent”.
Neuropsychological assessment
Formal cognitive screening was performed using the Addenbrooke’s Cognitive Examination (ACE). Most patients completed the second iteration of the ACE, known as the ACE-R [32], but more recent cases completed the third version of the task known as the ACE-III [33]. Importantly, performance on the ACE-III has been shown to correlate tightly with performance on the ACE-R [33]. In addition to providing a general measure of cognitive performance, both versions of the ACE assess five cognitive domains, including: attention (18 points), memory (26 points), verbal fluency (14 points), language (26 points), and visuospatial ability (16 points). A total score below 88/100 detects dementia with high sensitivity and specificity on the ACE-R and the ACE-III [32, 33].
Language deficits were examined in further detail using two commonly used tools for the neuropsychological assessment of aphasic syndromes. Specifically, the Sydney Language Battery (SYDBAT), which was developed for use in progressive aphasia [34], was used to assess confrontational naming, single word repetition, word comprehension, and semantic association separately, with performance on each subtest scored out of 30 points. Interpretation of grammar was assessed using the Test for the Reception of Grammar (TROG) [35], which is a sentence-picture matching task that examines interpretation of different type and complexity of syntactic structures. To complete the task, the subject is required to select the best graphical representation of a given sentence, from an array of four possibilities. The TROG includes 20 blocks of four sentences each, with difficulty increasing as the test proceeds [35]. The TROG total is scored out of 80 points.
The SYDBAT and TROG are untimed, therefore the Trail making test (Parts A and B) and the Rey-Osterrieth Complex Figure copy, which are timed, were used to assess cognitive processing speed. In Part A of the Trail Making Test the subject joins circles labelled with consecutive numbers (i.e., “1”, “2”, “3” etc.) in sequence, and the time taken to complete the task is recorded. Part B of the Trail Making Test is like Part A, but the subject joins numbers alternating with consecutive letters (i.e., “1”, “A”, “2”, “B”, “3”, “C” etc.) in sequence. The Rey-Osterrieth Complex Figure task requires the copy of a complex drawing. The time taken to produce the copy and the accuracy of the copy are recorded. The second component of the task requires the subject to produce a copy of the complex figure from memory.
Neuropathological classification of PSP
Patients were enrolled in the Frontier brain donor program (approved by the Human Research Ethics Committees of the South Eastern Sydney Local Health District) and the brains collected by the Sydney Brain Bank (approved by the Human Research Ethics Committees of the University of New South Wales). Standardized neuropathological characterization was performed [36] and recommendations from previously published neuropathological criteria for FTLD-tau used [37–40] following assessment of neuronal loss and gliosis in a variety of sections (hematoxylin and eosin, modified Bielschowsky silver-staining, immunohistochemistry). For the immunohistochemical localization of the tau protein, the antibody used was for phosphorylated tau (clone AT8; mouse; 1 : 1000; Cat. No. MN1012; Thermo Scientific Australia, Scoresby, Victoria) utilizing a Discovery DX autostainer (Ventana Medical Systems, Tuscon, AZ, USA), peroxidase chromogen and hematoxylin counter-staining.
Statistical analysis
Univariate statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, version 23.0, IBM Corp, Armonk, NY, USA). Group comparisons of continuous variables were analyzed using analysis of variance (ANOVA) when normally distributed or the Kruskal–Wallis test when non-normally distributed. Pairwise comparisons were performed using the independent samples t test when continuous variables were normally distributed and the Mann-Whitney test when non-normally distributed. Categorical data were analyzed using the Chi-Square test. To correct for up to 50 comparisons, a Bonferroni correction was used to determine a significance threshold of p < 0.001. Impaired performance on continuous measures was defined as a score < 2 standard deviations below the control mean for that particular measure. Continuous data is presented as mean±standard deviation.
RESULTS
Patient demographics and cognitive screening
In total, 144 participants were included in the study (PSP 22, PNFA 29, and Control 93). The groups did not significantly differ in age (PSP 71.5±6.1 years; PNFA 70.8±10.3 years; Control 71.5±7.8 years, p = 0.942) and male sex (PSP 50%; PNFA 37.9%; Control 40.9%, p = 0.82).
In terms of cognitive screening, both disease groups were impaired on the ACE compared to the Control group, although the pattern of deficits differed. As presented in Table 1, both groups were impaired on all subtasks of the ACE, as well as the ACE total, compared to Control (all p < 0.001). In addition, the PSP group performed worse on the visuospatial subtask than the PNFA group (PSP 12.5±2.8; PNFA 14.8±1.5, p = 0.001). In contrast, there was a trend for worse performance on the language subtask in the PNFA group (PSP 22.3±3.5; PNFA 19.8±4, p = 0.01).
Demographics and cognitive screening of participants with progressive supranuclear palsy (PSP), progressive non-fluent aphasia (PNFA), and Controls
PSP, PNFA, and Control groups were matched in age and gender. PSP and PNFA groups were impaired on the ACE compared to the Control group, but the pattern of deficits differed; PSP performed worse on the visuospatial subtask than PNFA, while PNFA performed worse on the language subtask. Number (percent) or Mean (SD); NS, non-significant.
Clinical history
Of the 22 patients diagnosed with PSP, 7 (35%) had language symptoms before the development of the characteristic movement disorder and 6 (30%) had a movement disorder before the development of any cognitive/behavioral symptoms. Of the remainder, 5 (25%) reported mixed cognitive/behavioral and movement disorder symptoms and signs as the initial symptoms, while 2 (10%) had a behavioral onset to their symptoms. In 2 (10%) patients, the initial symptom could not be determined.
Almost all patients reported language disturbances at the time of first assessment (PSP 92.9%; PNFA 100%, p = 0.194). In addition, both groups reported a similar frequency of symptoms suggestive of executive dysfunction (PSP 35.7%; PNFA 21.7%, p = 0.353), but report of visuospatial disturbances was generally infrequent (PSP 7.1%; PNFA 13%, p = 0.575). Although motor symptoms were reported in both disease groups to some extent, significantly more PSP cases reported gait disturbance (PSP 66.7%; PNFA 9.5%, p < 0.001), falls (PSP 86.7%; PNFA 14.3%, p < 0.001), or impaired balance (PSP 86.7%; PNFA 9.5%, p < 0.001). There were trends for more slow movement (PSP 60%; PNFA 14.3%, p = 0.004) and micrographia in PSP (PSP 46.7%; PNFA 5%, p = 0.004).
On more specific questioning of speech and language symptoms, both groups reported similar rates of word-finding difficulties (PSP 76.9%; PNFA 87%, p = 0.438) and dysgraphia (PSP 69.2%; PNFA 65.2%, p = 0.806). The most frequent language symptom reported in PSP was adynamism— defined here as reduced verbal content or spontaneity (PSP 92.3%; PNFA 56.5%, p = 0.025), whereas significantlymore PNFA cases reported misuse of words (PSP 15.4%; PNFA 82.6%, p < 0.001) and a trend for morecomprehension problems (PSP 0%; PNFA 34.8%, p = 0.02).
Clinical examination
On clinical assessment, language impairment at initial assessment was common among both disease groups (PSP 86.7%; PNFA 100%, p = 0.048). As presented in Table 2, rates of dysarthria, slowed speech, anomia, single word/sentence comprehension difficulties, and surface dyslexia were similar in both groups (all p > 0.178). As might have been predicted, there were trends for more severe word-finding difficulties, apraxia of speech, syntactic errors, and phonological substitutions in spontaneous speech in PNFA (all p < 0.045). In addition, patients with PNFA were more frequently impaired on sentence repetition (p < 0.001) with a trend for impaired single word repetition (p = 0.002) and greater dysgraphia (p = 0.005). No single language feature distinguished the PSP group on clinical examination.
Bedside examination of aphasia for participants with progressive supranuclear palsy (PSP) and progressive non-fluent aphasia (PNFA)
Language impairment was almost universal among both disease groups. Rates of dysarthria, slowed speech, anomia, single word/sentence comprehension difficulties, and surface dyslexia were similar in both groups, but patients with PNFA exhibited more word-finding difficulties, apraxia of speech, syntactic errors, phonological substitutions in spontaneous speech, and impairment on single word and sentence repetition tasks. No single language feature distinguished the PSP group on bedside examination. Number (percent); NS, nonsignificant; all p-values <0.05 are shown.
Patients with PSP had more motor deficits on initial examination than those with PNFA. Specifically, gait disorder (PSP 86.7%, PNFA 7.1%, p < 0.001), postural instability (PSP 75%, PNFA 11.1%, p < 0.001), eye movement abnormalities (PSP 81.3%, PNFA 3.6%, p < 0.001), and parkinsonism (PSP 66.7%, PNFA 10.7%, p < 0.001) were all more common in PSP at first examination than in PNFA. In terms of parkinsonian signs, bradykinesia was the most frequent finding (PSP 76.9%, PNFA 13.6%, p < 0.001), followed by rigidity (PSP 61.5%; PNFA 0%, p < 0.001).
Neuropsychological assessment of language abilities
At a group level, both the PSP and PNFA groups demonstrated evidence of aphasia on formal testing, with impaired performance on all components of the SYDBAT and on the TROG compared to Controls (See Table 3). Specifically, both groups were significantly impaired relative to controls on the naming (both p < 0.001) and single word repetition (both p < 0.001), with trends for impairment on comprehension (both p < 0.015) and semantic association (both p < 0.002) sections of the SYDBAT (See Fig. 1). The frequency of impaired performance on the SYDBAT sections, defined as a score < 2 SDs from the control mean, was similar for both patient groups for naming (PSP 36.4%, PNFA 44.8%, p = 0.543), semantic association (PSP 18.2%, PNFA 20.7%, p = 0.823), and comprehension (PSP 27.3%, PNFA 20.7%, p = 0.53). There was a trend for a difference in single word repetition between the two groups, with relatively preserved performance in the PSP group compared to PNFA (PSP 26.7±5.5; PNFA 20.5±5.5, p = 0.006). Consistent with this finding, impaired performance was more frequent in PNFA (86.2%) patients than in PSP (31.8%, p < 0.001).
Neuropsychological assessment of language for participants with progressive supranuclear palsy (PSP), progressive non-fluent aphasia (PNFA), and Controls
The PSP and PNFA groups demonstrated evidence of aphasia on formal testing, with impaired performance on all components of the Sydney Language Battery (SYDBAT) and the Test of Reception of Grammar (TROG) compared to Controls. Specifically, both groups were impaired on the naming, repetition, comprehension, and semantic association sections of the SYDBAT. Single word repetition was relatively preserved in PSP compared to PNFA. Both PSP and PNFA demonstrated impaired syntactic comprehension compared to Controls, but, there were no significant differences in TROG performance between the PSP and PNFA groups.
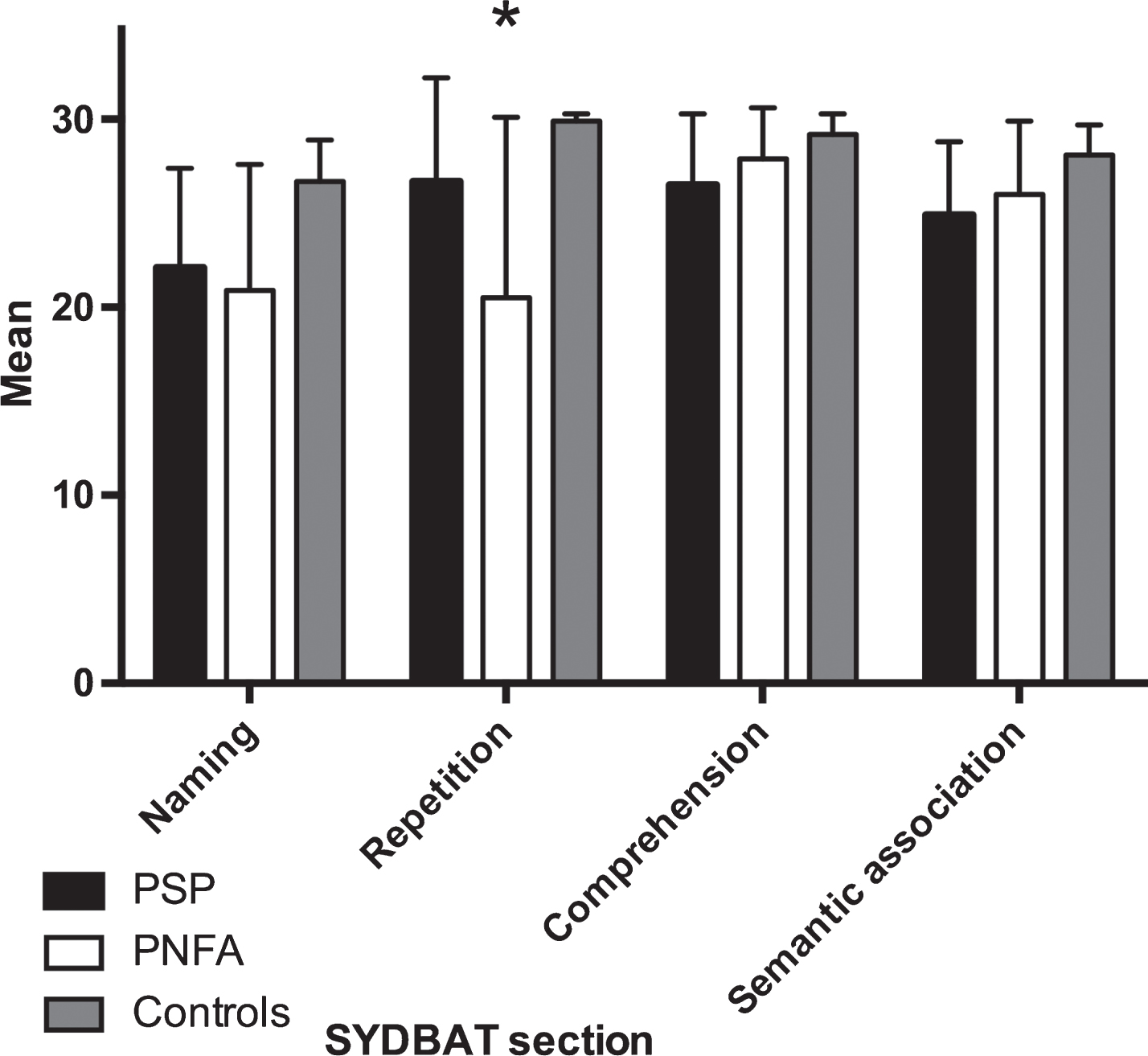
Average performance on subtests of the Sydney Language Battery (SYDBAT) in participants with progressive supranuclear palsy (PSP), progressive non-fluent aphasia (PNFA), and Controls. PSP and PNFA groups demonstrated impaired performance on all components of the SYDBAT. Both groups were significantly impaired on the naming (both p < 0.001), repetition (both p < 0.001), comprehension (both p < 0.05) and semantic association (both p < 0.05) sections of the SYDBAT. Compared to PNFA, PSP patients were relatively preserved on single word repetition (*p < 0.05). Error bars represent standard deviation.
Finally, the PSP and PNFA groups both demonstrated evidence of impaired syntactic comprehension on the TROG. Both patient groups had a significant reduction in the number of total blocks correct (PSP 13±4.9; PNFA 12.3±4.4; Controls 18.4±1.4, p < 0.001), with a trend for group difference in TROG total correct (PSP 67.7±11.3; PNFA 64.6±12.8; Controls 69.1±16.5, p = 0.006). There were no significant differences in TROG performance between the PSP and PNFA groups, and the proportion of PSP patients impaired on the TROG total score (defined as <2 SD below control mean) was not different from that of PNFA patients.
Neuropsychological assessment of non-language cognitive abilities
The PSP and PNFA groups demonstrated evidence of impaired executive function compared to controls. As demonstrated in Table 4, both disease groups were significantly (p < 0.001) impaired on verbal letter fluency compared to Controls, but there was no difference between PSP and PNFA. The PSP group produced significantly more errors on the Trails test (section B) than Controls (p < 0.001), with a trend for more errors in PSP than PNFA (p = 0.003). Both PSP and PNFA groups demonstrated significant impairment compared to Controls on working memory tasks (p < 0.001), such as digit span, but there was no significant difference between the two disease groups. There was a significant group difference in the RCF copy score (p < 0.001), driven by significant impairment in PSP (p < 0.001), and a trend for impaired performance in PNFA (p = 0.042), compared to Controls. In addition, there was a trend for disproportionate impairment on the RCF copy score in PSP compared to PNFA (p = 0.008).
Neuropsychological assessment of non-language cognitive abilities for participants with progressive supranuclear palsy (PSP), progressive non-fluent aphasia (PNFA), and Controls
Intergroup differences were noted for all tasks, except for a trend in RCF copy time. PSP patients were significantly impaired on the RCF copy score and copy time compared to PNFA, but did not differ from PNFA on any other measure.
One of the most striking findings was a profound reduction in cognitive processing speed in PSP patients on several tasks where a timed component was included. For example, PSP patients were significantly (p < 0.001) slower in completing the Trails B task than Controls, with a trend (p = 0.011) for slower performance compared to PNFA patients. Similarly, there was a trend (p = 0.009) for group difference in RCF copy time, with trends for slower performance in PSP compared to controls (p = 0.004) and PNFA (p = 0.018); there was no difference in RCF copy time in PNFA compared to controls. Among PSP patients, there was a trend for correlation between performance on SYDBAT semantic association and Trails B time (r = –0.711, p = 0.014) and between SYDBATrepetition and Digit span backwards (r = 0.586, p = 0.022), but neither satisfied the corrected threshold for significance of p < 0.001. There were no other significant correlations between SYDBAT subtests and performance on non-language cognitive tasks. Trends for correlation between the TROG total correct score and the Trails B time (r = –0.717, p = 0.03) and Trails B errors (r = –0.694, p = 0.038), but neither satisfied the corrected threshold for significance of p < 0.001. There were no other significant correlations between the TROG and non-language cognitive tasks in the PSP group.
Pathology
Pathological diagnoses were available on four patients who had been diagnosed with PSP clinically during life. All cases demonstrated evidence of a 4-repeat tauopathy. In three, the diagnosis was pathological PSP and the fourth case met pathological criteria for corticobasal degeneration.
DISCUSSION
The present study, the first systematic comparison of PSP and PNFA patients, demonstrated that true aphasia is a prominent feature of PSP, with deficits on clinical and neuropsychological language assessments similar in quality and quantity to those seen in PNFA. Patients with PSP demonstrated an equivalent degree of impairment to PNFA patients on tasks assessing object naming, single word comprehension, and semantic association. Surprisingly, the PSP group was as impaired on a syntactic comprehension task as the PNFA group, even though impaired comprehension and production of syntax are defining features of PNFA. Furthermore, reduced speed on timed non-language cognitive tasks was particularly common in PSP patients. Overall, the results are in keeping with the emerging recognition of clinical and pathological overlaps between PSP and PNFA. Better measures of adynamism should be explored [9, 10] as potential markers of PSP pathology in patients who present with non-fluent aphasia, including otherwise typical cases of PNFA.
Before further discussion of the results of the present study, it is important to recognize the potential referral bias affecting inclusion of PSP patients. Specifically, roughly one third of patients reported a movement disorder, gait instability, or falls as their initial symptom; most patients included in the present PSP group showed cognitive and behavioral symptoms initially, rather than motor symptoms of PSP. As such, our cohort of PSP patients may over-represent the frequency of cognitive deficits, and language disturbances more specifically, compared to PSP patients seen and exclusively managed in movement disorder clinics. For example, one very recent population based study, reported an incidence of language disturbance in only 27.1% of PSP patients [41], compared with 86.7% of patients who had some degree of language impairment on clinical assessment and up to 36.4% of patients with impaired performance on formal language testing in our study. In addition, the present study excluded patients with primary progressive apraxia of speech, which may have influenced the results of comparisons between PSP and PNFA groups. Ideally, a systematic neuropsychological study of PSP patients recruited from movement disorders clinics is needed to determine the true frequency of linguistic deficits in patients who present primarily with movement disorder, with a population based approach to examine the issue more generally. Nonetheless, the vast majority of PSP patients included in the present study had typical motor features of the disorder by the time of their initial assessment in our clinic, and all met diagnostic criteria, which emphasize the presence of typical motor features. Furthermore, pathological confirmation was available in about 20% of patients; all pathologically confirmed cases had evidence of 4-repeat tau pathology (three with PSP pathology and one with corticobasal degeneration). One strength of our study was the consistent use of predefined clinical assessment tools, designed to probe pertinent symptoms and signs used to distinguish potential PSP cases from PNFA cases; however, not all aspects of language were assessed. Specifically, some previous PSP studies have reported disproportionate impairment of verbs compared to nouns [15, 42], but the SYDBAT used here only includesnouns.
Speech and language disturbances have been recognized in PSP for several decades, but the overlap with PNFA has only been appreciated more recently. Dysarthria and adynamism are accepted as common features [43], but the question of true aphasia has been more controversial. Nonetheless, non-fluent language production in PSP with deficits in object naming were reported as early as the late 1970 s [44]. More recent studies have confirmed deficits of picture naming and word-to-picture matching and, as mentioned, disproportionate difficulty on verbs rather than nouns [14, 42], linked to pathology of the inferior frontal gyrus [15]. Syntactic comprehension disturbances have been reported in PSP less frequently [23, 45], but not consistently [46], and no direct comparison to PNFA has been attempted previously. Unfortunately, most studies examining PNFA and PSP have not teased apart the signs and symptoms of aphasia from those of primary progressive apraxia of speech, complicating interpretation of the findings. When cases of primary progressive apraxia of speech, who have little or no aphasic features, were specifically selected, a close relationship with tau pathology and particularly PSP was identified [23, 48]. In the present study, patients with primary progressive apraxia of speech were excluded. As such, the rates and severity of aphasic deficits may have been even higher than in previous studies. Nonetheless, on all measures apart from single word repetition, PSP patients demonstrated aphasic deficits that were as frequent and severe as seen in PNFA.
A separate, but related issue is whether PNFA patients who develop motor features of PSP later in the course of their illness differ from other PNFA patients. One detailed study compared 4 patients who presented with PNFA, with later development of PSP features (referred to as PSP-PNFA), to other PNFA cases [17]. Although both patient groups fulfilled the Neary criteria for the diagnosis of PNFA at presentation, the pattern and severity of aphasia differed. Patients with PSP-PNFA tended to have a reduced overall speech rate, measured in words/minute on a spontaneous language task. Spelling was significantly more impaired in the PNFA group compared to the PSP-PNFA group, but no significant group differences were established on tests of comprehension, repetition, or reading [17].
The clinical and pathological overlaps between PSP and PNFA have been increasingly recognized. Consistent with previous reports [26, 43], two of the PSP patients in the current study initially presented with PNFA. Although none of the PNFA patients included in the present study had pathological diagnoses, PSP pathology has been described in otherwise typical cases of PNFA [20, 49]. The pathology of PNFA is heterogeneous, with cases caused by forms of tauopathy, TDP-43 pathology, and Alzheimer’s disease; more specific biomarkers of underlying pathologies are needed, especially as targeted molecular therapies are developed [50–52]. As such, development of a reliable biomarker of PSP pathology for use in PNFA and unclassifiable cases of non-fluent aphasia would represent a major advance.
Adynamic speech may be the most distinctive language symptom and sign in PSP, and should be examined as a potential clinical biomarker of PSP pathology. In the present study, 92.9% of patients reported adynamic speech, which we defined historically as reduced verbal content or spontaneity, consistent with previous studies that have emphasized adynamic speech in PSP [5, 9–11]. The neurolinguistic processes underpinning adynamic speech remain relatively under investigated, although detailed case reports have been published by Warren et al. [13] and Robinson et al. [9, 10] suggesting that deficits in generation of novel thoughts and/or verbal messages may be responsible.
Separately, reduced cognitive processing speed is considered a hallmark of PSP [53, 54] and other sub-cortical dementias [7, 55]. Typically, neuropsychological tests of language are not timed, and performance is judged according to the accuracy of a response, rather than according to speed of response. Unlike tests of language, the executive tasks used in the present study were timed, and demonstrated marked cognitive slowing in PSP patients. However, the Trail making test and the RCF copy task are, to a variable extent, dependent on motor responses, and therefore could be confounded by significant parkinsonism.
Executive dysfunction has long been recognized as a core feature of PSP [8, 55], but the relationships between cognitive slowing, executive dysfunction, adynamic speech, and aphasia remain controversial. In the present study, there was no significant correlation between performance on the SYDBAT subtests and performance on executive or working memory tasks, suggesting that poor performance on language tasks was not solely due to executive dysfunction, but rather reflects a true aphasia in PSP.
The present study suggests that aphasic deficits occur in PSP, at a similar severity to those seen in PNFA. These findings are in keeping with emerging concepts of clinical and pathological overlaps between PSP and PNFA, and argue against a pure adynamic aphasia in PSP. Nonetheless, further study of aphasia across the several different phenotypes of PSP, with neuropathological confirmation of PSP pathology, are needed to determine the true frequency of aphasia across the range of PSP phenotypes. Conversely, the presence of cognitive slowing may prove to be an important clinical biomarker of underlying PSP pathology in patients who present with PNFA or unclassifiable non-fluent aphasia. Future studies might utilize analysis of picture descriptions, or endogenously generated speech, to determine the utility of quantifying adynamism [9, 10]. Vocal analysis, looking at measures of pause frequency [56] and response latency may also be helpful. Regardless of the approach, measures of adynamism should be developed and studied as potential clinical biomarkers of PSP pathology.
Footnotes
ACKNOWLEDGMENTS
This work was supported by funding to Forefront, a collaborative research group dedicated to the study of frontotemporal dementia and motor neuron disease, from the National Health and Medical Research Council of Australia (NHMRC) program grant (#1037746) and the Australian Research Council Centre of Excellence in Cognition and its Disorders Memory Node (#CE110001021). Autopsy collection through the Sydney Brain Bank was supported by the University of New South Wales and Neuroscience Research Australia. We are grateful to the research participants involved with the ForeFront research studies and wish to thank the staff of the Sydney Brain Bank for tissue preparation and characterization of the Sydney cases. In addition, JRB is supported by a NHMRC Early Career Fellowship (#1072451), KJB by an ARC Future Fellowship (FT120100355) and GMH is supported by a NHMRC Senior Principal Research Fellow (#1079679).