
Abstract
Background:
Older people with cognitive impairment, including dementia and delirium, are high users of acute care services internationally. Potentially inappropriate medication (PIM) use may be associated with adverse outcomes, including hospital re-admission, functional disability, and mortality.
Objective:
This systematic review aimed to quantify and compare the prevalence of PIMs in older inpatients with and without cognitive impairment.
Methods:
A systematic search of observational studies was performed independently assessed by two reviewers in Embase, Medline, PsycINFO, International Pharmaceutical Abstracts, Scopus, and Informit. Articles published in English during the period January 2007–June 2017 that reported PIM prevalence in hospital inpatients ≥ 65 years were included. PIMs were defined as the presence of polypharmacy (multiple medication use) and using implicit or explicit tools, such as the Beers criteria, and ‘Screening Tool of Older Person’s Prescriptions’ (STOPP).
Results:
47 articles were included. In studies measuring polypharmacy (n = 15), the prevalence of PIMs ranged from 53.2% to 89.8% and 30.4% to 97.1% for inpatients with and without cognitive impairment, respectively, and 24.0% to 80.0% when cognitive status was unreported. In studies employing explicit and implicit tools (n = 35), the prevalence of PIMs when cognitive impairment was reported ranged from 20.6% to 80.5% using the Beers criteria, and 39.3% to 88.5% using STOPP. When cognitive status was unreported, the prevalence of PIMs ranged from 7.0% to 79.2% using the Beers criteria, and 20.0% to 63.4% using STOPP.
Conclusion:
Our findings suggest a high prevalence of PIMs in older inpatients with and without cognitive impairment. Future studies should investigate the impact of PIM use on patient-centered outcomes, such as functional status and quality of life, to inform enhanced acute care services.
Keywords
INTRODUCTION
Potentially inappropriate medication (PIM) use is of major concern in older adults (aged 65 years and over) due to greater sensitivity for adverse drug events (ADEs) related to altered pharmacokinetics, pharmacodynamics, and drug-disease interactions [1, 2]. PIMs can be defined as specific medications or medication classes which should be avoided, as they are either ineffective or pose an unfavorable risk of harm over benefit when safer or equally effective alternatives are available [3]. Common approaches used to quantify PIMs include assessing for multiple medication use (such as polypharmacy) [4], and examining exposure to individual high-risk medications using explicit and implicit assessment tools [2].
While there is no universally accepted definition of polypharmacy, it is commonly defined as the use of five or more regular medications [5]. Polypharmacy is recognized as the most significant risk factor for ADEs in older adults, with an estimated prevalence of 20% to 40%, depending on the age, comorbidities, and number of prescribers for the population studied [4, 6]. Even though polypharmacy may be appropriate in certain situations, especially when medications are clinically indicated to manage several medical conditions [7], studies have shown that polypharmacy is associated with negative health outcomes in older people, including increased rates of falls, frailty, hospitalization and mortality [8].
The appropriateness of prescribed medications in older people can also be assessed using implicit and explicit criteria [9]. The most frequently used explicit criteria include the Beers criteria [10], as well as the ‘Screening Tool of Older Person’s Prescriptions/Screening Tool to Alert Doctors to Right Treatment’ (STOPP/START) [11]. The prevalence of PIMs varies widely according to the Beers and STOPP criteria, with current evidence amongst adults living in residential long-term care facilities determined the prevalence of PIMs to range from 21.3% to 63.0% using the updated Beers criteria of 2003, and 23.7% to 79.8% when assessed using STOPP [12]. However, PIM use has not yet been systematically documented in the acute care setting.
Furthermore, the improved recognition for considering cognitive impairment when assessing PIMs is reflected by the inclusion of a separate PIM list for people with dementia and delirium in the recently updated version of the Beers criteria [10]. Older people with cognitive syndromes are more likely to experience a more pronounced sensitivity to ADEs [13, 14]. It has also been reported that patients with dementia are prescribed an average of 5–10 medications, with the majority of treatments indicated for other comorbid medical conditions [13]. The use of multiple medications in this population, particularly anticholinergic and sedative agents, may worsen memory loss and increase functional impairment [13]. Established measures, such as the Anticholinergic Cognitive Burden (ACB) scale, have been developed to determine the prevalence of PIMs for people with varying degrees of cognitive impairment [15] and those with advanced dementia [16]. A recent review found the prevalence of PIMs in older people with cognitive impairment and/or dementia living in the community setting to range from 15% to 47%, with the most frequently implicated PIMs being anticholinergics and benzodiazepines [17]. A further study of Finnish community-dwelling patients determined that those with Alzheimer’s disease had greater exposure to these high-risk drug classes, documenting a prevalence of 51.4% versus 33.3% when compared to individuals without the disease [14].
Providing appropriate medical care for older inpatients with cognitive impairment is of particular interest since they are high users of acute care services internationally [18]. The consequences of acute admissions into hospital for older people with dementia are substantial, and may lead to longer hospital stays and a greater risk of adverse outcomes, including delirium, falls, and institutionalization after discharge [19–21]. Improving acute care services has been identified as a key priority, as hospitalization disrupts continuity of care, increases caregiver load, and may result in patient distress brought on by an unfamiliar environment and increased medication burden [22]. Many patients are administered PIMs on admission, during admission and on discharge, including anticholinergics, antipsychotics and benzodiazepines, all of which may further impair cognition and increase the risk of hospital re-admission [23].
Despite the need to enhance acute care services for people with cognitive impairment, many previous studies assessing medication appropriateness have not routinely reported the cognitive status of included participants, irrespective of the study setting [13]. Currently, limited evidence exists that systematically compares PIM use among older people by level of cognitive function, even when cognitive impairment is reported. Therefore, the aim of this systematic review was to quantify and compare the prevalence of PIM use among older adults with and without cognitive impairment in the acute care setting.
METHODS
Key definitions
For the purposes of this review, PIMs were defined as the presence of polypharmacy and/or specific high-risk medications captured by implicit and explicit tools. Due to the expected variability in the definition of polypharmacy, we used definitions proposed by the authors of included articles instead of implementing our own judgement and assigning a particular cut-off. The selected number of medications labelled as polypharmacy did not eliminate those which were clinically indicated; therefore, the use of multiple medications should only be regarded as potentially inappropriate. Additionally, explicit tools, such as the Beers [10] and STOPP criteria [11], refer to consensus lists of drugs considered to be potentially inappropriate in older people, whereas implicit tools, such as the ‘Medication Appropriateness Index’ (MAI) [24] and ‘Assessing Care of the Elderly’ (ACOVE) [25], require clinical judgement to assess PIMs. Cognitive impairment was defined as the diagnosis of mild, moderate, or severe cognitive impairment, delirium, or any form of dementia.
Database search
We performed a systematic search of six electronic databases (Embase, Medline, PsycINFO, International Pharmaceutical Abstracts, Scopus, and Informit) for original observational research articles, including cohort and cross-sectional studies, published from January 2007 through June 2017. Despite several implicit and explicit criteria having been published before this period, our review has allowed for time to adapt these tools into updated criteria which best reflect current prescribing patterns and practices. The key word search was as follows: (potentially inappropriate medic* OR potentially inappropriate drug* OR potentially inappropriate OR inappropriate OR inappropriate prescribing OR overprescribing OR polypharmacy OR multiple medic* OR high-risk drug* OR beers criteria OR medication appropriateness index OR STOPP) AND (hospitali?* OR hospital OR hospital patient OR inpatient OR acute care) AND ((cognitive* OR impair* OR mild cognitive impairment OR memory loss OR memory impairment OR dementia OR alzheimer OR delirium) OR (aged OR elderly OR geriatric OR old OR older)). The same key words were used across all databases, and terms searched as free-text words, supplemented with the respective Thesaurus (MeSH or Emtree terms) when available.
Inclusion and exclusion criteria
The ‘Preferred Reporting Items for Systematic reviews and Meta-Analyses’ (PRISMA) guidelines were followed throughout this review [26]. Full-text articles were included if they reported on the prevalence of PIMs using polypharmacy, or explicit or implicit tools. We excluded articles if they: 1) were conducted in an outpatient setting, such as nursing homes and community-dwellings; 2) consisted of any participants under the age of 65 years (even when a significant proportion of study participants were aged over 65 years); 3) included case reports, case series, clinical trials and systematic reviews; or 4) were written in languages other than English.
Data extraction
After removal of duplicates, two reviewers (MR and AC) independently screened the articles for potential suitability based on titles and abstracts. Full-text articles were then assessed for eligibility by both reviewers (MR and AC), and final selection was made by consensus with a third author (DG) reviewing discrepancies. Additional articles were identified by one reviewer (MR) through conducting a manual search of the reference list of identified articles, with eligibility determined by the two other reviewers (AC and DG). The following information was extracted: 1) author, country, and year of the study conducted; 2) number of participants and mean age; 3) whether cognitive impairment was reported, and if so, the definition of cognitive impairment and proportion of participants diagnosed; 4) the prevalence of PIMs assessed by polypharmacy and/or explicit or implicit tools; and, where available, 5) the most prevalent PIM measured as a proportion of overall PIMs. Only data related to hospital admission were extracted for this review.
Quality assessment
A quality assessment was performed for all included studies using the ‘Cochrane Risk of Bias Assessment Tool’ for controlled before-after studies [27]. Nine standard allocation criteria categorized studies as possessing low, high, or unclear risk of bias.
RESULTS
Search results and study characteristics
A total of 1,916 articles were identified, with 144 full-text articles reviewed, of which 41 were included in the review. Another six articles were identified after a manual search of the reference list of identified articles, resulting in a total of 47 articles (Fig. 1). Cognitive impairment was reported in 19 articles, with no reported cognitive status in the remaining 28 articles. The most common PIM measure involved explicit and implicit criteria (n = 35), as opposed to articles focusing on polypharmacy only (n = 12) or a combination of measures (n = 3). Most studies were conducted in Europe (42.6%) and Asia (23.4%), and smaller numbers of studies in Australia (12.8%) and North America (8.5%).
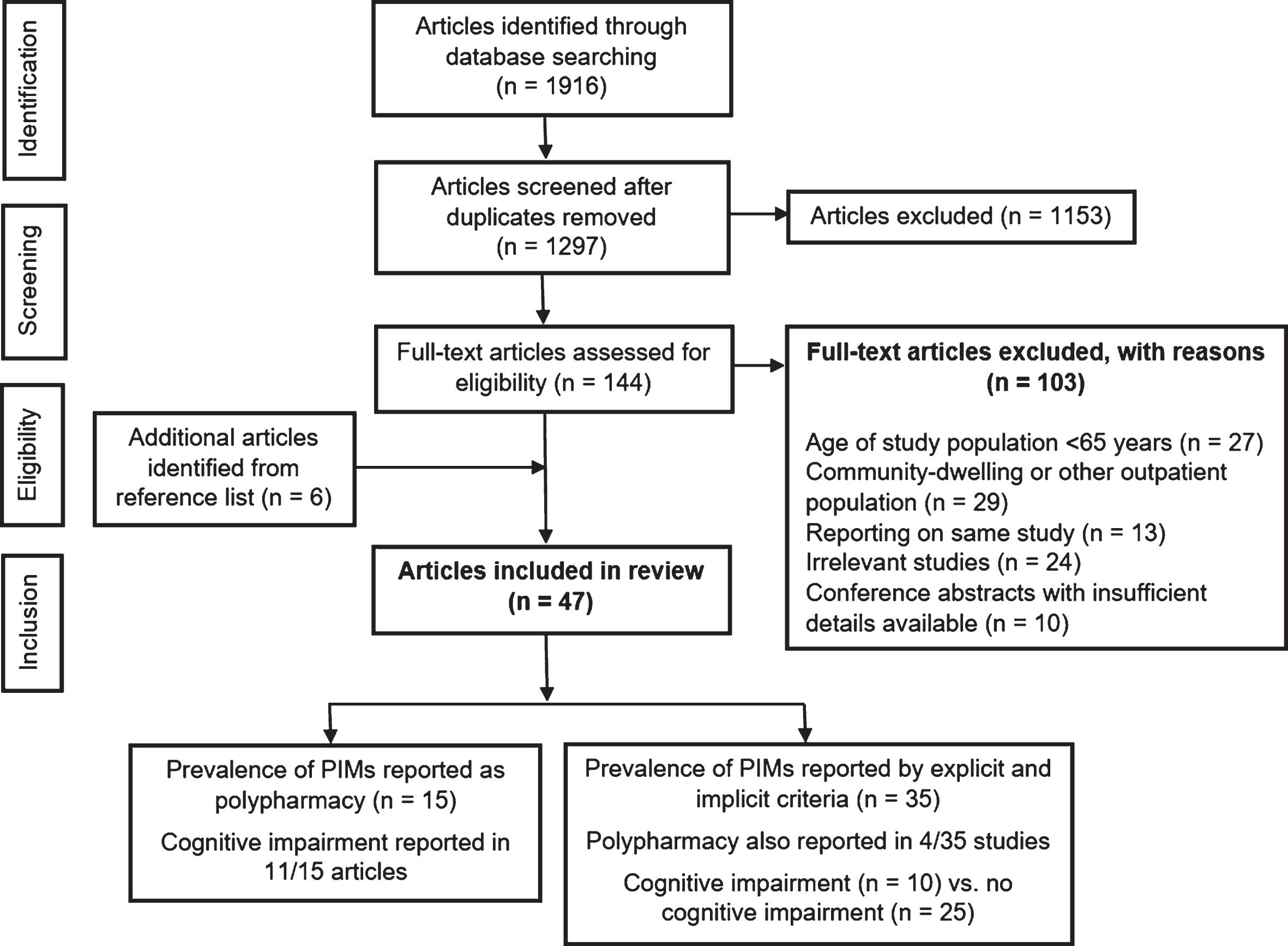
Study inclusion and exclusion criteria flowchart. PIM, potentially inappropriate medication.
Prevalence of PIMs defined by polypharmacy in older inpatients with and without cognitive impairment
Polypharmacy exposure was reported according to cognitive status in 11 out of 15 studies [4, 28–35], compared to the remaining four studies where cognitive status was not reported [36–39] (Table 1). It was defined as the use of five or more medications in 11 studies [4, 37], six or more medications in three studies [31, 39], and 10 or more medications in one study [38]. Polypharmacy was documented at the time of hospital admission in nine studies [4, 34–36], during hospital stay in four studies [30, 32, 39], and at hospital discharge in two studies [33, 37]. Cognitive impairment was defined as the diagnosis of dementia in four studies [4, 35], delirium in three studies [4, 33], and any form of cognitive impairment in five studies [23, 33].
Prevalence of potentially inappropriate medications (PIMs) defined by polypharmacy in older inpatients with and without cognitive impairment (n = 15)
*Sorted in descending order of the proportion of study participants with reported cognitive impairment. †Comparison data of polypharmacy and cognitive status within the study was obtained after contacting authors. ‡Based on the entire population. Comparison data of polypharmacy and cognitive status within the study was unavailable despite contacting authors. NOTE. Studies marked ‘NA’ did not report polypharmacy based on cognitive status.
The prevalence of polypharmacy ranged from 53.2% to 89.8% in studies including older people with cognitive impairment reported [4, 35], whereas the prevalence of polypharmacy ranged from 30.4% to 97.1% in studies including older people without cognitive impairment [4, 31–35]. In the four studies when cognitive status was not reported, the prevalence of polypharmacy ranged from 24.0% to 80.0% [36–39]. The prevalence of polypharmacy in the three studies which reported dementia only, and not any combination of disorders, was higher in older people living with dementia (56.7% to 83.7%) versus no dementia diagnosis (51.5% to 76.8%) [19, 35].
Prevalence of PIMs defined by explicit or implicit tools in older inpatients when cognitive impairment was reported
Ten articles reported the prevalence of PIMs using either explicit assessment criteria, including the Beers, STOPP and START criteria; or implicit tools, including ACOVE and MAI [1, 40–46] (Table 2). PIMs were documented at the time of hospital admission in seven studies [1, 40–43], and during hospital stay in three studies [44–46]. Cognitive impairment was reported as one or more of the following: dementia in four studies [40, 46]; impaired cognitive function in three studies [1, 43]; mild, moderate, or severe cognitive impairment or deterioration in three studies [23, 41]; and delirium in one study [45]. All participants were found to have cognitive impairment in one study only [40].
Prevalence of potentially inappropriate medications (PIMs) defined by explicit or implicit criteria for studies with a proportion of participants with cognitive impairment (n = 10)
ACOVE, Assessing Care of the Elderly; MAI, Medication Appropriateness Index; MMSE, Mini-Mental State Examination; PIM, potentially inappropriate medication; START, Screening Tool to Alert Doctors to Right Treatment; STOPP, Screening Tool of Older Person’s Prescriptions. *Sorted in descending order of the proportion of study participants with reported cognitive impairment. NOTE. Studies marked ‘NA’ did not use the Beers criteria to capture PIM use.
The prevalence of PIMs varied from 20.6% to 80.5% between six studies which used different versions of the Beers criteria, either 2003 [40, 42], 2012 [44–46] or 2015 version [23]. The seven studies based on STOPP criteria reported a prevalence of 39.3% to 88.5% [1, 43–45], and the four articles using START criteria recorded a prevalence of 41.0% to 64.7% [1, 45]. ACOVE criteria were used in one study, reporting a prevalence of 56.3% [45]. One study also employed the MAI assessment tool, providing a mean sum score of 23.0 (range 0–86), with a greater number indicating the presence of PIMs after summing up individual appropriateness scores from 0–18 [28].
Benzodiazepines were found to be the most commonly prescribed PIM, with a prevalence ranging from 15.1% to 61.3% of all PIMs when STOPP criteria were employed [1, 45], and 16.6% to 39.5% of all PIMs when assessed using several versions of the Beers criteria [23, 44–46].
Prevalence of PIMs defined by explicit or implicit tools in studies when cognitive status was not reported
A total of 25 articles assessed the prevalence of PIMs without cognitive status reported [9, 47–69] (Table 3). Explicit criteria which were used include the Beers criteria, ‘Healthcare Effectiveness Data and Information Set’ (HEDIS), ‘Improving Prescribing in the Elderly Tool’ (IPET), the German PRISCUS tool, START and/or STOPP. Implicit assessment tools which were used include ACOVE and MAI. PIMs were documented at the time of hospital admission in eight studies [50, 69], during hospital stay in 16 studies [9, 68], and at hospital discharge in one study [65].
Prevalence of potentially inappropriate medications (PIMs) defined by explicit or implicit criteria in studies when cognitive status was not reported (n = 25)
ACOVE, Assessing Care of the Elderly; HEDIS, Healthcare Effectiveness Data and Information Set; IPET, Improving Prescribing in the Elderly Tool; MAI, Medication Appropriateness Index; PIM, potentially inappropriate medication; START, Screening Tool to Alert Doctors to Right Treatment; STOPP, Screening Tool of Older Person’s Prescriptions. *Sorted in descending order of prevalence of potentially inappropriate medications. NOTE. Studies marked ‘NA’ did not use the Beers criteria to capture PIM use.
The prevalence of PIMs varied from 7.0% to 79.2% in 21 studies which employed any version of the Beers criteria [9, 60–69], with most studies using the updated lists in 2003 [48, 69] or 2012 [9, 67]. STOPP criteria was implemented in 12 studies, with a prevalence of PIMs ranging from 20.0% to 63.4% between studies [9, 68]. Four studies used START criteria and reported a prevalence of 11.0% to 74.0% [9, 68]. Two studies relied on IPET criteria to provide a prevalence of 25.4% and 27.4% [9, 66]. HEDIS, PRISCUS and ACOVE criteria were all used in one study each, reporting a prevalence of PIMs to be 9.7% [66], 14.3% [58] and 59.4% [48], respectively. Only one study utilized the implicit MAI tool, reporting a mean sum score of 5.5 (range 0–12) [66].
The most prevalent PIM prescribed were benzodiazepines, ranging from 10.5% to 76.0% of all PIMs using several versions of the Beers criteria [48, 69]. Other highly prevalent PIMs included calcium channel blockers leading to chronic constipation (11.7% to 18.5% of all PIMs) when employing the STOPP criteria [60, 68], and the combination of nonsteroidal anti-inflammatory drugs (NSAIDs) with anti-hypertensives or long-term use of NSAIDs (13.3% to 75.0% of all PIMs) using several versions of the Beers criteria [56, 68].
Risk of bias assessment
Articles included in this systematic review were either cohort studies (n = 16) or cross-sectional studies (n = 21), and each were assessed using the ‘Cochrane Risk of Bias Assessment Tool’ (Supplementary Table 1). Out of the 25 studies which used implicit and explicit criteria and did not report cognitive status, 19 studies were graded as having either an unclear or high risk of bias due to inadequately addressing outcome data [9, 60–69], compared to five of 10 studies which reported cognitive impairment [41, 43–46]. An unclear or high risk of bias in this study criteria was also found in eight of 15 studies where PIMs were assessed using polypharmacy [23, 39]. Selective reporting and other risk of bias were unclear in most studies. Due to the varied nature of study design, combined with differences in inclusion and exclusion criteria, it is not possible to compare the quality of the studies.
DISCUSSION
Main findings
To our knowledge, this is the first systematic review which quantifies and compares the prevalence of PIMs in older hospital patients with and without cognitive impairment. The findings suggest a higher prevalence of PIMs in some, but not all, studies where cognitive impairment was reported; however, these studies varied substantially between PIM measures.
Overall, there were important differences in polypharmacy exposure among inpatients with and without cognitive impairment, as well as between studies when cognitive status was not reported. In studies comprising of inpatients with cognitive impairment only, the minimum prevalence of polypharmacy was 53.2%, compared to 30.4% for studies containing inpatients without cognitive impairment. However, substantial variation was observed, and this may have arisen from the way in which polypharmacy was defined, along with the fact that multiple definitions were used to determine cognitive impairment when it was reported. Nevertheless, a higher PIM prevalence was present for those with cognitive impairment in two studies defining polypharmacy as the use of six or more regular medications [31, 35], and three studies defining polypharmacy as the use of five or more medications [19, 34]. These results suggest that people with cognitive impairment are more likely to be exposed to polypharmacy, regardless of the cut-off used to define polypharmacy. Additionally, for the three studies which defined cognitive impairment as being diagnosed with dementia only [19, 35], there was also a higher prevalence of PIMs within all studies when compared to PIM use in patients without dementia (56.7% to 83.7% versus 51.5% to 76.8%). While the use of multiple medications may be clinically appropriate in certain circumstances, polypharmacy has been associated with harm resulting from a multitude of factors, including drug-drug interactions and drug-disease interactions [7]. Therefore, the higher prevalence of polypharmacy among patients with dementia may have been a factor for admission to hospital. Since the majority of studies assessed polypharmacy exposure at the time of hospital admission, thereby reflecting potential ADEs that may be due to outpatient rather than inpatient PIM use, opportunities exist to develop strategies and interventions during hospital stay to rectify this problem, as well as those that target prescribing in primary health care.
In addition to multiple medication use, both explicit and implicit approaches to defining PIM use also resulted in variable findings. There was a higher prevalence of PIMs between studies when using STOPP over the Beers criteria, and this is consistent with previous research conducted in community-dwelling older people [12]. This study found a higher prevalence of PIMs in studies with cognitive impairment reported than in studies that did not report on cognitive status, particularly when employing STOPP criteria (39.3% to 88.5% versus 20.0% to 63.4%). This may be due to the large number of studies conducted in Europe (42.6% of included studies), where the STOPP criteria (developed in Ireland) has been shown to capture a greater number of PIMs when compared to the Beers criteria, which is more specific to North America (8.5% of included studies conducted here) [11]. Earlier versions of the Beers criteria are comprised of medications that are no longer commonly used, as opposed to STOPP, which also contains criteria to detect drug-drug interactions and drug duplication [11]. Different versions of explicit criteria may have led to variation in PIM prevalence, with later modifications and updates changing the scope of PIMs that may be captured. This may pose implications which could affect the reliability and generalizability of our results.
Regardless of the criteria implemented within studies, we found an association between PIM use and the proportion of participants with reported cognitive impairment for the three studies with the highest proportion of participants with impairment [28, 40, 41], suggesting that inpatients with these disorders may be more likely to be prescribed PIMs. Despite the implicit MAI tool used in only two studies, a higher score was also found in the study which reported 70.6% of participants with cognitive impairment [28], as opposed to the study which did not report cognitive status [66]. With regards to the most prevalent PIM prescribed, the high prevalence of benzodiazepines in this systematic review is consistent with another recent review assessing PIMs in community-dwelling older people with cognitive impairment and/or dementia [17]. While future interventions addressing PIM use should address those with greater risk of harm over clinical benefit, greater efforts should be undertaken to target the inappropriate use of benzodiazepines, particularly among inpatients with cognitive impairment.
Despite our findings aligning with previous research which demonstrates that older people living with dementia have a high prevalence of inappropriate drug use [70], the lack of consensus in relation to approach taken to define cognitive impairment makes it challenging to infer valid comparisons between studies. Only five of 19 studies solely defined cognitive impairment as the clinical diagnosis of dementia [19, 46], with other studies reporting delirium only [31, 45], impaired cognitive function determined by a Mini-Mental State Examination (MMSE) score below 24 [1, 43], or a combination of cognitive disorders [4, 44]. The criteria used for the diagnosis dementia, delirium and mild cognitive impairment also varied between studies and countries, and did not consistently use rigorous objective measures. These comparisons are further made difficult with the numerous explicit and implicit tools available to characterize PIMs.
Nevertheless, the high prevalence of PIMs when measured by polypharmacy, together with assessment by explicit or implicit tools, emphasizes the importance of monitoring multiple medication use in acute care. Current published evidence suggests a significant, yet highly variable, prevalence of PIM use in the residential long-term care setting, with a recent systematic review by Storms et al. [12] determining the prevalence of PIM use to range from 18.5% to 82.6% when using the Beers criteria, and 23.7% to 79.8% when utilizing STOPP criteria. Previous research has indicated that older people with dementia are at greater burden of PIMs within the UK community, whereby the prevalence of polypharmacy was as high as 57.2% and 40.4% in residents with (n = 10,528) and without dementia (n = 280,641), respectively [71]. Another cross-sectional study of 5406 nursing home residents with advanced dementia reported that 53.9% were using a medication with questionable benefit, according to a Delphi consensus list of PIMs [16].
The articles identified in this review used several versions of the Beers criteria, along with STOPP, to assess the prevalence of PIMs in older inpatients. However, many of these criteria fail to consider older people with dementia, delirium, and other cognitive disorders [13]. However, the updated Beers criteria of 2015 does provide an additional list of PIMs for dementia and delirium, with recommendations to avoid using all anticholinergic agents, H2-receptor antagonists, benzodiazepine and ‘Z-drugs’, as well as chronic or as-needed antipsychotics [10]. Only two studies employed the 2015 Beers criteria [23, 63]; however, one of these failed to document cognitive assessment and limited its study to individuals taking five or more medications [63]. On the other hand, Gutierrez-Valencia et al. found that 23.5% of PIMs were prescribed in the cohort admitted with dementia, delirium or other cognitive impairment [23]. Benzodiazepines were also the most prevalent PIM used across all hospital patients using the 2015 Beers criteria (39.5%). Therefore, an even higher prevalence of benzodiazepines may be seen when using the 2015 Beers criteria, in which any treatment is considered inappropriate while previous versions only identified particular benzodiazepines for certain durations [10]. Recent efforts have focused on identifying medications of questionable benefit in advanced dementia in nursing home residents [16]; however, limited evidence exists which characterizes PIM use in mild-moderate dementia and in the acute care setting.
Strengths and limitations
The major strength of this review was the rigorous nature of its systematic approach, with two independent reviewers determining each study’s eligibility, along with conducting data extraction. Studies were located from six databases, and each were evaluated for risk of bias using Cochrane quality assessment criteria. Many studies relied on the Beers and STOPP criteria, which are the most frequently used instruments to measure PIMs. Included studies were also carried out in hospitals across most continents.
However, this review had several limitations. First, while we employed a targeted online search strategy and manually checked reference lists to include all the relevant studies, only studies published in English from Embase, Medline, PsycINFO, International Pharmaceutical Abstracts, Scopus, and Informit over January 2007 to June 2017 were selected. Limiting the search strategy to studies consisting of all participants aged 65 years and over may have resulted in omitting relevant sub-analysis findings of comparisons between wider population age groups. Second, for the 10 studies using explicit and implicit criteria where cognitive status was reported, we were unable to compare the prevalence of PIMs within each individual study to determine whether participants with cognitive impairment were more likely to be prescribed PIMs. Instead, we could only form comparisons between studies when using these criteria. Third, these comparisons are further complicated by PIM use not being measured uniformly throughout this review, with its prevalence documented at numerous points, including at the time of hospital admission, during hospital stay, and at hospital discharge.
Lastly, we were unable to evaluate the overall quality of the included studies due to significant variation in study design, restricting the generalizability of our findings. In the 28 studies which did not report cognitive impairment, only seven studies addressed cognitive impairment in their inclusion and exclusion criteria [48, 54–57]. Psychogeriatric patients were excluded in three studies [49, 59], as were those who were mentally unstable or unable to provide informed consent due to severe cognitive impairment in an additional four studies [48, 55–57]. A study conducted by Tosato et al. [50] assessed cognitive status using a MMSE but did not report PIMs in terms of cognition. Therefore, inconsistencies with the inclusion and exclusion criteria of studies which did not report cognitive impairment remains a significant limitation of this review. While some studies that documented cognitive impairment may have been more likely to report higher PIM prevalence due to publication bias, inconsistencies in the quality of the study design render it difficult to form such a conclusion.
Implications for policy and research
Despite only 19/47 of the included articles consisting of a proportion of participants with cognitive impairment, our results do indicate important differences in the prevalence of PIMs among inpatients with and without cognitive impairment. Our findings also highlight the significance of reporting cognitive status in older people when admitted to the acute care setting, whereby some PIMs may be more prevalent or clinically relevant in people with cognitive impairment.
There is a significant need to evaluate the appropriateness of high-risk prescribing when older patients with any form of cognitive impairment are admitted to the acute care setting. The prevalence of dementia in hospital patients aged over 70 years has been previously documented to be as high as 29% to 42% [18]. Timmons et al. [72] has previously reported on the frequent nature of incorrectly assessing inpatients aged over 70 years, with inadequate assessment of cognition (43% of cases) and delirium (30% of cases). Whilst Parsons [13] acknowledges that more recent studies evaluating inappropriate medication use do in fact recruit older people with mild to moderate dementia, it is common for diagnosis of cases of dementia to be either delayed and/or undocumented [73]. Further research is warranted to determine the most useful tools for screening and diagnosing cognitive disorders, due to the international variation in health care systems and differences between wards.
Future policies should encourage the assembly of cognitive- and/or dementia-related registries to optimize the collection of epidemiological data for research, monitor the quality of care for individuals with cognitive disorders, and thus improve on medical care [74]. Registries may help evaluate and refine the diagnostic criteria for dementia and delirium, along with standardizing and validating screening instruments and diagnostic tools. Consequently, this may enhance the methodological quality of studies, improving the applicability of prevalence data for patients with cognitive impairment.
Moreover, frequent medication monitoring and assessment for PIMs should be encouraged in patients with cognitive impairment admitted to acute care. This review provides further evidence for the high prevalence of anticholinergic and sedative medications use in patients with cognitive impairment. Overuse of these medications have been associated with ADEs, some of which may limit cognitive and physical function [75]. Anticholinergic and sedative medications are commonly used to treat medical conditions which may occur in later stages of life, such as urinary incontinence, sleep and pain disorders, chronic obstructive pulmonary disease, and mental illnesses [75]. Regular assessment of PIMs, along with monitoring multiple medication use, may improve patient health outcomes, especially for those with cognitive disorders.
Conclusion
PIM use, when defined using polypharmacy and explicit or implicit tools, is highly prevalent among older inpatients. However, those with cognitive impairment (including dementia and delirium) were found to experience a higher prevalence of PIMs, as determined by a limited number of studies that reported cognitive status. As such, it is important that clinicians can recognize and review these medications to minimize adverse outcomes associated with use in the acute care setting. Due to the high variability of our findings, further studies using criteria specific to cognitive impaired inpatients are necessary to generate a better understanding of the prevalence of PIMs in people with dementia and delirium. Future studies of older adults in hospital should focus on the impact of PIM use on patient-centered outcomes to inform enhanced acute care services for people with cognitive impairment.
Footnotes
ACKNOWLEDGMENTS
DG is supported by the National Health and Medical Research Council (NHMRC) Dementia Leadership Fellowship. This review was supported by NSW Health Translational Research Grant Project 274 (2016-18), ‘Reducing inappropriate polypharmacy for older inpatients.’