
Abstract
Background:
Dilated perivascular spaces in the centrum semiovale (CSO-PVS) are closely related to small vessel disease. However, recent studies have revealed that cerebral amyloid angiopathy can cause dilation of the CSO-PVS and obstruction of interstitial fluid flow along the intramural periarterial drainage.
Objective:
To examine the severity and age-related prevalence of CSO-PVS through magnetic resonance imaging (MRI) and investigate their clinically relevant factors.
Methods:
This study included 1,060 subjects who participated in our brain program. The subjects ranged from 23 to 83 years in age and were active in society. The frequencies of the MRI abnormalities of small vessel diseases, including CSO-PVS, were examined. The CSO-PVS severity was classified into three grades: G0, G1, G2, according to the visual rating. The subjects were divided into five age groups and their age-related frequencies were also studied. Using the clinico-laboratory data of 712 subjects, the clinically relevant factors of CSO-PVS were investigated using logistic regression analysis.
Results:
The frequencies of all G0 (“normal”) MRI abnormalities significantly decreased with age. A high prevalence of G2 CSO-PVS was observed (24%) in the youngest group aged≤39 years, whereas other MRI abnormalities in this group were not or rarely observed. In multivariable logistic regression analyses, G2 CSO-PVS was found to be closely associated with age, hypertension, and the estimated glomerular filtration ratio.
Conclusions:
This study reveals that CSO-PVS begin to develop in subjects aged less than 39 years. Age-related changes are involved. Further studies are necessary to elucidate the pathophysiological role of the CSO-PVS.
Keywords
INTRODUCTION
Recently, perivascular spaces (PVS) have become a topic of interest in research on the communication pathways of interstitial fluid (ISF) from the brain to the cervical lymph nodes. Amyloid-β (Aβ), one type of brain waste, is eliminated from the brain along the periarterial pathway [1]. Aβ deposition in the brain is a well-known phenomenon of normal aging and is a hallmark of Alzheimer’s disease (AD). In cerebral amyloid angiopathy (CAA), Aβ is deposited in basement membranes in the walls of the cortical and leptomenigeal arteries. Recent patho-clinical studies have suggested that CAA can cause dilatation of PVS in the centrum semiovale (CSO-PVS or SPVS) through blockage of ISF flow along intramural periarterial drainage pathways [1, 2]. Further, severe CSO-PVS are more frequent in patients with pathology-proven CAA and can be regarded as a surrogate marker for CAA [3].
CSO-PVS are well-known as a MRI marker of small vessel disease [4]. However, most studies relevant to CSO-PVS have targeted elderly subjects [4]. The frequency of CSO-PVS in young or middle-aged subjects has not been investigated thoroughly.
If dilated CSO-PVS can develop secondary to obstruction due to the deposition of amyloid or other contents of ISF in the cortical or leptomeningeal arteries, MRI would detect dilated CSO-PVS in non-demented younger subjects, thereby providing more information on the development of CAA and AD, as well as small vessel disease. In this study, we investigated the prevalence of dilated CSO-PVS on MRI in socially active subjects in a wide range of age groups to clarify the pathophysiological role of CSO-PVS in the brain.
METHODS
Standard protocol approval
This study was performed with approval of the Institutional Review Board of Otowa Hospital. Written informed consent was obtained from all subjects.
Study population and data collection
For this cross-sectional analysis, we used prospectively collected data from the brain program in the Health Screening Center at Otowa hospital for 24 months, beginning in March 2015. This program consisted of physical examinations and non-invasive brain MRI studies with or without blood chemistry for the prevention and early detection of brain disorders. Most subjects were middle-aged and socially active, and showed no signs of cognitive impairment. Elderly subjects were also socially active and independent in their daily lives. A history of minor cerebrovascular disease was noted in 19 subjects. These subjects were excluded from the study: the data of 1,060 subjects were thus used for the analyses of the severity and age-related frequencies of six MRI abnormalities. A 3- or a 1.5-Tesla (T) MRI was used for the brain screening. Thus, we focused on the frequencies of CSO-PVS in socially active middle-aged and elderly subjects by 3T or 1.5T MRI.
Of the 1,060 subjects who underwent MRI, laboratory data were not obtained for 348 subjects. A majority of those subjects were professional truckers; they were relatively young and predominantly male. Thus, a subset of 712 subjects was created. For this subset, the clinical history and laboratory examinations, as well as MRI, were available. Age, body mass index (BMI), estimated glomerular filtration rate (eGFR), smoking, hypertension (HT), dyslipidemia (DL), and diabetes mellitus (DM) were the variables in this study. Subjects undergoing drug treatment for any of the conditions listed above were regarded as positive for that variable. Smoking was defined as being currently a smoker or having a history of smoking. The cutoff levels for age and BMI were 50 years and 30, respectively. The other cutoff levels were based on the criteria described in a previous publication [5]. Briefly, the cutoff levels for eGFR and HT were 60 ml/min/1.73 m2 and 140/90 mmHg, respectively. The cutoff levels for DL were low density lipoprotein cholesterol≥140 mg/dL, high density lipoprotein cholesterol <40 mg/dL, or triglycerides≥150 mg/dL. The cutoff level for DM was 6.5% in hemoglobin A1c.
MRI data acquisition and analysis
The brain MRI protocol of both 3T and 1.5T MRIs included T1- and T2-weighted images, fluid-attenuated inversion recovery (FLAIR) images and T2 star weighted images and MR angiography. In this study, the T2-weighted images, FLAIR images and T2-star images were assessed. On the 1.5T MRI scanner (MAGNETOM Avanto, Siemens, Erlangen, Germany), the T2-weighted image sequence was as follows: repetition time (TR) = 5850 ms, echo time (TE) = 95 ms, flip angle = 180 degrees, voxel size =0.6×0.5×5.0 mm3. FLAIR image sequence was as follows: TR = 900 ms, TE = 105 ms, flip angle = 170 degrees, voxel size = 0.9×0.7×5.0 mm3. T2-star-weighted images had the following specifications; TR = 650 ms, TE = 21.9 ms, flip angle = 20 degrees, voxel size = 1.3×0.9×5.0 mm3.
On the 3T MRI scanner (MAGNETOM Skyra, Siemens, Erlangen, Germany), the T2-weighted image sequence was as follows: TR = 5000 ms, TE = 87 ms, flip angle = 150 degrees, voxel size = 0.4× 0.4×5.0 mm3. The FLAIR image sequence was as follows: TR = 10000 ms, TE = 90 ms, TI = 25640 ms, concatenations = 2, flip angle = 150 degrees, voxel size = 0.6×0.6×5.0 mm3. T2-star-weighted images had the following specifications; TR =545 ms, TE = 10 ms, flip angle = 20 degrees, voxel size = 0.7×0.7×5.0 mm3.
The CSO-PVS and the perivascular spaces in the basal ganglia (BG-PVS) were defined as linear when imaged parallel to the course of the vessel, and round or ovoid, when imaged perpendicular to the course of the penetrating vessels [6]. Visual ratings for the CSO-PVS and the BG-PVS on T2-weighted images were done into three grades: G0 = none or few abnormalities, G1 = moderate, and G2 = abundant (Fig. 1), with reference to our previous quantitative assessment using 3T MRI with CISS [7], in which they were classified as follows (per cerebral hemisphere): <10 for the “few” group, 11–30 for the “moderate” group, and >31 for the “abundant” group.

Grading of CSO-PVS on MRI. CSO-PVS were classified into three grades; G0 = none or few, G1 = moderate, and G2 = abundant. CSO-PVS were visible as linear structures in the white matter of the centrum semiovale (white arrows). Abundant CSO-PVS were noted in patients classified as G2, among which the juxtacortical CSO-PVS (dark arrows) were thicker than those in the deep white matter.
Although the images on 3T MRI had higher resolution, the images on 1.5T MRI could show clear delineations of all MRI abnormalities with appropriate settings of window level and width. To observe CSO-PVS, we set a window level of 450 and a width of 250 for 3T MRI and of 300 and 200 for 1.5T MRI, and combined both data sets for analysis (Supplementary Figure 1). Cohens’ kappa values for the inter-rater agreement were 0.81 for SPVS and 0.83 for BPVS, respectively. CSO-PVS could be seen within the white matter in any location, but they were more often observed in the parieto-occipital region near the trigone of the lateral ventricle. CSO-PVS in the juxtracortical white matter tended to be thicker (Fig. 1).
Periventricular hyperintensities (PVH) and deep white matter hyperintensities (DWMH) were assessed with T2-weighted images. They were classified into four grades (G0 to G3) according to the Fazekas scale [8]. T2-star images were used to assess MBL quantitatively, which were classified into three grades; G0 = none, G1 = one lesion, G2 =two or more lesions. Brain atrophy was assessed by measuring frontal subarachnoid-space widening (FSSW) over 3 cm on T2-weighted MR images [9]: G0 = less than 3 cm, G1 = 3 cm or more.
Multivariable logistic regression analysis was used to evaluate the association between the high grades of CSO-PVS and the independent variables in the 712 subjects for whom both MRI and clinico-laboratory data were available.
Statistics
Continuous data are provided as the mean and standard deviation, and categorical data are provided as the prevalence and percentage. Comparisons of the means between two groups were calculated using Welch’s 2-tailed t-test. Comparisons of the categorical data were performed using the chi-squared tests. The inter-rater agreement was examined with Cohens’ kappa coefficient. To assess age-related changes, subjects were divided into five age groups by age:≤39, 40–49, 50–59, 60–69, and≥70. Subjects under 39 or over 70 years of age were regarded as a single age group because of the low numbers of subjects of those ages. A decreasing trend in prevalence of Grade 0 of the respective variables among age groups was examined using the Cochran–Armitage test.
To assess the association with CSO-PVS, a subset of the data for which clinico-laboratory and MRI data were available, containing 712 of the 1060 subjects was analyzed. Since CSO-PVS was divided into three grades, we compared the G0 data as a reference with the G1 data and G2 data. To assess the effect of modification and interaction among the potential risk factors, multivariable analyses were conducted after adjustment for pre-specified age, BMI, eGFR, smoking, HT, DM and DL. Significance was set at p < 0.05. All statistical analyses were performed using the open source software R Foundation (version 3.3.1; R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org).
RESULTS
A summary of the 1,060 subjects who underwent MRI analyses is shown in Table 1. The mean age and SD were 54.2 and 10.2 years, ranging from 23 to 83 years. Of all subjects, 76.6% were male. A summary of the clinico-laboratory analyses of the subset of 712 subjects is also shown in Table 1. As data for 348 subjects were excluded, this subset showed a higher mean age (p < 0.05) and a lower rate of male preponderance (p < 0.05). However, there were no significant differences in any MRI abnormalities between the data groups.
Characteristics of data for MRI analysis and logistic regression analyses. MRI data were obtained for 1060 subjects. Data for logistic regression analyses were available for 712 subjects, because 348 relatively young, male subjects did not undergo laboratory examinations. However, there were no statistical differences regarding MRI abnormalities between both groups
Regarding the severity-related frequencies, the G0 classification of all MRI abnormalities, except CSO-PVS, was most common (Fig. 2). In contrast, the G0 classification of CSO-PVS was least common and increasing frequency with increasing severity was observed.
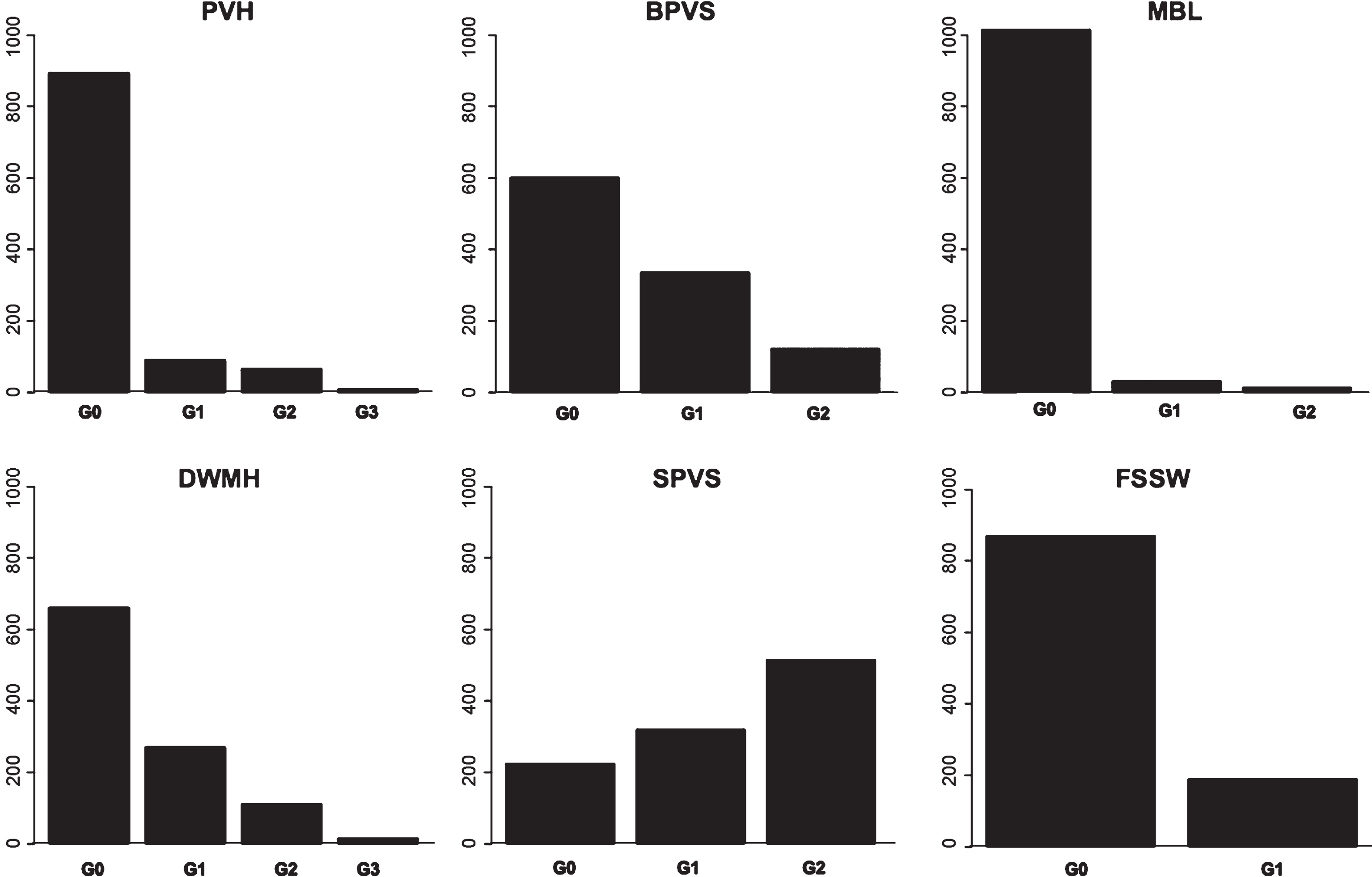
Frequencies at each grade of the six MRI abnormalities of PVH, DWMH, BG-PVS, CSO-PVS, MBL, and FSSW. In all except CSO-PVS, the lowest grade (G0) occurred most often. In contrast, G2 occurred most often, followed by G1, in CSO-PVS.
We then examined age-related frequencies. Subjects were divided into five groups; ≤39, 40–49, 50–59, 60–69 and≥70. The numbers of subjects in these groups were 69, 247, 448, 219 and 77, respectively. Figure 3 shows percentage of each grade in each age group. The Cochran-Armitage trend test for G0 revealed a decreasing trend with age for all variables (p < 0.001). G2 of CSO-PVS was found in 24.6% of subjects in the youngest group, increasing to 55% if G1 (30.4%) was included. Thus, there was a high frequency of high grades of CSO-PVS even in the≤39 age group. This finding was markedly different from the results of the other MRI abnormalities.

Age-related percentage of frequencies at each grade of the six MRI abnormalities PVH, DWMH, BG-PVS, CSO-PVS, MBL, and FSSW. Subjects were divided into five age groups; ≤39, 40–49, 50–59, 60–69 and≥70. The incidence of G0 of all MRI abnormalities (i.e., “normal”) gradually decreased with age. As a peculiar finding, G2 of CSO-PVS was observed in 24.6% of all subjects in the group under 39 years of age: G0 or G1 was observed in 55% of all subjects.
Multivariable logistic regression analysis of G1 CSO-PVS to G0 as a reference was not statistically different for any variables (Table 2). In contrast, G2 CSO-PVS showed statistically significant differences for three variables: age, eGFR, and HT (Table 2). The highest multivariable odds ratio, 2.53, was found for eGFR (95% confidence interval: 1.03 – 6.20). Thus, in subjects over 50 years of age, low eGFR of <60 ml/min/1.73 m2, and hypertension were regarded as facilitating factors for CSO-PVS.
Odds ratios for SPVS. Odds ratios were computed using binary logistic regression analyses for G0 SPVS as a reference and compared with G1 or G2 of SPVS. There were no statistical differences among variables in G1 SPVS. In contrast, G2 SPVS showed statistically significant differences in three variables; age, eGFR, and HT
DISCUSSION
The present study revealed that the G0 (“normal”) classification of all MRI abnormalities showed a significant decrease in prevalence with increasing age. In contrast, higher grades of abnormalities detected on MRI gradually increased in prevalence above at 40 or 50 years of age. Among these, a unique finding was observed for CSO-PVS, where the highest grade (G2) was observed in 24% of subjects of the youngest age group. In multivariable logistic regression analyses, significant associations between the highest grade of CSO-PVS and age, hypertension, and eGFR were noted.
In a previous study, we used the term “Virchow-Robin spaces” (VRS), which is equivalent to an observation of PVS on MRI [7]. Using 3T-MRI and a highly fluid-sensitive method of constructive interference in the steady state, we showed the morphological differences in the VRS between the centrum semiovale and basal ganglia, and a decrease in the prevalence of VRS in the centrum semiovale in patients with idiopathic normal pressure hydrocephalus. Although VRS are considered to be physically empty spaces, a recent ultrastructural study showed that there is no empty space between the artery wall and the glia limitans [10]. Furthermore, STRIVE recommends the term “perivascular space” [6]. We therefore have used the term “PVS” instead of “VRS” in this manuscript.
The white matter abnormalities on MRI such as PVH or DWMH usually begin to develop from around 40 or 50 years of age and then gradually increase in prevalence with age [7–11]. In this study, the higher grades of CSO-PVS (G1 and G2) were already observed in more than half of all subjects in the youngest age group under 40. This observation of the high prevalence of high grades of CSO-PVS in young and middle-aged subjects corresponds well to the data of patients with traumatic brain injury using T2-weighted images on a 1.5T MRI, where the number of CSO-PVS was associated with age in their control group of 17 subjects ranging from 18 to 47 years of age [12]. Although this study included only a small number of subjects, the results showed that CSO-PVS could be observed even in young subjects, and that SPVS increased in prevalence with age. Thus, CSO-PVS can develop in middle age or earlier.
Dilated CSO-PVS are regarded as a feature of cerebral small vessel disease [4]. A population-based study of CSO-PVS in the elderly subjects reported that the degree of CSO-PVS is associated with age, hypertension, volume of white matter hyperintensities, and lacunar infarction [13]. The present study also reveals that age, hypertension, and eGFR are factors of CSO-PVS even in subjects of a wider range (23 to 83 years) with socially active life. This suggests that CSO-PVS is a marker of age-related hypertensive processes.
High grades of CSO-PVS are also noted in patients with pathology-proven CAA and they are more frequent than those in the control subjects [3]. Another study shows that the prevalence of high grades of CSO-PVS is greater in CAA-related intracerebral hemorrhage than in hypertensive arteriopathy-related intracerebral hemorrhage [14]. A patho-neuroimaging study revealed that dilation of the perivascular spaces and drainage failure of the ISF from the white matter in AD may be associated with the deposition of Aβ in the perivascular fluid drainage pathways of the cortical and leptomeningeal arteries [2]. The perivascular drainage of fluid and solutes from the white matter seems to be impaired by CAA in the parent leptomeningeal or cortical arteries with consequent dilatation of PVS in the white matter [1]. These studies indicate that dilated CSO-PVS, which can be visible on MRI, can also be a surrogate marker for CAA [4].
A recent study revealed that CSO-PVS were associated with clinically-diagnosed AD but failed to show any association with amyloid PET positivity [15]. This may be because of the low resolution of PET or they might be manifestations of an amyloid-independent process. Although a high frequency of co-occurrence was observed between CAA and AD, CAA was absent in subjects with frequent neuritic plaques but present in 20.9% of subjects with no neuritic plaques [16]. Thus, the dilated CSO-PVS could be a marker for CAA, but also could be a marker for other common disorders such as cerebral small vessel disease. Since marked difference is noted between CSO-PVS and other MRI abnormalities of small vessel disease, dilated CSO-PVS are more plausible for a marker of deposition in PVS with amyloid or other contents in ISF. Hypertension would play an important role in the blockage of ISF drainage along the leptomeningeal or cortical arteries. Further studies are necessary to elucidate the relationship between impaired drainage of brain waste and hypertension.
The present study is the first to report that impaired renal function has a high association with the highest grade of CSO-PVS, a possible marker of CAA, as well as small vessel disease. Chronic kidney disease is known as a major burden on global health and is also associated with cerebral vascular diseases [17]. Impairments of ISF drainage and of glomerular filtration may correspond, as the brain and kidneys share the specific feature of continuous high-volume perfusion and the traditional risk factors for vascular injury including hypertension [18].
The strength of this study is that it represents a recent, non-invasive assessment of more than 1,000 subjects over 24 months. The brain program at our hospital is a health screening program for actively working subjects. It includes a minimum of MRI, MR angiography, laboratory examinations, and medical advice for the prevention and early detection of stroke as well as cognitive and other neurological disorders. In this study, a majority of the subjects were middle-aged and socially active, and showed no signs of cognitive impairment. Therefore, this study provides important data concerning the preclinical stages of vascular and neurodegenerative diseases. However, there were several limitations. There was a selection bias. The subjects in this study were health-conscious and paid the examination fee themselves, so they may not reflect the general population. Another limitation is the lack of data on cognitive performance. As our brain program is not part of a specialized “dementia clinic”, we did not assess the cognitive state of the participants. However, as stated above, the subjects in this program are socially active and have no evident cognition impairment.
The present study revealed that high grades of CSO-PVS are already developed in middle age, when subjects are socially active and show no signs of dementia. The highest grade of CSO-PVS shows associations with age, hypertension, and low eGFR.
Further studies are necessary to clarify whether dilated CSO-PVS are truly caused by hypertension, how dilated CSO-PVS in middle age can lead to deleterious effects on the brain over long time intervals, and how much dilated CSO-PVS may contribute to the development of cognitive impairment.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank staff at the Health Screening Center and the Outpatient clinic at Otowa Hospital. Author MI receives honoraria for lecturing from Johnson and Johnson Japan, Medtronic Japan, and Nihon-Mediphysics Japan. Author SY receives honoraria for lecturing from Codman and Johnson and Johnson. Author KY has no competing interests.
This study was supported by Health and Labor Sciences Research Grants for Research on Intractable Diseases, Ministry of Health, Labor and Welfare, Japan (2014-Nanci-General-052). The sponsors were not involved in the study design, collection, analysis, or interpretation of the data, writing of the report, or in the decision to submit the paper for publication.