
Abstract
Background:
Saccadic paradigms display changes across a number of degenerative conditions reflecting changes in the oculomotor pathway which in some conditions have been linked to disease presentation.
Objective:
To examine a novel range of saccadic paradigms in behavioral variant frontotemporal dementia (bvFTD).
Methods:
Prosaccade, predictive, self-paced, memory-guided, and anti-saccade tasks were examined in bvFTD patients and controls.
Results:
A significant increase in latency for the bvFTD group was seen in all tasks. Self-paced saccades are reduced in number, memory-guided saccades display an increase in errors. Predictive saccades show an increased latency that does not remain when prosaccade latency changes are accounted for. While changes were seen across a range of paradigms, no individual task completely separated bvFTD from control participants.
Conclusion:
bvFTD patients as a group display a number of changes on saccadic testing which may reflect the frontal lobe changes seen in this condition.
Keywords
INTRODUCTION
Saccadic performance has become of increasing interest in clinical research into neurological disorders, with findings of significant changes in prosaccades and anti-saccades in Huntington’s disease [1], and anti-saccades in Alzheimer’s disease (AD) [2]. Changes in saccade parameters have been correlated with neuropsychological performance, with saccadic paradigms used to index executive functioning in different groups including schizophrenia patients, the elderly, and children [3, 4]. Executive functioning is controlled through the frontal cortex and consists of a number of different domains including working memory, attention, inhibitory control, judgement, and planning. Different saccadic paradigms, whose anatomical substrates overlap with executive control centers, have been used to index some of these different domains of cognitive function.
Higher-order saccades include anti-saccades, self-paced, predictive, and memory-guided saccades. Higher-order saccades recruit different cortical areas to modulate eye movements depending on the task, including pathways through the frontal lobe. These saccades require a range of different processes beyond a simple reflexive response for their triggering. Behavioral variant frontotemporal dementia (bvFTD) is an insidious, largely younger-onset neurodegenerative disease which presents with changes to behavior, mood, and personality. Behavioral changes can be classified as either apathetic or disinhibited, and may include a loss of empathy, disinterest, social inappropriateness, withdrawal, or impulsivity [5, 6]. The disease results in atrophy of the frontotemporal limbic/paralimbic circuit, particularly in the ventromedial prefrontal cortex, orbitofrontal cortex, anterior insula, anterior cingulate, anterior temporal lobe, and the ventral striatum [7 –9]. BvFTD is one of the three variants of frontotemporal dementia and sits on a spectrum with motor neuron disease (MND), progressive supranuclear palsy (PSP), and corticobasal syndrome [10]. These diseases overlap with bvFTD both on a molecular level and behaviorally [11], and it is not uncommon to be diagnosed with bvFTD along with MND (FTD-MND) or bvFTD with parkinsonism. Cases can also be classified according to the nature of the accumulated protein, including tau, TDP-43, or FUS proteins [12]. This classification is important, as therapeutic options are beginning to target the underlying molecular pathophysiology. In bvFTD, the molecular classification cannot be determined from the phenotypic presentation.
Clinical changes can appear subtle in the early stages of the disease, and fifty percent of patients are given a psychiatric diagnosis before their diagnosis of bvFTD [13]. Diagnosis is usually made via a combination of clinical features and supportive investigations, as there is no one pathognomonic sign [14].
The regions in the cortex involved in saccade control overlap with the areas reported to degenerate in bvFTD, thus further understanding of how bvFTD patients perform on tests of saccadic function may yield clinically useful markers of illness progression, and/or response to future disease-modifying treatments.
Lesions to the frontal eye fields have shown an increased latency in prosaccades, memory-guided, and anti-saccades, as well as a reduction in the number of predictive saccades made [15]. The atrophy seen in bvFTD includes the frontal eye fields, thus an increased latency for a range of saccadic paradigms may be predicted in this group. Alternatively, a decreased latency may be seen in bvFTD patients in those movements with higher cortical input due to a lack of inhibition from the dorsal lateral prefrontal cortex (DLPFC) [16]. It could be anticipated that velocity of eye movements would be slightly reduced due to frontal eye field degeneration [17], but not to the degree expected if the brainstem regions were involved, such as the changes seen in PSP [18].
Current literature does not provide a clear indication of what occurs in bvFTD regarding latency and velocity. Examining patients identified by phenotypical presentation, Meyniel et al. [19] found an increase in horizontal prosaccade latency in bvFTD patients compared to controls, whereas studies by Boxer et al. [20] and Garbutt et al. [21] failed to show a significant difference. Boxer et al. [22] however examined eye movements based on identifying patient participants’ underlying molecular pathology at autopsy and reported reduced velocity and gain only in participants with tau-pathology, with TDP43-pathology participants not performing significantly different from controls. The significant change in velocity in vertical prosaccades reported by Moon et al. [23] in FTD-MND patients appears to be in contrast to these results, as FTD-MND patients predominantly have TDP43 accumulation (Type B) as their underlying pathology. This should predict that prosaccades will be indistinguishable from those of normal subjects in participants with FTD-MND. However, this is not what has been reported by Moon et al. [23], who found significant changes in velocity. An isolated report of a single bvFTD patient with TDP43 pathology demonstrated oculomotor changes, including a partial vertical gaze palsy and “square wave horizontal saccades” [24]. Thus, it is not possible to anticipate ocular-motor performance in these patient groups on the basis of the protein aggregate alone. The eye movement changes reported in the FTD-MND population by Moon et al. [23] may be able to be explained by the MND component; however, motor neuron disease has traditionally been thought to spare saccadic eye movements [25]. These results may also be able to be explained by slightly different cortical degeneration within the different TDP-43 subtypes, rather than just the molecular aggregate type alone.
A number of studies have examined anti-saccades in bvFTD, and a few studies have compared this higher order saccade task in bvFTD and AD. BvFTD patients and AD patients appear to make similar numbers of anti-saccade errors [21] and both conditions appear significantly different to controls [19–22 , 26]. This is not surprising, given their difficulty with inhibitory control at a behavioral level. AD patients show a low rate of corrections; however, bvFTD participants have been reported to correct as well as controls [21]. This is thought to reflect bvFTD participants’ more intact visual processing, as including corrections produced a higher correlation with neuropsychological tests with greater visual components [20].
Anti-saccades worsen with disease progression in AD and provide a reliable eye movement correlation for disease severity [27]. Anti-saccade correct responses and corrected errors have been positively linked with Mini-Mental State Exam (MMSE) scores [20, 28] and have been suggested as a possible biomarker in AD [29]. Unlike in AD, MMSE scores in bvFTD are not correlated with anti-saccade performance [20], although this may be due to MMSE underestimating impairment in bvFTD, as it is relatively insensitive to impaired executive functioning [30]. No data is available for how bvFTD patients’ anti-saccades change over time. Anti-saccade errors are negatively correlated with tests of frontal lobe function, including the Frontal Assessment Battery (FAB) and Mattis dementia rating scale in bvFTD patients [19], as these tests are more sensitive to the deficits occurring in bvFTD [31, 32]. While the literature has examined prosaccades and anti-saccades in these patients, higher order saccades also extend to self-paced saccades, predictive saccades, and memory-guided saccades. Similar to anti-saccades, these volitional saccade paradigms have the potential to be sensitive to changes in bvFTD as their pathways overlap with areas known to degenerate in this disease, yet these paradigms have not been explored in the literature. Eye movement recording produces objective results, and simple paradigms such as self-paced saccades and predictive saccades may have utility in examining those in whom cognitive testing is difficult. This study sought to examine the changes displayed by bvFTD participants in an exploratory manner relative to controls in these higher-order saccadic paradigms. Prosaccades and anti-saccades, which have been previously examined, were included for reference, and we sought to index bvFTD behavior on self-paced saccades, predictive saccades, and memory-guided saccadic paradigms.
METHOD
This study received ethical approval as part of a larger study from the Melbourne Health Human Research Ethics committee (HREC #2013.015). All participants and/or their responsible person were involved in the discussion and consent process of the study. One patient participant was deemed unfit cognitively to consent for themselves and so consent was provided after discussion with both the patient and their responsible person as approved in the ethics application. All other participants gave their own consent.
Participant information
Patient participants were recruited from the Royal Melbourne Hospital Neuropsychiatry unit (NPU) and controls from the university newsletter or partners of patient participants. Diagnosis was made based on clinical criteria [33] by a multidisciplinary team including psychiatry, neurology, psychology, and occupational therapy. All patient participants had received an MRI, fMRI, or both as part of their normal diagnostic work-up on the ward and met Rascovsky et al.’s criteria [33] for probable bvFTD. Exclusion criteria for all participants included any history of another neurological condition: co-morbid major depressive disorder, bipolar disorder, or schizophrenia; stroke, intracranial mass on MRI, traumatic brain injury, alcohol and/or substance abuse, significant intercurrent medical illness, learning disorder, and significant ocular pathology.
Materials and tasks
Participants were seated 67 cm in front of a Samsung SyncMaster 2043 monitor. Gaze was tracked using an SMI HEDx tracker (200 Hz) mounted on a bicycle helmet [34].
Horizontal and vertical prosaccades, self-paced, predictive, memory-guided, and anti-saccades were tested. A five-point calibration was run before each saccade task. The target for all paradigms was a 0.9 degree dot.
Prosaccades were examined by moving the target pseudo-randomly every 1200 to 2100 ms between center, 5, 10, and 15 degrees horizontally, and center, 5, and 10 degrees vertically. Thus, while the saccade jumps were determined randomly, each participant received exactly the same stimuli. There were 80 horizontal prosaccade trials and 88 vertical prosaccade trials.
Predictive saccades were tested immediately after the prosaccades so that participants continued with the instruction of “follow the target” to minimize mental load and learning demands on this cognitively impaired patient group. The target alternated 10 degrees left and right every 1000 ms for 1 minute (60 trials).
The self-paced saccade paradigm presented two targets 20 degrees apart for 1 minute, while participants were instructed to alternate their gaze as quickly as possible between the two. Anti-saccade trials displayed a black target in the center of the screen for the entire task. This was done to give a consistent point to return to. A red target was displayed after a pseudo-random fixation time (1000 ms to 1900 ms) at either 5 or 10 degrees to the left or right of the central dot. Participants were instructed to “Look at the central black dot, another dot (red) will be flashed either to the left or right, when this happens don’t look at the red dot; instead look in the opposite direction, to where the mirror image of the dot would be (look an equal and opposite amount). A green dot will flash in the correct location after a short period of time. Once the green dot has flashed return your gaze to the central dot”. 2000 ms was given to make an eye movement in the opposite direction before a green dot was displayed for 600 ms showing the correct eye movement location.
Memory-guided saccade trials displayed a central black target and after a pseudo-random fixation time (800 ms to 1800 ms) a target was presented at 5 or 10 degrees to the right or left for 150 ms. Shorter times were trialed but in pilot testing this resulted in the image remaining frozen on the screen. After a further pseudo-random fixation time (800 ms to 2000 ms) the central target was extinguished, and participants were given 2000 ms to move their eyes to where they remembered the target being before a green target flashed in the correct location. Participants were instructed to “Look at the central black dot, another dot will flash in the surrounding area; do not look at it. Once the central dot goes out, move your eyes to where the dot flashed.” For both memory-guided and anti-saccades, two practice trials with extra instruction from the examiner, to ensure they understood the task, were undertaken. These two trials could be repeated once if required. Practice trials were not given for any other paradigm. After the practice trials, 48 anti-saccade trials and 40 memory-guided trials were presented.
In addition to the diagnosis, the Neuropsychiatry Cognitive Screening tool (NUCOG) scores, as performed at the hospital visit closest to eye movement testing, were collected for each patient participant. The NUCOG is a validated cognitive screening tool which assesses performance in the following domains: executive function, memory, visuo-spatial construction, attention, and language [35]. Total score (out of 100), and individual cognitive domain scores (out of 20) are reported in Table 1.
BvFTD patient participant age and cognitive scores. Abnormal scores have been asterisked
Data analysis
A velocity threshold of 30 degrees/sec and an acceleration of 8000 degrees/sec2 was used to define when a movement began and ended. Not all trials resulted in an analyzable movement. All paradigms except self-paced saccades were analyzed for latency. Horizontal and vertical prosaccades were additionally analyzed for asymptotic peak velocity and gain. Asymptotic peak velocity was analyzed by fitting a one-phase exponential decay non-linear regression line to the magnitude and peak velocity for each saccade data set from all of the trials per participant. The plateau of the fit for all trials was taken as the asymptotic peak velocity for each participant. Participants were removed if their data did not result in a reliable fit.
Predictive saccades were analyzed without excluding anticipatory saccades. Latencies for each participant had their corresponding prosaccade latency subtracted to determine average prediction.
Self-paced saccades were analyzed for the highest number of saccades able to be generated in any 30-s window in the testing. This value was determined rather than taking the total number of saccades made in the one-minute window of testing as it was observed that participants’ attention wandered easily, and this gave a more consistent indication of their best performance.
Memory-guided and anti-saccade analysis examined the number of errors, corrections, and latency of correct movements. Latency values had the corresponding prosaccade latencies subtracted. A correct anti-saccade was recorded if the first movement after the appearance of the target was in the opposite direction to the red target. Anti-saccade errors were defined as movement in the incorrect direction after the appearance of the red target. Total errors were expressed as a proportion of total number of analyzable trials. Corrected errors were explored as a proportion of the total number of errors. Memory-guided errors were defined as any movement before the offset of the fixation target. Corrections were defined as a return to baseline position in the next movement following an error. The relationship of the changes in eye movements which significantly differed from controls was correlated with cognitive performance as indicated by NUCOG scores using Pearson rank correlations.
RESULTS
A total of 20 bvFTD and 22 control participants were recruited. BvFTD participants, characteristics are included in Table 1. A total NUCOG score of less than 80 is considered to indicate dementia and a score of 16 or less on an individual domain is considered abnormal. Control participants had an age range from 31–77 years with an average age of 51.18 years. There was no significant difference in age between bvFTD and control participants (F(1,40) = 0.274, p = 0.604).
Two patient participants did not have NUCOGs as their cognitive screening tool, but instead had Behavioural Assessment Tool for Cognition and Higher function (BATCH) and MMSE scores (Table 2). The BATCH is a tool designed to rate cognition through observed behaviors when direct cognitive testing is not possible, and correlates highly with both the overall and individual domains of the NUCOG [36]. BvFTD and control data are presented in box-and-whisker plots with the median marked and whiskers extending to the minimum and maximum values. Mean values are reported with the statistical tests. The sample size for some of the tasks was reduced as bvFTD participants were unable to produce sufficient data for analysis, or in some cases became uncooperative. This resulted in a bvFTD participant group of 20 for the horizontal prosaccades task, 18 for vertical prosaccades, 20 for predictive saccades, 18 for self-paced saccades, 16 anti-saccades, and 14 for memory guided saccades. All results were tested for normality and non-parametric statistics used where appropriate.
Patient participants with cognitive testing results other than NUCOG. Abnormal scores have been asterisked
Prosaccades
No significant difference was found for latency for right versus leftward saccades (F(1,38) = 0.084, p = 0.774) or up versus downward saccades (F(1,34) = 1.1015, p = 0.321), so horizontal and vertical saccades were pooled within each plane for analysis. Analysis of variance revealed a significantly longer latency for the bvFTD group for both horizontal saccades (bvFTD = 218.0 ms, controls = 170.1.4 ms, F(1,40) = 24.61, p < 0.001) and vertical saccades (bvFTD = 224.0 ms, controls = 169.0 ms F(1,38) = 16.78, p = 0.0002) (Fig. 1). There was no significant interaction between diagnostic group and saccade target size.
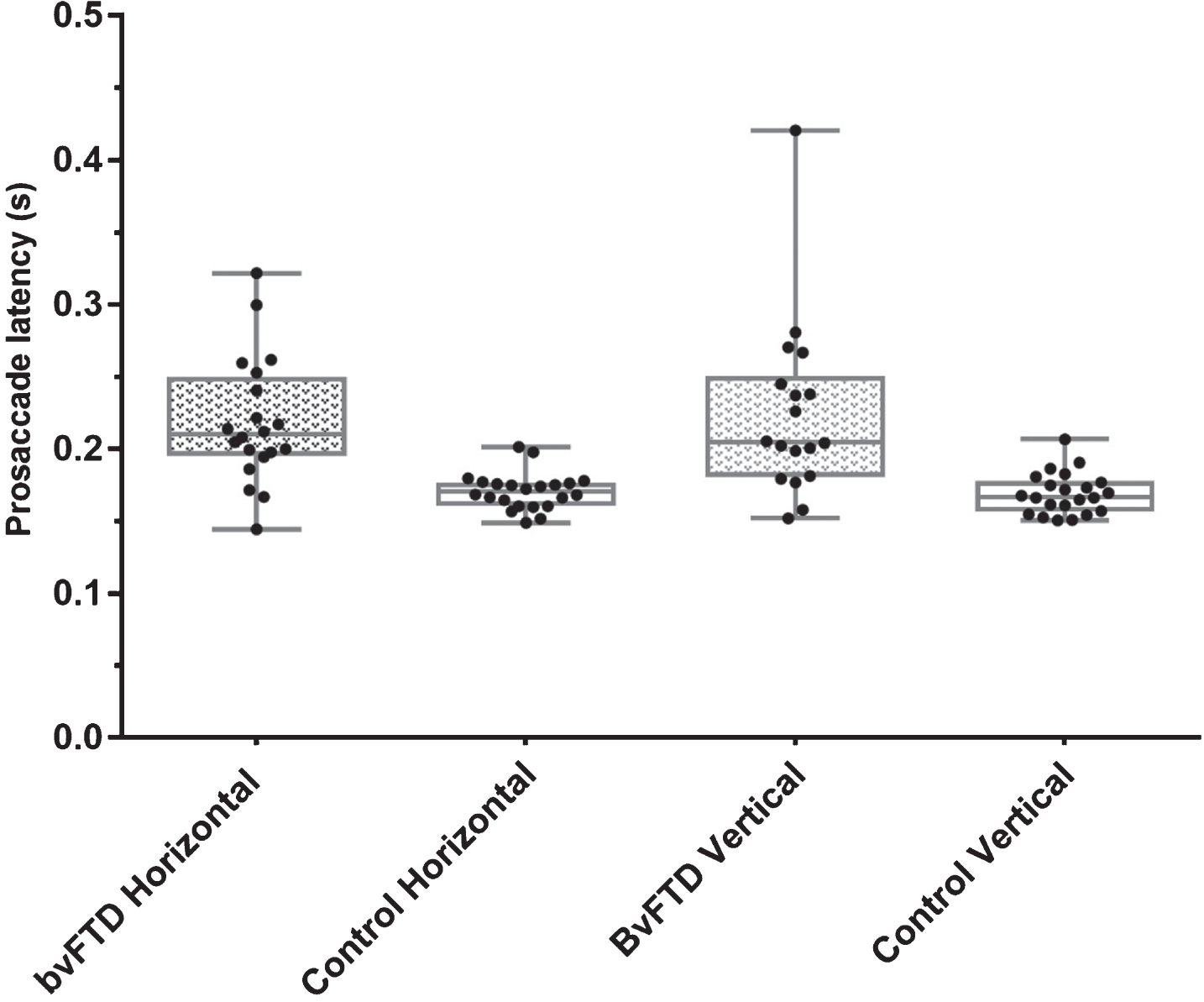
Prosaccade latencies.
No significant difference was found for right versus leftward saccade gain (F(1,38) = 0.774, p = 0.385), and so right and leftward saccades were pooled for analysis. Kruskal-Wallis examination revealed a statistically significant lower gain for the bvFTD group for horizontal gain (bvFTD = 0.830, control = 0.935 H = 7.956, p = 0.0048). There was a significant difference between up versus downward mean gain between groups (F(1,34 = 7.933, p = 0.0080), thus up and down saccades were analyzed separately. ANOVA revealed a statistically lower gain for the bvFTD group compared to controls, both in up gaze (bvFTD = 0.745, controls = 0.850, F(1,38) = 9.328, p = 0.0041) and in down gaze (bvFTD = 0.869, controls 1.047 F(1,38) = 19.34, p < 0.001) (Fig. 2).
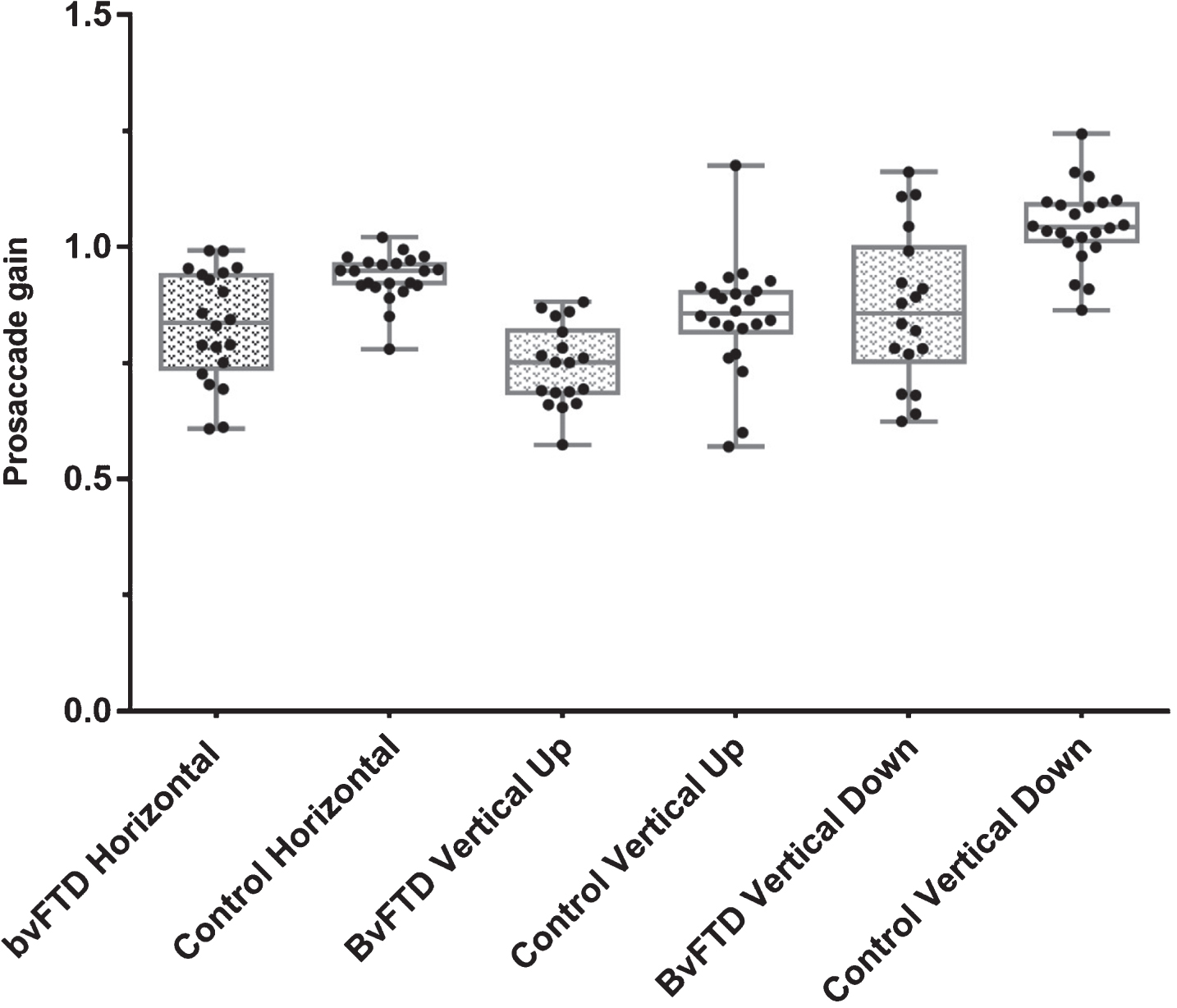
Mean gain for prosaccades.
Four bvFTD participants, results were removed from the vertical asymptotic velocity calculations due to poor fit of the data with plotting. There was no significant difference for right versus leftward horizontal velocity in bvFTD participants (F(1,38 = 0.928, p = 0.342) or up versus downwards asymptotic velocity measures (F(1,24) = 3.188, p = 0.0868), and so results were pooled in each meridian for analysis.
Analysis of variance of asymptotic peak velocity for horizontal saccades revealed a significant difference between bvFTD and controls (bvFTD = 454.8 degrees/s, control = 527.3 degrees/s, F(1,40) = 6.844, p = 0.0125). ANOVA of asymptotic peak velocity for vertical saccades did not reveal any statistically significant difference (bvFTD = 537.0 degrees/s, control = 520.1 degrees/s, F(1,33) = 0.06, p = 0.807) between bvFTD and control groups.
Predictive saccades
The bvFTD group displayed a significantly longer predictive saccade latency than control participants (bvFTD = 77.8 ms, control = – 43.1 ms, F(1,40) = 7.35, p = 0.0098).
The prosaccade latency was subtracted from the predictive saccade latency for each participant to reveal the degree of prediction occurring. There was no significant difference between bvFTD or control participants, predictive saccade latency values once prosaccade latency had been subtracted (bvFTD = – 140.3 ms, controls = – 213.1 ms, F(1,40) = 2.941, p = 0.094).
Self-paced saccades
The bvFTD group showed a significantly lower number of saccades per 30 seconds (bvFTD = 35.0, controls = 66.3, F(1,38) = 42.86, p < 0.001) (Fig. 3).
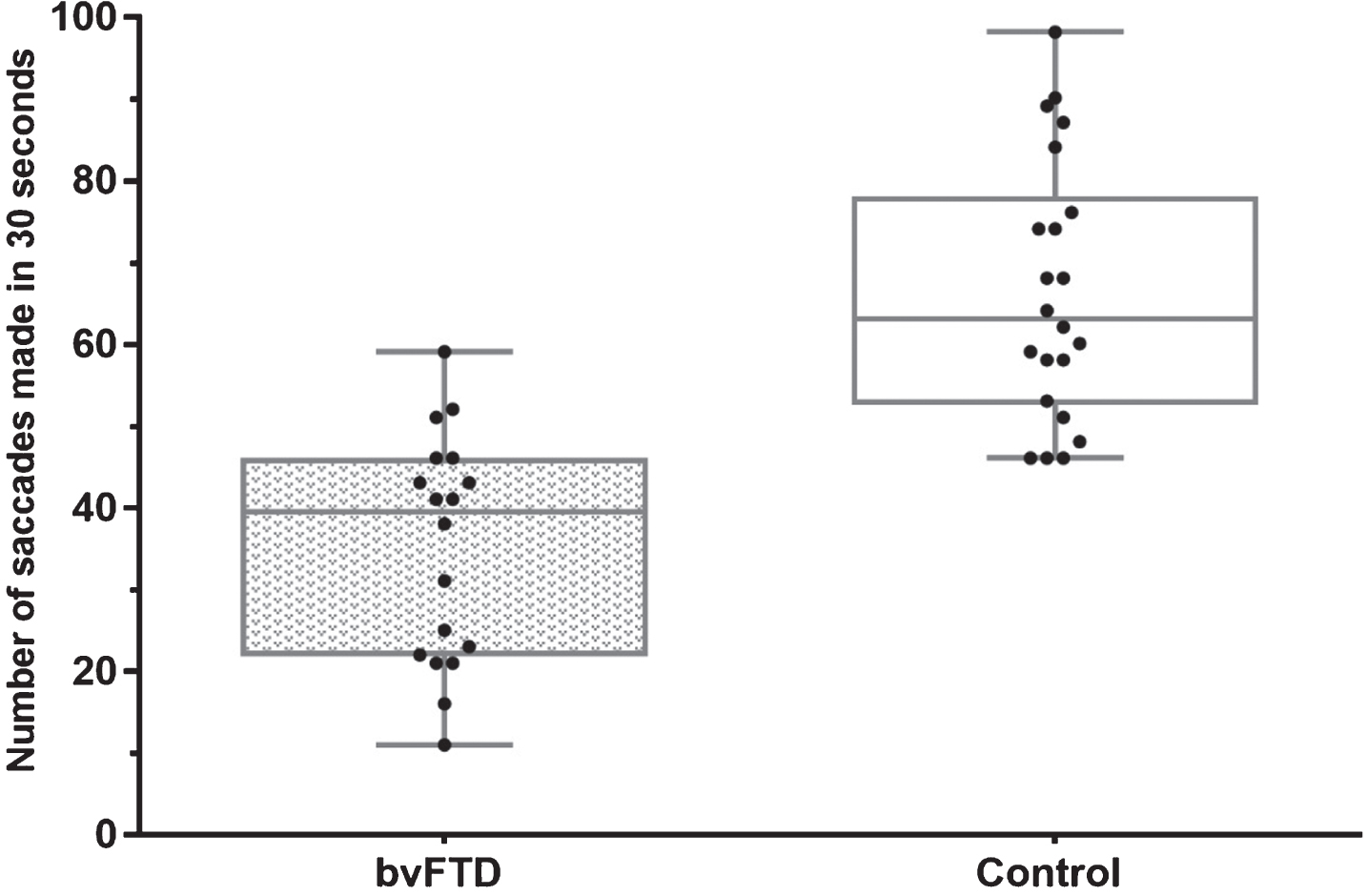
Number of self-paced saccades made in best 30 sec of trial.
Anti-saccades
There was a statistically significant increase in the proportion of error trials in the bvFTD group compared to the control group (bvFTD = 0.715, control = 0.319, F(1,36) = 49.62, p < 0.001) (Fig. 4).
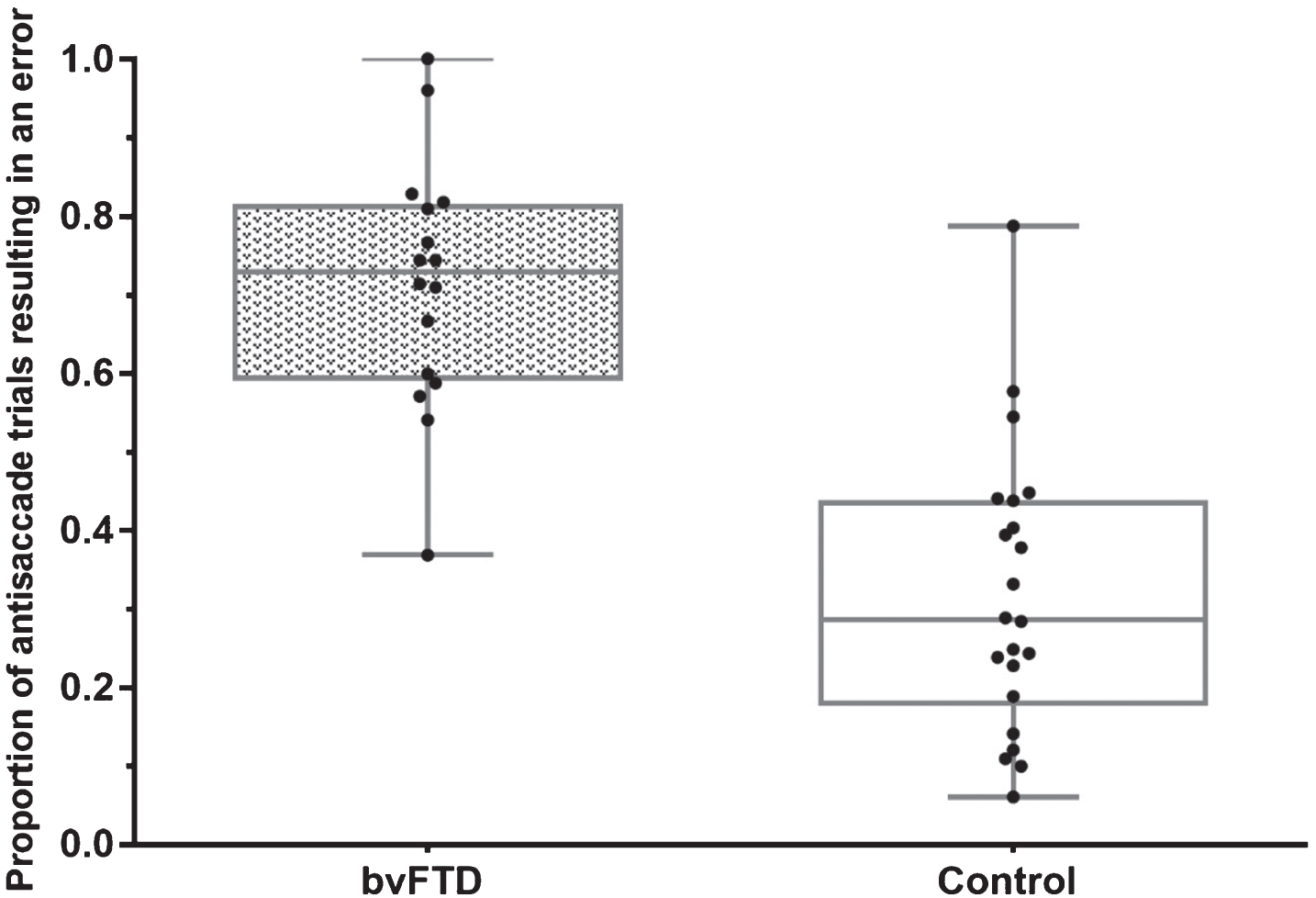
Total number of anti-saccade errors as a proportion of total analyzable trials.
BvFTD participants corrected a proportion of their errors but controls corrected a significantly higher proportion of their errors (bvFTD = 0.794, controls = 0.994 F(1,36) = 37.70, p < 0.001).
For correct anti-saccade movements the bvFTD group displayed a significantly longer latency time (bvFTD 516.1 ms, controls = 380.7 ms, F(1,35) = 7.069, p = 0.012) (Fig. 5). Latency values for horizontal prosaccades were subtracted from latency values for correct anti-saccades. After subtraction, no significant difference was seen between bvFTD and control participants, remaining latency values (bvFTD = 301.8 ms, control = 210.6 ms F(1,35) = 2.970 p = 0.094). For anti-saccade error saccades, bvFTD participants displayed a significantly longer latency than controls (bvFTD = 268.3 ms, control = 212.6 ms F(1,36) = 9.606, p = 0.0038) (Fig. 5).
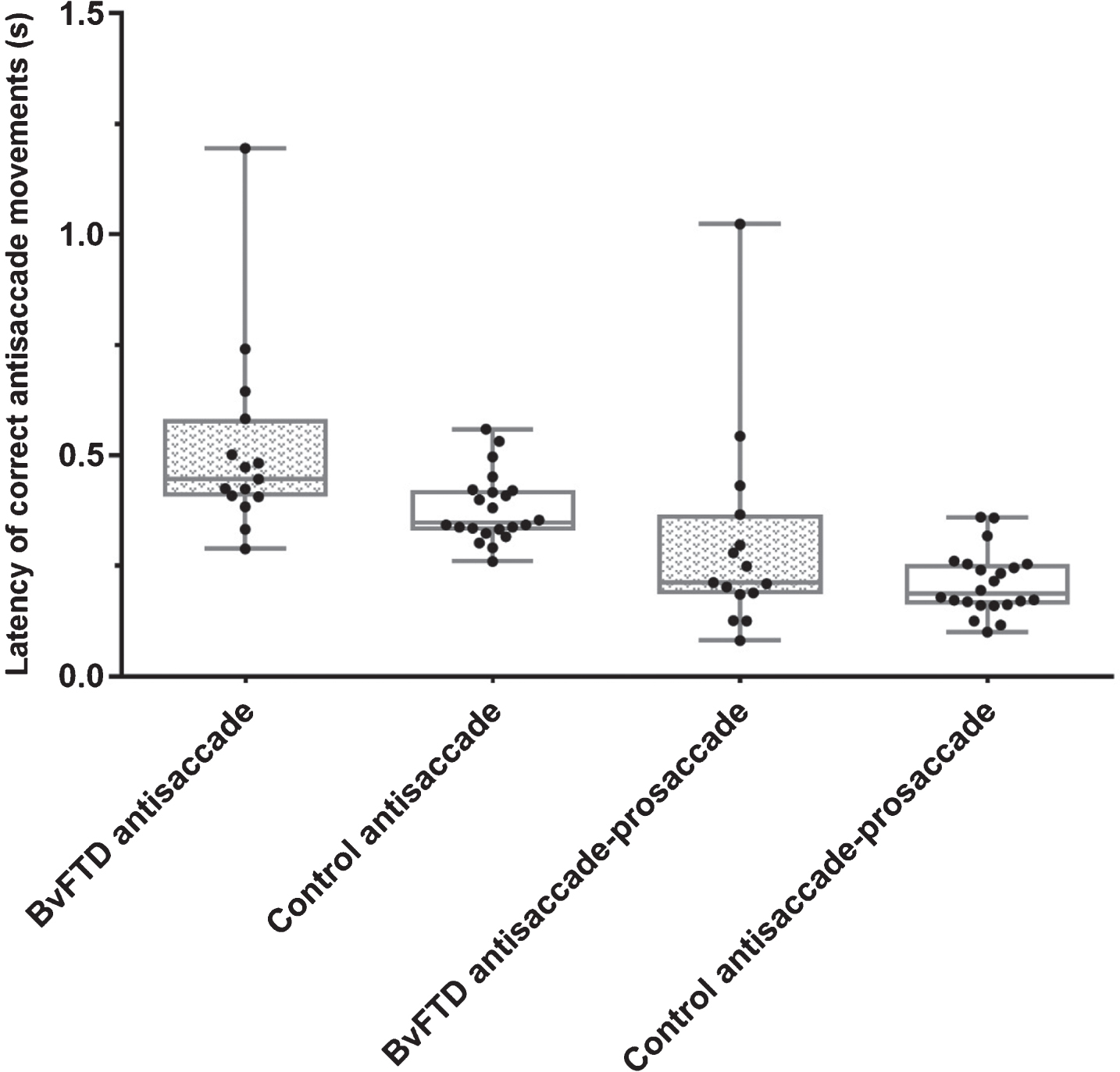
Latency of correct anti-saccade trials before and after correction for prosaccade latency.
There was no significant difference between bvFTD and control participants for anti-saccade gain (bvFTD = – 0.950, controls = – 0.840, F(1,35) = 0.902, p = 0.349).
Memory-guided saccades
The bvFTD group displayed a significantly higher proportion of errors than controls (bvFTD = 0.868, controls = 0.406, F(1,34) = 82.85, p < 0.001) (Fig. 6).
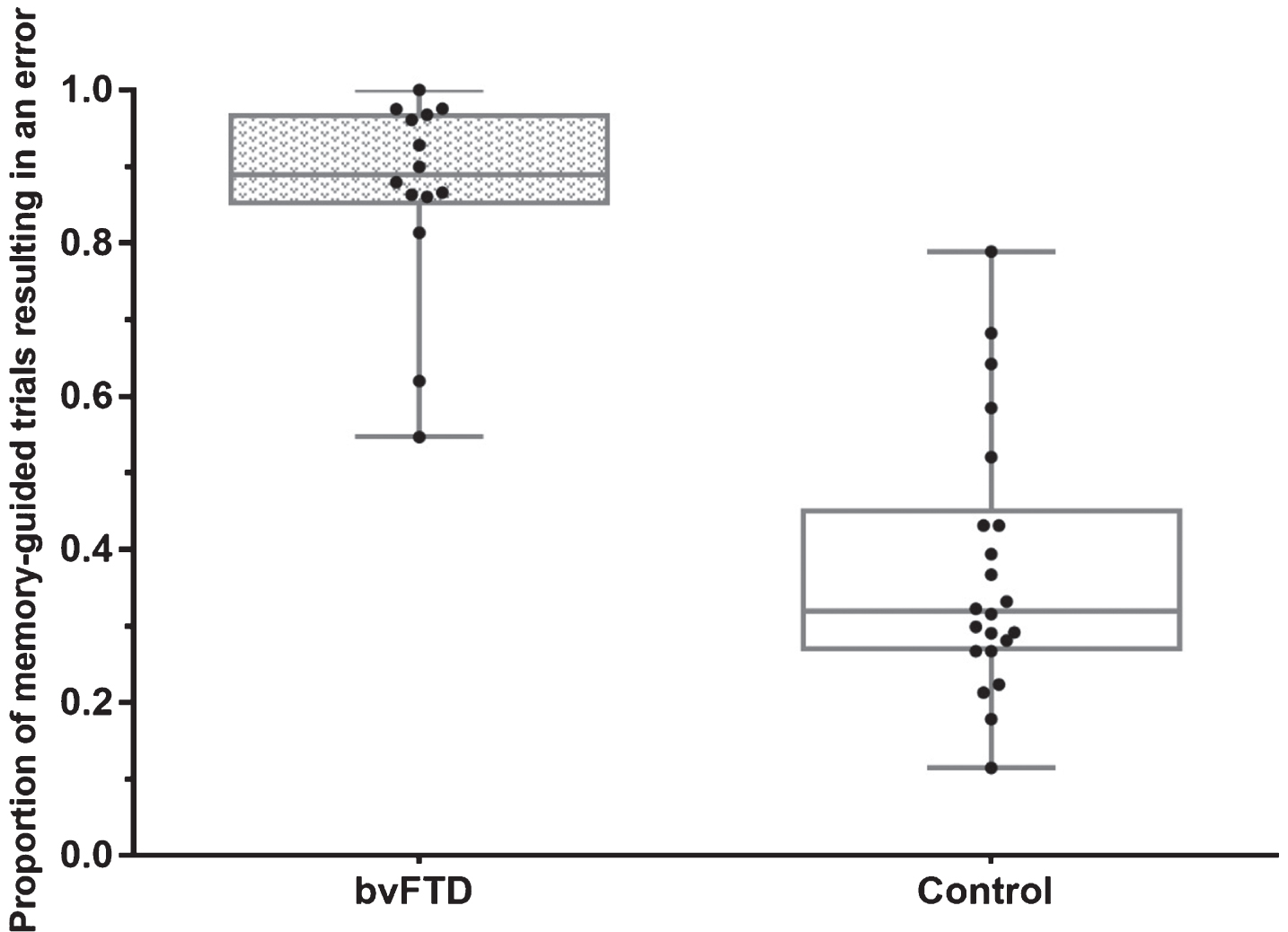
Proportion of total memory-guided trials that resulted in an error.
There was no significant difference in the proportion of errors corrected between bvFTD and control groups (bvFTD = 0.796, controls = 0.704, F(1,34) = 1.876, p = 0.180).
The bvFTD group displayed a significantly longer latency than controls (Fig. 7) (bvFTD = 488.2 ms, controls = 330.9 ms, F(1,34) = 9.820, (p = 0.0035). The latency difference remained significant once prosaccade latency values were subtracted for each participant (bvFTD = 269.9 ms, controls = 160.9 ms, F(1,34) = 5.359, p = 0.027).
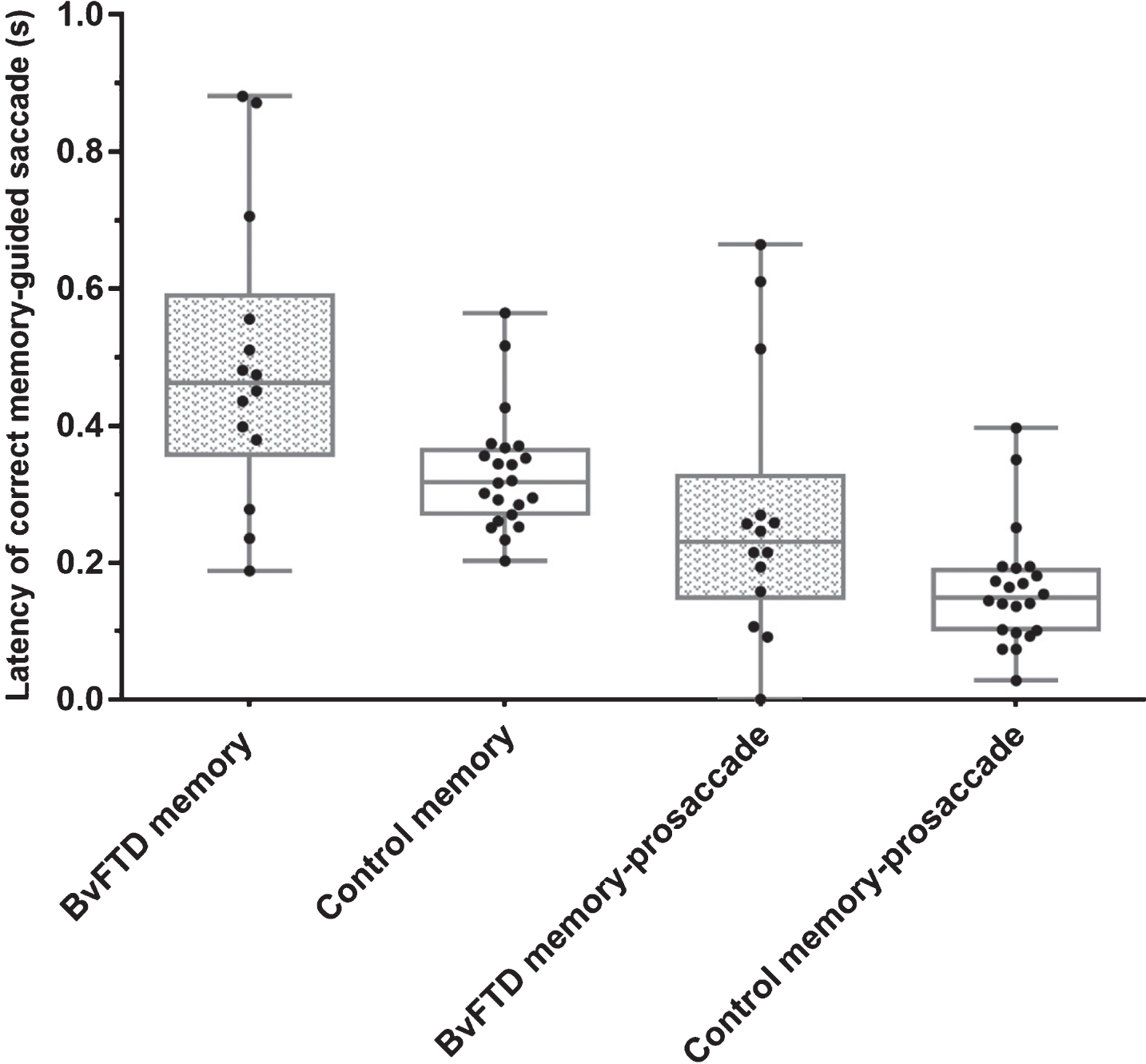
Latency of correct memory-guided saccades before and after correction for prosaccade latency.
Correlations between saccades and NUCOG data
Pearson’s correlation of NUCOG scores for bvFTD participants was not significant for prosaccades, predictive, self-paced, or memory-guided saccades.
Pearson’s correlational analysis revealed a statistically significant correlation between total NUCOG score and the proportion of total anti-saccade errors corrected. Examining the individual components of the NUCOG revealed an unsurprising correlation with executive function. No other domains were significantly correlated. Significant correlations after Holm-Bonferroni correction are indicated with an asterisk in Table 3.
Correlation coefficients between anti-saccade errors and NUCOG cognitive domains
DISCUSSION
BvFTD participants as a group displayed an increased latency across a range of saccadic paradigms. Our findings are consistent with reports of a significant difference between bvFTD and control prosaccades [19]. This finding is not consistent with reports of no change in saccadic latency [20, 21]. The increased latency has two hypothetical causes: either a defect in the motor pathway or a delay in the saccadic command coming from higher cortical areas such as the frontal eye fields (FEF). BvFTD affects the frontal lobes, including the FEF, which are involved in triggering higher order saccades. The disorder is not traditionally thought to affect the brainstem, however bvFTD lies on a spectrum and may occur concurrently with conditions which do show brainstem changes, including parkinsonian disorders and motor neuron disease. This overlapping spectrum produces the possibility of a motor pathway defect. TDP molecular changes have been reported in the superior colliculus in bvFTD [37], and these changes are thought to be anterograde to cortical changes. We believe this is unlikely to be the cause, however, as this does not fit with the Boxer et al. [22] finding of increased latency being seen only in patients with tau-based pathology.
Our study examined prosaccade latency as a whole without separating the movements into express saccades and longer prosaccades. There is a possibility that there are changes to either one or both of these movement groups, reflecting input from the brainstem only for reflex, and from both the brainstem and frontal lobe for longer saccades.
No significant difference is seen in bvFTD between right and left prosaccade gain; however, similar to what is seen in PSP [38] and Neimann Pick type C [39], there is a significant difference in saccadic gain for up and down gaze. In agreement with Boxer et al. [22], both up and down gaze gain were significantly reduced for bvFTD participants when compared to controls; the magnitude of this reduction was much greater for downgaze. Within this result there is a large spread of gains displayed by bvFTD participants. This variance may be explainable by the presence of different molecular subgroups within our cohort or by differences in the stage of disease progression and this warrants further investigation. Unlike in parkinsonian disorders dominated by the presence of tau and with basal ganglia changes, no significant difference was found between the participant groups for asymptotic peak velocity of vertical saccades. Vertical saccadic velocity not being significantly different to controls is a finding consistently reported in the literature [20, 21] and may be useful in differentiating bvFTD cases from PSP patients in the clinic. In contrast to vertical saccades, a small difference in horizontal velocity was found between bvFTD and controls. This reflects the independence of the horizontal and vertical saccadic burst neurons. While vertical saccades tend to be more frequently impaired in neurodegenerative diseases, in Gaucher Type 3 disease it is the horizontal saccades that are lost first [40].
On the anti-saccade task, bvFTD participants displayed an increased number of directional errors. In agreement with the literature, a large portion of these errors were corrected, indicating that while participants were unable to inhibit making the errors, they were capable of understanding the task, recognizing when they had made a mistake and what action was needed to correct it. In contrast to the anti-saccade results in Garbutt et al. [21], bvFTD participants also made significantly more uncorrected errors than controls.
Total anti-saccade errors as a proportion of all analyzable trials were not significantly correlated with the NUCOG or any of its domains. Exploring error types, the proportion of anti-saccades which were corrected was significantly correlated with overall NUCOG score and with the executive function subscale. This finding agrees with correlations found between executive function and anti-saccade errors in aging [41] and AD [28, 42]. This highlights the cognitive domain requirements in the anti-saccade task. The capacity to make anti-saccade corrections is a significant point of difference between bvFTD and many overlapping conditions, including AD, in which anti-saccade correction rates are low and decline further with increasing disease severity.
In addition to prosaccades and anti-saccades, we examined several saccadic paradigms which have not been characterized previously in bvFTD: predictive, self-paced, and memory-guided saccades. Predictive saccades are very similar to prosaccades in that the task may still be satisfactorily completed by continuing the same behavior necessary for prosaccades. There is, however, a degree of learning that can lead to responses with zero or even negative latencies. This is the predictive component, thought to represent learning, which utilizes additional processing beyond that required for prosaccades, with additional inputs from the frontal eye field, supplementary eye fields, dorsomedial thalamus, anterior cingulate, and hippocampus [43]. BvFTD participants as a group display good prediction, as evidenced by the absence of a significant difference in latency once prosaccade latency values for each participant were removed. This suggests that their ability to implicitly learn stimulus timing is unimpaired, though low-level saccade triggering, as indicated by the prolonged prosaccade latency, is delayed.
Self-paced saccades are a voluntary saccadic paradigm not previously reported in bvFTD patients, which have been linked with frontal lobe activity and integrity [44]. Self-paced saccades are relatively simple for the patient to understand and involve additional input from the caudal anterior cingulate gyrus, supplementary motor area, supplementary eye field, cerebellar vermis, right fusiform and lingual gyri, and right insula [45, 46]. Self-paced saccade rate is decreased in other conditions, including Neimann Pick type C [47], moderate to severe traumatic brain injury [48], and post-concussion syndrome [44]. The bvFTD participant group produced a lower number of saccades when compared with controls. As an internally-driven task, the increased inter-saccadic interval displayed by participants may reflect atrophy affecting the FEF. Given the simplicity of this task it may have future utility clinically for differentiating bvFTD patients from controls early in the disease, or for assessing those in whom cognitive testing is difficult.
Memory-guided saccades present increased difficulty relative to prosaccades, self-paced, and predictive saccades, and a few of the bvFTD participants were unable to complete the task. The memory-guided task requires significant input from the supplementary eye field, as well as the DLPFC, anterior cingulate, frontal premotor cortex, and frontal and parietal eye fields [49]. BvFTD performance for memory-guided saccades was similar to that seen in anti-saccades; bvFTD participants had a significantly increased total error rate, with a large proportion of these being corrected. Errors on the task were more frequently uncorrected than was the case for anti-saccades. Unlike in anti-saccades, error rates were not significantly correlated with any of the NUCOG cognitive domains. This lack of a correlation could be due to the different error types possible in the task [50]. BvFTD participants appear able to understand both the anti-saccade and memory-guided tasks, as seen by their correcting errors, but they nonetheless are unable to inhibit these errors, and appear to have more difficulty with the memory-guided task than controls. This is evidenced by the increased latency which remains after the prosaccade latency is subtracted out. Memory-guided saccades require greater levels of inhibition; not only is there the chance of making a reflexive prosaccade but there is also the possibility of making a volitionally planned response before the central stimulus is extinguished [50, 51]. The DLPFC has been shown to be activated in both memory-guided and anti-saccades, and DLPFC atrophy has previously been linked to increased anti-saccade error rates [29]. DLPFC atrophy in bvFTD patients could explain the similarity in the pattern of errors generated in these higher-order tasks.
Similar to anti-saccades and prosaccade latencies, which have been previously reported, self-paced, memory-guided, and predictive saccades displayed a large variability in results achieved which may reflect our diverse cross-sectional group. Further evaluation examining both progression and underlying molecular subtype is warranted. Saccadic testing has been considered a quantitative method for measuring motor changes and for probing cortical contributions to specific behaviors. Saccadic testing in AD yielded a significant difference between patients and controls; however, patients individually show a large range of saccadic performance, with some patients displaying eye movements within the normal range. A similar situation is seen in bvFTD, with significant differences between group means but with significant overlap in the range of control and clinical participants’ responses. Two reasons could account for the variance seen in bvFTD patients’ responses: clinical progression and/or differences in the underlying molecular pathology. Horizontal prosaccades and self-paced saccades appear to demonstrate the greatest separation between bvFTD and control participants; however, neither task is without overlap.
Limitations and future directions
There is currently no definitive treatment for frontotemporal dementia. While there are as yet no illness-modifying medications available, medications are used in dementia care to control behavioral and psychological symptoms of the condition. A few of the drugs used in our patient group have the potential to affect eye movements. These drugs are commonly used, and so exclusion based on their use would have reduced recruitment numbers and significantly affected the power of the study. Saccadic velocity is the most commonly reported affected parameter [52], particularly at higher doses [53]. We noted a small decrease in horizontal prosaccade velocity in our bvFTD cohort and there is a possibility that this is a medication effect.
This battery of eye movement tasks in bvFTD participants elicited a distinctive pattern of change based on the brain areas typically affected in bvFTD. Some eye movements which have been reported as significantly impaired in other neurodegenerative groups, such as peak velocity in PSP, fall within normal limits in bvFTD. Examining a battery of saccades with increasing input from a wide range of cortical regions may allow the practitioner to detect and monitor change in specific regions. This would be worth investigating both over time, and in comparison, to other neuropsychiatric groups, and to examine with concurrent neuroimaging to probe the relationship between these changes and brain structure. Executive function changes, anti-saccade errors, and anti-saccade corrections are non-specific findings; thus, these must be treated with caution when considering diagnosis. Eye movement changes may be correlated with specific neuropsychological tests; however, the aim of this study was to explore changes in saccadic paradigms themselves in bvFTD rather than to examine their relationship to other assessments. Future studies could further examine the relationship between eye movements and detailed neuropsychological testing, as well as look at their relationship to the clinical dementia rating scale, to examine impairments beyond cognitive changes.
Our results must be interpreted with caution as they are based on group changes which show significant variability and do not examine differences in individual underlying molecular pathology; however, these paradigms are simple and warrant further investigation with additional patient subtyping.