
Abstract
Background:
Patients with Down syndrome (DS) often survive into adulthood. Relatively little information is currently available regarding hospitalization outcomes among mature, older adults with DS.
Objective:
To identify risk factors associated with hospital mortality rates and increased costs for hospitalized older adults with DS.
Methods:
Data on hospitalized older adults with DS (≥65 years) were identified from the Nationwide Inpatient Sample database (6) from 2002 through 2012. Multivariate analyses were performed to evaluate risk factors associated with hospital mortality and hospitalization cost in these patients.
Results:
A total of 2,134 older adults with DS were identified. A temporal increase over the 11-year period was observed in the number of older adults with DS who were hospitalized (trend p < 0.0001). However, the hospital mortality rate and post-hospital discharge to skilled nursing facilities have decreased during the same time period. Risk factors associated with increased hospital mortality included advanced age (70–79 years), female gender, admissions in the western United States, and presence of comorbid conditions (ischemic heart disease, Alzheimer’s disease, and cerebrovascular accident). The mean cost was $18,241 (SD $56,105) over the 11-year period. However, no significant temporal changes in costs were noted (trend p = 0.14).
Conclusions:
The number of hospitalized elderly Americans with DS has increased over the 11-year period. However, hospital mortality and discharge to skilled nursing facilities have decreased during the same time period. Several demographic and co-morbid factors are associated with increased mortality. No significant differences in temporal trends in costs were noted.
Keywords
INTRODUCTION
Down syndrome (DS) is the most commonly identifiable genetic cause of cognitive impairment, with a prevalence of approximately one in 733 live births [1]. Individuals with DS are at increased risk of mortality and adverse outcomes related to various co-morbidities, which include congenital heart disease, epilepsy, leukemia, and thyroid disorders, along with others [2–4].
Even though the life expectancy for individuals with DS has increased from 12 years in 1949 to nearly a median of 60 years of age today, it is still lower than that for the general population [5, 6]. Common causes of mortality among individuals with DS include leukemia, respiratory illness, congenital circulatory defects, diseases of the digestive system, dementia, and Alzheimer’s disease [3, 7]. Patients with DS have an earlier progression to Alzheimer’s disease as compared to the general population. The presence of Alzheimer’s disease as a co-morbid condition may also impact hospitalization among older patients with DS.
Much of the information on individuals with DS is still limited to childhood and younger adults [8]. Little is known about the outcomes following hospitalization of elderly adults with DS [9]. The frequency of Alzheimer’s disease among hospitalized patients with DS is not well investigated. Therefore, this study was undertaken with the objective to describe the temporal trend for hospitalization among older DS patients and in those with associated Alzheimer’s disease and to identify risk factors associated with hospital mortality and costs of hospitalization. Specifically, we wanted to investigate if Alzheimer’s disease was a factor associated with in-hospital mortality and cost of hospitalization.
METHODS
Data and sample
Retrospective data were pooled from the 2002 to 2012 Nationwide Inpatient Sample (NIS) databases (renamed as the National Inpatient Sample in 2012), sponsored by the Agency for Healthcare Research and Quality (AHRQ) as part of the Healthcare Cost and Utilization Project (HCUP). NIS is the largest publicly available all-payer inpatient care database in the United States, representing a 20% stratified sample of all US community hospitals [10]. A weighting variable provided by HCUP for trends and discharges was used to generate a national estimate [11]. Weighted frequencies are approximately five times the unweighted frequencies, because the NIS contains a 20% random sample from all hospitalizations in the US every year.
All patients aged 65 years or older who had an International Classification of Disease, 9th Revision, Clinical Modification diagnosis code indicating Down syndrome (ICD-9-CM: 758.0) were identified. Patients transferred to another short-term hospital were excluded in order to avoid double counting. The final study sample consisted of 2,134 records (unweighted sample), representing 10,144 discharges in the US (nationally weighted sample) from 2002 through 2012.
Outcomes
Outcome measures included in-hospital mortality and hospitalization associated costs. Costs were converted from the total charge variable in the NIS datasets using charge-to-cost ratios and were reported in 2014 US dollars using Consumer Price Index for hospital services.
The HCUP NIS contains data on total charges for each hospital discharge. This charge information represents the amount that hospitals billed for services, but does not reflect how much hospital services actually cost or the specific amounts that hospitals received in payment. The HCUP Cost-to-Charge Ratio Files are used to convert hospital charges to actual costs. For each data year, a Cost-to-Charge Ratio File was created based on all-payer inpatient cost for every hospital in the corresponding NIS database. Using the merged data elements from the Cost-to-Charge Ratio Files and the total charges reported in the NIS databases, we converted the hospital total charge data to cost estimates by multiplying total charges with the appropriate cost-to-charge ratio. Because the study sample contains data across 11 years, we reported costs data in 2014 US dollars using Consumer Price Index for hospital services [10].
Independent variables
Outcomes were adjusted for patient demographics (age, sex, and race/ethnicity), admission type (admitted from a long-term care facility and admission year), comorbidities, and hospital characteristics (size, rurality, teaching status, and region). Patients not admitted from long-term care facility may have been admitted from outpatient facilities, other acute care hospitals, or emergency departments. Age (in years) was transformed into four categories: 65–69, 70–74, 75–79, and 80 or older. Race/ethnicity was re-categorized into white, black, other race/ethnicity, and missing. Because some states do not report data on race/ethnicity, these data were not missing at random. Those discharges with missing race/ethnicity were assigned to a separate “missing” group. Admission year was grouped into three-year periods, except for the last two years. Comorbidities that are common for older patients with DS were included to adjust for patient risk factors. Hospital characteristics were obtained from the NIS hospital weights file.
Data analyses
Patient and hospital characteristics are presented as relative frequencies and percentages for each independent variable. T-statistics were calculated to analyze the overall trend of each independent variable during the study period. Trend p values were obtained using analysis of variance (ANOVA) with Bonferroni adjustments to analyze the differences among study variables across the 11 years. Univariate comparison between survivors and non-survivors was performed using t-test and Chi-square test. Multivariate logistic regression was conducted for in-hospital mortality. A generalized linear model with logit link and gamma distribution was fitted for right skewed cost data as a function of all the independent variables.
All statistical analyses were performed using SAS 9.4® (SAS Institute, Inc., Cary, NC, 2013). All tests of significance were two-sided; significant results were defined at p < 0.05. Approval to conduct the study as exempt from human subjects review was received from the Institutional Review Board at the University of Arkansas for Medical Sciences.
RESULTS
Hospitalizations trends
During the 11-year study period, the number of hospitalizations with a diagnosis of DS among older adults (≥65 at the time of admission) showed an upward trend, with an increase from 649 hospital discharges in 2002 to 1,300 hospital discharges in 2012 (Fig. 1A). This represents the weighted frequency (labeled on y-axis left hand side). The weighted frequency, represents an adjusted value to account for the entire US population, and is derived from the un-weighted frequency weighted frequency (labeled on -axis right hand side). This is in contrast to a relatively stable trend for individuals with DS across all age groups (Fig. 1B).
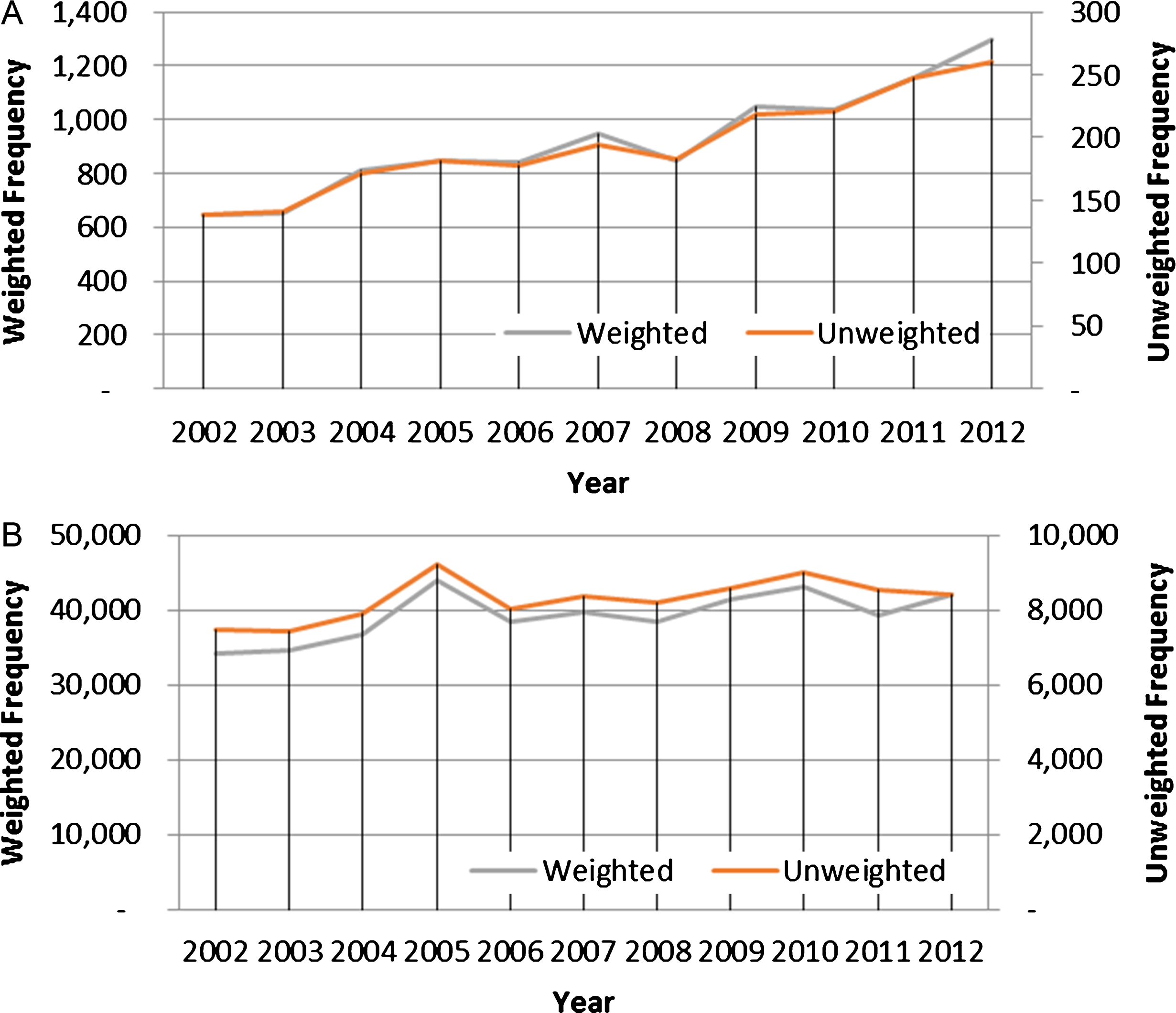
A) Number of hospitalizations with a diagnosis of Down syndrome for older adults (≥65), 2002–2012. B) Number of hospitalizations with a diagnosis of Down syndrome for all age groups, 2002–2012.
The three most common primary diagnoses for hospitalization among older adults with DS were aspiration pneumonitis, acute pneumonia, and septicemia. These diagnoses accounted for 40.6% of all hospitalizations (Table 1). Operations on the digestive system, operations on the cardiovascular system, and diagnostic and therapeutic procedures were the most common procedures performed and accounted for 74.0% of all procedures (Table 1).
Ten Most Common Primary Diagnoses and Procedures for Hospitalizations among Older Adults with Downs Syndrome, 2002–2012
Patient and hospital characteristics
Table 2 shows the patient and hospital characteristics of the hospitalizations for older adults with DS. Patients 65–69 years of age accounted for 69% of the overall study population and 11% were older than 75 years of age at the time of admission. Majority of patients with DS with Alzheimer’s disease (76.6%) hospitalized were in the 65–69 years age group compared to 67.7% for patients with DS without Alzheimer’s disease (p value 0.009) (Supplementary Tables 1 and 2). More than half of the older patients with DS received care in large hospitals and 79.3% were treated at urban hospitals (including teaching and non-teaching).
Patient and hospital characteristics of hospitalizations for older adults with downs syndrome, 2002–2012
LTC, long-term care facility; COPD, chronic obstructive pulmonary diseases. Categorical data represented as frequency (%). †p values less than 0.0015 were deemed significant, after Bonferroni adjustment.
A significant increase (based on trend p values) in hospitalization was observed in Southern states over the study period (from 19.7% in 2002 to 34.2% in 2012). The Midwest had a significant downward trend, from 30% in 2002 to 21.5% in 2012. Among comorbid conditions for older adults with DS, an overall upward trend was observed for hypothyroidism, mental disorders (including dementia), and hypertension, diabetes, and ear disorders. Hypothyroidism was the most common comorbidity (40%) among hospitalization diagnoses for DS patients.
Hospital mortality and costs
Table 3 depicts the outcomes of hospitalized older patents with DS. Hospital mortality rates and discharge disposition of older patients with DS to skilled nursing facilities have decreased significantly over the 11-year period while home discharges increased. However, no significant difference in temporal trends in cost of hospitalization was noted over the study period. The cost of hospitalization (overall and for top 5 primary diagnoses for hospitalization) for patients with DS with Alzheimer’s disease was significantly lower compared to patients with DS without Alzheimer’s disease (Supplementary Table 3).
Outcomes of older patients with DS, 2002–2012
SNF, Skilled nursing facility; *in 2014 US$; **denominator for calculating percentages is the total hospitalized elderly DS patients in each year.
Table 4 depicts the risk factors associated with hospital mortality and costs of hospitalization among older adults with DS. Significant risk factors associated with increased mortality during hospitalization included age 70–79 years at the time of admission [AOR1.42 (1.20–1.68) for age 70–74 years] and AOR 1.40 (1.07–1.84) for age range 75–79 years], female gender [AOR 1.20 (1.04–1.38)], patients in Western US region [AOR 1.45 (1.17–1.80)]; presence of ischemic heart disease [AOR 1.96 (1.59–2.42)], Alzheimer’s disease [AOR 1.52 (1.25–1.85)], cerebrovascular disease [AOR 1.73 (1.33–2.24)], and earlier era hospitalization (2002–2004). In contrast, presence of hypothyroidism, hypertension, eye and ear diseases were associated with lower mortality during hospitalizations. Among hospital characteristics, patients hospitalized to large urban hospitals compared to rural hospital [AOR 0.74 (0.62–0.89) and 0.56 (0.46–0.68) for urban non-teaching and urban teaching hospitals, respectively], in the Midwest region [AOR 0.79 (0.64–0.98)] had lower mortality rates.
Factors associated with in-hospital mortality and costs in older adults with downs syndrome, 2002–2012
LTC, long-term care facility; COPD, chronic obstructive pulmonary disease.
Risk factors significantly associated with hospitalization costs included black race, medium and large hospitals, location in Western region, presence of comorbid chronic obstructive pulmonary diseases (COPD), and admission between 2005 and 2007. Meanwhile, female gender, Midwest and South locations, the presence of Alzheimer’s disease and cognitive disorders, and comorbid eye diseases were associated with lower hospitalization costs. Specifically, the mean cost of hospitalization for patients with DS and Alzheimer’s disease was $15,972.6 (SD: $38,272.2) per hospitalization compared to $18,621.85 (SD: $58,486.1) for patients with DS without AD. Supplementary Table 3 provides details of average cost of hospitalization for older patients with DS and AD compared to those without AD.
Supplementary Table 4 provides a univariable comparison of survivors and non-survivors. Care in urban teaching hospitals, and co-morbidities such as hypertension and hypothyroidism were more frequently noted in survivors compared to non-survivors, whereas stroke and ischemic heart disease was noted more frequently in non-survivors compared to survivors. However, after Bonferroni adjustments none of the comparisons were statistically significant.
DISCUSSION
To our knowledge, this report is the largest cohort study to date to evaluate temporal trends, risk factors for in-hospital mortality, and hospitalization costs among older adults with DS.
In contrast to stable hospitalization trends among patients with DS, the number of hospitalizations among the subgroup of older adults with DS has more than doubled during the 11-year study period. The increase in hospitalization frequency in older adults with DS may reflect improved life expectancy among adults with DS [5] related to improved health care in recent eras. This is also reflected with the temporal trends for decrease in hospital mortality and reduced transfer to skilled nursing facilities upon hospital discharge for older patients with DS. However, with the increase in home discharge a possibility which cannot be ruled out is that older adults with DS were discharged home with the caregiver due to their inability to participate in therapy involved in skilled nursing facility or were changed to palliative care status with home discharge.
Ischemic heart disease was one of the risk factors associated with in-hospital mortality in our study. Previously, Hill and colleagues [7], using a hospital discharge data from Sweden and Denmark have similarly shown a four-fold increase in mortality attributable to ischemic heart disease among patients with DS [7]. Yang and colleagues [12], in contrast, observed a lower standardized mortality odds ratio for deaths related to ischemic heart disease among adults greater than 40 years of age. These differences may be related to the type of study population investigated, as our study only includes hospitalized patients with DS in contrast to a population-based sample by Yang et al. It is possible that patients presenting with chest pain symptoms related to ischemic heart disease are more likely to be hospitalized and thus represents a self-selected sub-population and thus is noted as a risk factor for mortality in our study. Interestingly, the presence of congenital heart disease was not a risk factor for in-hospital mortality among older individuals with DS in our study. This may indicate a selection bias in this study as patients with DS with associated congenital heart disease present early in life and may not survive to old age and thus were under-represented in this cohort. These results are similar to those reported by other investigators in population studies [13, 14]. Zhu and colleagues [13], in a population-based study from Denmark, identified congenital heart disease as the main cause of death in those below 20 years of age and acquired diseases of the circulatory system are one of the main reasons for death in those who died after 20 years of age.
Concomitant Alzheimer’s disease was another risk factor associated with increased in-hospital mortality. These results are similar to those indicated by other investigators [3, 15]. Hill and colleagues have noted a 54-fold increase in mortality attributable to Alzheimer’s disease [7]. The mean age for diagnosis of Alzheimer’s disease was 55.8 years with a median survival time after diagnosis of only 3.8 years with death occurring at a median age of about 60 years in individuals with DS [16]. Age at diagnosis of Alzheimer’s disease and treatment status remained predictive of survival time following diagnosis. This also explains why older age >70 years is also an independent risk factor for in-hospital mortality as the incidence of dementia increases to approximately 80% by 65 years of age [15]. Mechanistically, the accumulation of amyloid A4 precursor protein begins to occur at a much younger age in patients with DS compared to the non-DS populations [17] and is also associated with increased rates of epilepsy and seizures [7, 16] which may trigger hospitalization in patients with Alzheimer’s disease.
The trend in hospitalized older patients with DS with comorbid cerebrovascular disease has not changed significantly over time. However, comorbid cerebrovascular disease among older DS patients was associated with a significant higher risk of in-hospital mortality. These results are similar to the report by other investigators [7, 18]. Sobey and colleagues, noted among hospitalized individuals with DS in Australia [18] that DS was associated with a greater risk of cerebrovascular events (ischemic as well as atherosclerotic) especially among females. The association between DS and ischemic stroke appeared to be explained largely by cardioembolic risk.
Gender differences for in-hospital mortality, observed in our study, has also been previously described in population-based studies [3, 19]. Contrary to the general population, where females have a longer life expectancy compared to men, male patients with DS outlive their women counterparts. This is still speculative, as it has not been fully replicated by other investigators [6, 14]. This increase in mortality and shorter life span in women with DS, if valid, may in part be related to the onset of early menopause among women with DS.
Our study found that the proportions of DS patients with comorbid hypertension, COPD, or diabetes were comparable to that observed in the general population [2]. However, other common conditions in older DS patients, such as thyroid dysfunction, cognitive disorders, congenital vision and hearing impairment were less common in the general versus DS populations. Thus, despite an increase in life expectancy and decreasing hospital mortality as the life expectancy of individuals with DS has increased, there is a continued need to provide specialized health care that addresses the unique issues that exist in older patients with DS.
Higher hospitalization costs were noted in older adults with DS, for care provided in medium and large sized hospital compared to small hospitals, and in patients with COPD. Hung and colleagues, in a study from Taiwan, have evaluated cost of hospitalization and length of hospital stay in patients with DS [9]. Patients with DS had double the length of stay and nearly three times the cost of hospitalization compared to the general population. The average hospital length of stay in older patients with DS was 6.7 days in our study compared to 22.3 days in Taiwan. However, the comparison to our study may not be fully valid. This is due to differences in healthcare systems, and the patient mix. The majority of the patients included were younger adults who have a different set of comorbid conditions and functionality as compared to their older counterparts in our study.
A majority of the older adults with DS have received care at larger and urban hospitals. It is possible that this could indicate that patients with DS who have more complicated health care needs may be accessing larger hospital where they are more likely to receive more comprehensive care. However, the lower proportion of DS patient hospitalization in smaller rural hospitals compared to urban hospital could indicate a potential disparity in access to healthcare in rural areas for these individuals. Moreover, it has been previously highlighted that individuals with intellectual disabilities experience health disparities compared to individuals within the general population [20–22]. These disparities may confer a higher mortality, morbidity, lower quality of life, and may adversely impact access to health care services for those with intellectual disabilities.
Limitations
There are several limitations in the current study. First, the NIS database is an administrative database. Like most electronic databases, NIS lacks detailed information on laboratory, pathology, imaging, and patient severity (like degree of individual’s cognitive capacity). These missing confounders might affect outcome comparisons. The diagnosis of Alzheimer’s disease in individuals is not standardized and thus subject to variations. Finally, the NIS database is compiled from hospital discharge data and does not have any outpatient follow-up data for mortality beyond the hospitalization. The NIS is an administrative database that aims to gather data for billing purposes and can be limited by erroneous coding. However, the Healthcare Cost and Utilization Project quality control measures should minimize these possibilities. Furthermore, the hard clinical end-points used in our analysis are more difficult to miscode. Nevertheless, the potential for unmeasured confounders that may bias the outcomes still exist.
In summary, despite increasing life expectancy, and growing numbers of hospitalized elderly Americans with DS, there is a trend of decreasing hospital mortality and discharge disposition to skilled nursing facilities among individuals with DS, from 2002 through 2012. The present study highlights the continuing need for allied healthcare workers to be aware of the complex medical needs of older patients with DS. It is plausible that care goal discussions earlier on in treatment may reduce hospitalizations among some of these patients. Future studies will be of interest.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/17-1067r3).