
Abstract
Background:
Greater physical fitness is associated with reduced rates of cognitive decline in older people; however, the mechanisms by which this occurs are still unclear. One potential mechanism is aortic stiffness, with increased stiffness resulting in higher pulsatile pressures reaching the brain and possibly causing progressive micro-damage. There is limited evidence that those who regularly exercise may have lower aortic stiffness.
Objective:
To investigate whether greater fitness and lower aortic stiffness predict better cognitive performance in older people and, if so, whether aortic stiffness mediates the relationship between fitness and cognition.
Methods:
Residents of independent living facilities, aged 60–90, participated in the study (N = 102). Primary measures included a computerized cognitive assessment battery, pulse wave velocity analysis to measure aortic stiffness, and the Six-Minute Walk test to assess fitness. Based on hierarchical regression analyses, structural equation modelling was used to test the mediation hypothesis.
Results:
Both fitness and aortic stiffness independently predicted Spatial Working Memory (SWM) performance, however no mediating relationship was found. Additionally, the derived structural equation model shows that, in conjunction with BMI and sex, fitness and aortic stiffness explain 33% of the overall variation in SWM, with age no longer directly predicting any variation.
Conclusions:
Greater fitness and lower aortic stiffness both independently predict better SWM in older people. The strong effect of age on cognitive performance is totally mediated by fitness and aortic stiffness. This suggests that addressing both physical fitness and aortic stiffness may be important to reduce the rate of age associated cognitive decline.
INTRODUCTION
People over the age of 65 are now the fastest growing demographic globally, with a recent United Nations report estimating a doubling of this older population to over two billion by the middle of the twenty-first century [1]. This rapid rise will subsequently lead to an associated rise in age-related cognitive decline and dementias, such as Alzheimer’s disease (AD). While an apparently inevitable aspect of aging, the rate of cognitive decline varies considerably between individuals, which has been attributed in part to modifiable risk factors such as lifestyle. It is estimated that reducing cognitive ageing so as to delay the onset of dementia by even 1 year could reduce the prevalence of dementia by more than 11% [2]. Given the wide-ranging personal and societal burdens associated with age-related cognitive impairment [3], it is imperative that potential interventions that may assist in reducing the rate of cognitive aging are investigated and understood.
The extant literature indicates that physical activity and fitness are positively associated with cognitive performance [4–7] and reduced risk for dementia [8–11]. Specifically, a number of large population-attributable risk (PAR) studies have found that, across the Western world, physical inactivity and associated low levels of physical fitness are associated with a larger proportion of dementia cases than any other lifestyle factor, including obesity, smoking, diabetes mellitus, midlife hypertension and depression [12, 13]. However, the mechanisms that underlie this relationship between physical fitness and the trajectory of cognitive aging are still unclear [14–16].
There are numerous mechanisms proposed to underlie the relationship between physical fitness and age-associated cognitive decline. These include inflammation, insulin regulation, stress resilience and changes to neurogenesis [16]. One other proposed mechanism is increased stiffness of the large central arteries. Arterial stiffness, or the reduced compliance/elasticity of the arteries, is proposed to affect the brain through a reduction in the ability of the large cardio-thoracic arteries, primarily the aorta, to buffer the peak pressure from the heart [17]. The brain is particularly vulnerable to higher pulsatile pressures, as it requires continuous high flow perfusion, which is facilitated by the lack of the more robust intermediate arterial systems afforded to other organs. It has been proposed that the prolonged higher peak pressures projected by stiffer central arteries may lead to small vessel damage and micro-bleeds [18, 19]. This damage to the cerebral microvasculature may contribute to neuronal loss and an associated decline in cognitive function [20–22]. Aortic stiffness, particularly as assessed with pulse wave velocity, is suggested to be an early marker of broader vascular health issues [23, 24], with central arterial degradation potentially negatively influencing cognitive performance before peripheral aspects of vascular health issues are evident, such as those assessed by standard brachial blood pressure tests [25]. This therefore makes aortic stiffness an important potential target for the reduction of vascular influences on cognitive decline and dementia prevention.
While there is a clear effect of aging on the major central elastic arteries, research has demonstrated that those who engage in regular exercise behavior tend to have lower arterial stiffness for their age [26]. This effect is possibly due to a reduction in the overall accumulated number of cardiac cycles and degree of pulsatile stress affecting these arteries [27]. However, to date, research in this area is still far from conclusive, with some studies finding that certain forms of exercise, particularly resistance exercise, may in fact increase arterial stiffness [28, 29] (although these studies were predominantly in young and middle-aged adults). A recent study involving healthy older participants found that cognition (i.e., executive function), aortic elasticity and fitness all declined with age [30]. Furthermore, the study found that increased aortic stiffness and reduced fitness were both directly correlated with poorer cognitive performance in older people. However, they were unable to demonstrate that aortic stiffness mediated the relationship between fitness and cognitive performance, possibly due to the assessment of only a single cognitive domain and the inclusion of a particularly healthy older cohort.
The current study examined the effect of physical fitness on cognitive function in older, cognitively intact individuals. Participants were living in self-care accommodation in retirement communities, where there is a focus on maintaining independence, maintaining cognitive faculties, and delaying any requirement for moving to supported levels of care. The aim of this study was to examine the relationships between physical fitness, arterial stiffness and cognitive function in older people. We hypothesized that both greater physical fitness and lower aortic stiffness would predict better cognitive function in older people. Furthermore, this study aimed to investigate whether arterial stiffness mediated the relationship between fitness and cognition in healthy older people and whether the relationship between age and cognition was partially mediated by arterial stiffness and fitness, as illustrated in the conceptual (theoretical) model outlined in Fig. 1.
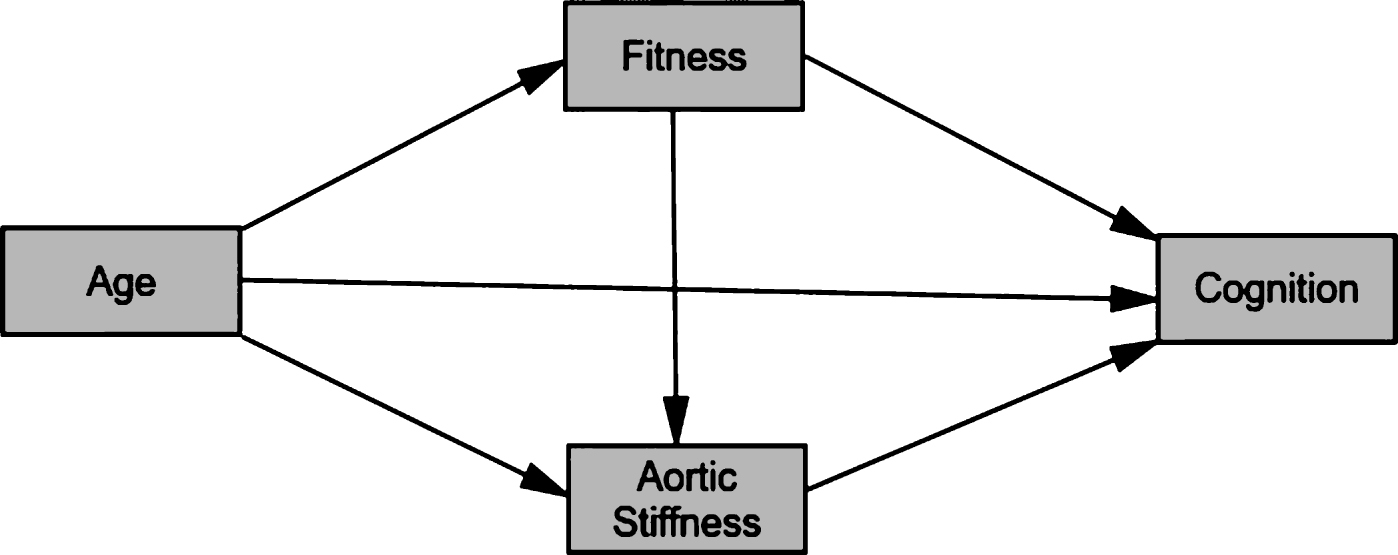
Conceptual model of the relationships between age, fitness, aortic stiffness, and cognition.
METHODS
This study examined the cross-sectional association between physical fitness, arterial stiffness and cognitive performance. These relationships were explored using baseline data from the Lifestyle Intervention in Independent Living Aged Care (LIILAC) clinical trial [31].
Residents living independently in aged care communities, aged between 60 and 90 years, were recruited across 15 sites in and around Melbourne, Australia, as part of the LIILAC trial [31]. One hundred and two participants (73 females and 29 males) were recruited for the LIILAC trial, all of whom were able to live independently, without the need for outside support for their daily living activities. This study involved all LIILAC trial participants.
Those with any uncorrected visual impairment that hindered their reading, with significant psychological or neurological disorders, suspected cognitive impairment (scoring <24 on the MMSE) or significant levels of depressive symptoms (scoring >9 on the Geriatric Depression Scale) were excluded from the study. Participation was predicated on the ability to read and speak fluent English, and the ability to walk independently and safely. Additionally, prospective participants were not eligible if taking illicit drugs or cognitive enhancing medication. However, to properly reflect the aging population, use of other prescribed medications was not an exclusion, as long as the dose had been stable for at least six months.
This study was approved by the Swinburne University Human Research Ethics Committee (project number 2013/057), and all participants provided informed consent that was counter-signed by their general practitioner, confirming that they were medically fit to participate in the LIILAC trial. The trial was also registered with the Australian New Zealand Clinical Trials Registry - ACTRN12614001133628. All procedures were conducted in accordance with the Declaration of Helsinki (as revised in 2004).
Fitness assessment
Fitness was assessed with the Six-Minute Walk test (6 MW), which involved participants walking back and forth between two markers placed 10 m apart on an unimpeded level surface. Participants were encouraged to walk as far as possible in six minutes, with the total distance recorded [32]. Multiple studies have demonstrated that this test is a simple, but reliable means of assessing physical fitness/functional capacity, particularly in cohorts with potential limitations [33, 34]. Only participants who completed the full six minutes were included in the analysis.
Arterial stiffness assessment
Carotid-femoral pulse wave velocity (CFPWV) was derived using a femoral cuff to capture the femoral waveform and tonometer (pressure sensor) captured the carotid waveform. CFPWV was then calculated as the distance between the carotid and femoral measurement sites divided by the transit time. This method is well validated [35], and is considered the gold standard of assessment of central arterial stiffness [36].
Peripheral and central blood pressures, as well as measures of arterial stiffness were assessed using applanation tonometry with the SphygmoCor ® device (Model XCEL, AtCor Medical, Sydney, Australia). Following a 5-minute rest period in a supine position, standard brachial blood pressure was measured using a brachial blood pressure cuff on the left. Three recordings were made, with the first being discarded and the average taken of the second and third recordings. Aortic blood pressures, augmentation pressure (AP) and augmentation index (AIx) were also analyzed by the device using a mathematical transfer function to derive the aortic waveform. The AP was calculated as the difference between the first and second systolic peak, with the AIx calculated as the percentage contribution that the AP makes to the overall pulse pressure (PP). AIx and AP, considered to be surrogate measures of peripheral arterial stiffness, were included in the variable set, as were the standard blood pressure measurements, given that there is extensive literature linking these measures with cognition [37].
Cognitive assessment
Cognitive performance was assessed using the Swinburne University Computerised Cognitive Assessment Battery (SUCCAB). The SUCCAB is a well-validated computerized test battery utilizing tests of cognition that are sensitive to age-associated cognitive decline [38]. The battery comprised eight tests, each preceded by a brief practice task to familiarise the participant with the procedure and task requirements. The tests were administered in the following order: Simple Reaction Time (SRT), Choice Reaction Time (CRT), Immediate Recognition (IRec), Congruent Stroop (CStrp), Incongruent Stroop (IStrp), Spatial Working Memory (SWM), Contextual Memory (CMem), and Delayed Recognition (DRec). The tasks were participant paced, with no maximum time to respond. Participants were instructed to respond as quickly and as accurately as possible. More detailed descriptions of the component tasks of the SUCCAB and their application are available [38–41].
Testing was undertaken onsite at the community facilities. Stimulus presentation was via a 23– inch monitor attached to a laptop, to ensure clear task visibility. Pre-testing validation found no differences in stimulus presentation time between the native laptop screen and the external monitor. All participant responses were via a 4-button response box. The SUCCAB took approximately 30 minutes to complete.
Percentage accuracy and the mean response-time to correctly performed trials were calculated for each task. The percentage accuracy was divided by the mean response time to give an overall performance score. Higher performance scores indicated faster reaction times and/or a greater trial accuracy. This ratio also assisted in accounting for the issue of the speed for accuracy trade-off prevalent in the cognitive assessment of older individuals [42–44]. As has been done previously with the SUCCAB [45], cognitive task performances from each of the eight tests were mapped into four broader cognitive ability domains, Reaction and Decision Speed (RDS), Cognitive Processing (CogP), Short Term Memory (STM) and Visual Processing (VisP), based on the Cattell-Horn-Carroll Broad Abilities model [46]. Since the STM domain is represented with just one cognitive task from the SUCCAB battery, namely SWM, this domain will be referred as SWM for clarity and accuracy of interpretation. Overall, this mapping into four cognitive domains enables a more standardized approach to the cognitive data analysis and reduced the chance of type 1 error.
Each performance variable was converted to a Z score to ensure each variable contributed equal weighting to the applicable domain ability score. The resultant cognitive ability domain scores were calculated as follows:
Reaction and Decision Speed (RDS)
(Z_SRT Performance + Z_CRT_Performance)/2
Cognitive Processing (CogP)
Z_(IStrp_Performance – Cstrp_Performance)
Spatial Working Memory (SWM)
Z_SWM_Performance
Visual Processing (VisP)
(Z_IRec_Performance + Z_DRec_Performance + Z_CMem_Performance)/3
Statistical analysis
Data analyses were conducted using IBM SPSS Statistics 24 and IBM SPSS Amos 24. Prior to analysis, the dependent cognitive variables were screened for normality and for outliers, with outliers being defined as lying further than 2.2 times the interquartile range below quartile 1 or above quartile 3 [47, 48]. Only RDS was found to have a univariate outlier, which was removed from further analysis. Additionally, CogP was found to have mild standardized negative skewness of 0.765. However it was decided that, in order to maintain consistency of interpretation with the other cognitive variables, not to transform this variable because regression analyses are fairly robust to this violation [49]. Multivariate outliers were identified using Mahalanobis Distances and were removed from analysis. Plots of the residuals obtained from the regression analyses described below (e.g., QQ-plots and predicted value plots) suggested that the regression assumptions of normality and homoscedasticity were supported.
Regression analyses were conducted to describe the relationship of cognition with fitness and arterial stiffness, independently and together, while controlling for the effects of age, sex and education. Based on the regression analyses, structural equation modelling was then used to test for significant mediation relationships. Goodness of fit statistics used for the structural equation modelling included the chi-square statistic, the normed chi-square and the root mean square error of approximation (RMSEA). As recommended by Hu and Bentler [50], adequate model fit requires RMSEA <0.06 and normed chi-square between 1 and 2.
RESULTS
Means and standard deviations for the demographic, cardiovascular and exercise variables/measures are presented in Table 1. Cognitive performance and the derived cognitive domain performance means and standard deviations are shown in Table 2.
Demographic, cardiovascular, and exercise characteristics
Mean (SD) reported. MMSE, Mini-Mental State Examination; BMI, body mass index; SBP, brachial systolic blood pressure; DBP, diastolic blood pressure; PP, brachial pulse pressure; AP, augmented pressure; AI, augmented index; CFPWV, carotid-femoral pulse wave velocity; 6MW, six-minute walk test.
Cognitive characteristics of study sample
Mean (SD) reported.
Initial analysis examined the associations of both the exercise and cardiovascular measures with each cognitive domain score. However, as age, sex and education are known to be significant predictors of cognition, each relationship was adjusted for these factors in the hierarchical regression analyses. The regression coefficient and standard error for each analysis are shown in Table 3.
Association of exercise and cardiovascular measures with cognitive domain performance – standardized weights
Model adjusted for age, sex, and education. 6MW, six-minute walk test; SBP, brachial systolic blood pressure; DBP, diastolic blood pressure; PP, brachial pulse pressure; AP, augmented pressure; AI, augmented index; CFPWV, carotid-femoral pulse wave velocity. ∧p < 0.05, *p≤0.01.
As can be seen in Table 3, higher 6 MW distance significantly predicted better Spatial Working Memory (SWM) after age, sex, and education were taken into account. The hierarchical regression model analysis revealed that, in total, the predictor variables explained 27% of the variance in SWM (F (4,94) = 8.55, p < 0.001). 6 MW significantly predicted 6% additional variance in SWM over and above that explained by age, sex and education (F change (1,94) = 7.08, p = 0.009), with greater distance walked predicting better SWM performance.
Additionally, lower CFPWV also significantly predicted better SWM performance, after controlling for the effects of age, sex and education. The hierarchical regression model analysis revealed that, in total, the predictor variables explained 25% of the variance in SWM (F (4,92) = 7.70, p < 0.001). CFPWV significantly predicted 6% additional variance in SWM over and above that predicted by age, sex and education alone (F change (1,92) = 7.13, p = 0.009), with higher pulse wave velocity predicting poorer SWM performance.
Similar, results were also found for diastolic blood pressure (DBP). The hierarchical regression model analysis revealed that, in total, the predictor variables explained 24% of the variance in SWM (F (4,96) = 8.63, p < 0.001). DBP significantly predicted 3% additional variance in Spatial Working Memory over and above that predicted by age, sex and education alone (F change (1,95) = 4.11, p = 0.046), with higher DBP predicting poorer SWM performance.
The model, as displayed in Fig. 2, was developed to explore these relationships with SWM as well as the contributing effects of age and sex; education was not included as it did not correlate with cognitive outcomes at any stage of analysis. BMI was also added to the model, given its known strong relationship with fitness and exercise. The model showed a good fit, χ2 (7) = 7.14, p = 0.41, normed chi-square = 1.020, and RMSEA = 0.014.
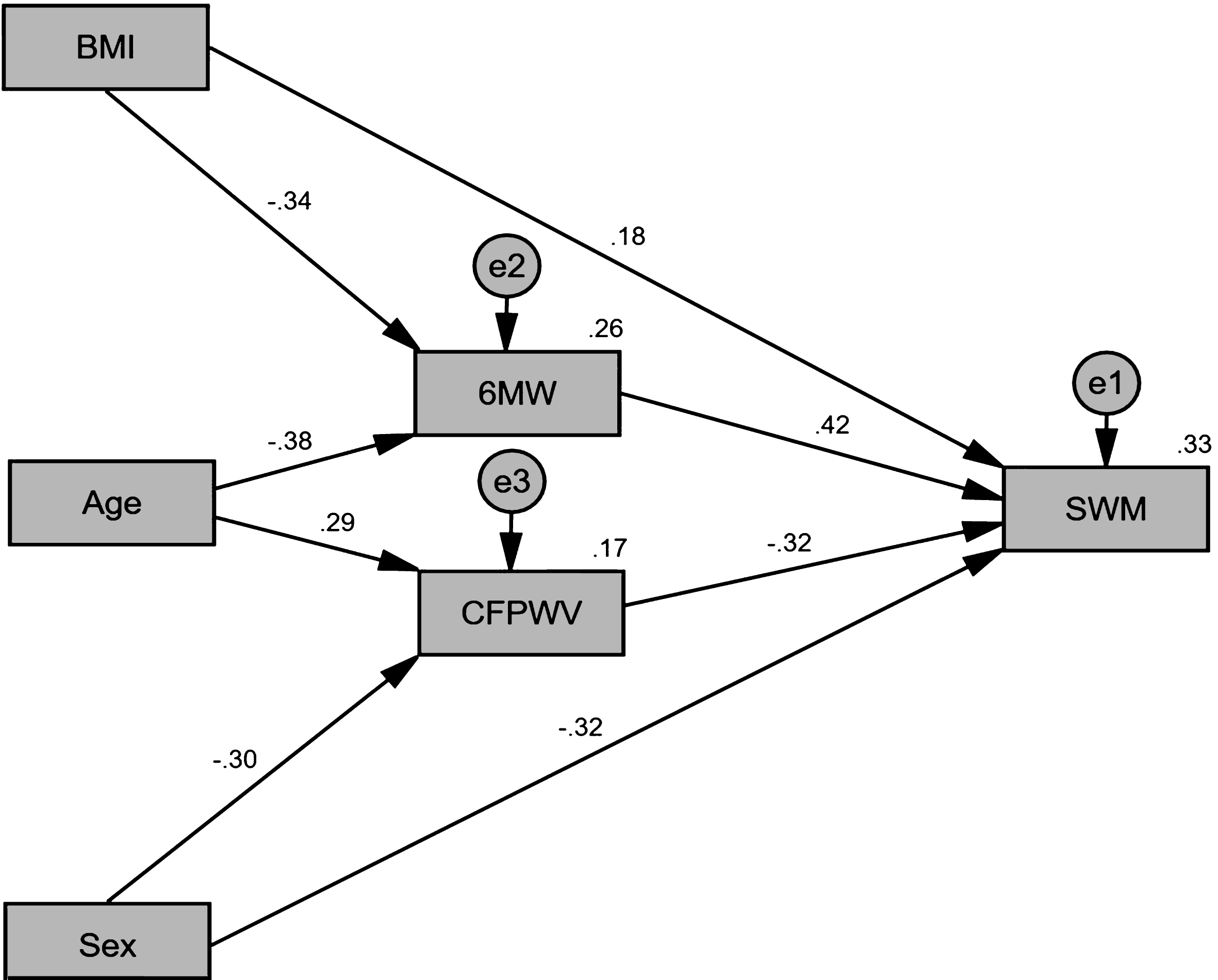
Final model for the physical fitness and arterial stiffness contribution to the variability in SWM. Standardized regression coefficients (β) are shown for each path and the percentage of variation explained is shown for each dependant variable. BMI, body mass index; 6MW, six-minute walk test; CFPWV, carotid-femoral pulse wave velocity; SWM, spatial working memory.
This model explains 33% of the variation in SWM. Contrary to expectation, adding a link from 6 MW to CFPWV produced no significant improvement in model fit (χ2 (1) = 1.25, p = 0.264), indicating that CFPWV does not mediate the relationship between 6 MW and CFPWV when age, BMI and sex are controlled. This model suggests the effect of BMI on SWM is partially mediated by 6 MW, the effect of sex on SWM is partially mediated by CFPWV, and the effect of age is completely mediated by 6 MW and CFPWV. This last result was confirmed when adding a direct link from age to SWM produced a non-significant improvement in the model fit (χ2 (1) = 1.37, p = 242). DBP was not included as it did not significantly contribute to SWM in the model.
Standardized direct, indirect and total effect sizes for the model are shown in Table 4. Both 6 MW and CFPWV have a large direct effect on SWM, with the effect of the 6 MW being 33% stronger than that of CFPWV.
Standardized effect sizes from Fig. 2
6MW, six-minute walk test distance; CFPWV, carotid-femoral pulse wave velocity; BMI, body mass index.
DISCUSSION
This study investigated the effects of both physical fitness and arterial stiffness on cognition in cognitively intact older adults. In partial support of the hypothesis, both higher fitness and lower central arterial stiffness significantly explained better SWM performance, and these relationships remained significant once the effects of age, sex, and BMI were adjusted for. However, no such relationships were found for the other measures of cognition. Contrary to expectations, there was no direct relationship between fitness and central arterial stiffness, with both predicting cognitive performance independently. The non-significant direct effect of age on cognition and the significant indirect effect size (– 0.254) for the relationship between age and cognition suggests full mediation of this relationship by fitness and CFPWV, and a possible mechanism/process for the relationship between age and cognition. This means that the reduction in SWM performance with increasing age, in this cohort of older people, may be fully explained by a combination of reduction in physical fitness and poorer health of the central thoracic arteries, that commonly occur over time.
These results are partially in line with the results of the study by Tarumi et al. [51] investigating the differences between endurance trained and sedentary middle-aged adults. Specifically, they also found that fitter older adults had better cognitive performance, as did those with lower arterial stiffness. Conversely, their study found a negative relationship between fitness and arterial stiffness, which was not supported by our findings. However, it should be noted that Tarumi and colleagues looked at highly fit middle-aged adults (aged 51–53), as opposed to older adults, in their endurance trained group, and they excluded participants with a broader range of medication use and health issues than our study. The lack of a direct relationship between fitness and arterial stiffness in older adults is supported by other studies [52, 53], however these studies did not examine cognition.
The SWM task is the measure in the SUCCAB cognitive battery that has consistently shown the greatest sensitivity to age-associated cognitive decline [37, 38] and following intervention [40, 45]. This sensitivity may well explain the specific findings for this cognitive domain in this study. Similar studies with larger sample sizes would be required to establish whether the cognitive relationships of fitness and central arterial stiffness are domain specific to SWM, or whether a broader range of cognitive processes are involved. The study is also limited by the cross-sectional nature of the data. Current fitness, particularly in older people, does not necessarily reflect a history of fitness across the lifespan. It is probable that the lower stiffness of the central arterial system is at least partially the product of fitness and exercise over a longer term, rather than at a singular time point [16, 54].
The findings from this study support the well-established contention that a focus on maintenance and, where possible, improvement of fitness is an important factor when attempting to ameliorate the rate of cognitive decline in older people. However, the results also indicate that it may be of similar importance for practitioners to investigate the stiffness of an individual’s central thoracic arteries. Given the recent advances in comparatively low-cost, non-invasive measurement techniques, consideration should be given to including assessment of aortic health as a central part of health focused interventions to reduce cognitive decline trajectories in older people. While fitness had no direct effect on aortic health in this study, pharmacological treatments have been found to reduce aortic stiffness beyond the effects of blood pressure mitigation [55], and could potentially play a role in a multi-faceted approach to cognitive preservation.
Strengths of this study include the use of older people residing in similar independent living aged care environments. This consequently reduced the potential influence of social isolation and environmental living conditions which may also impact cognitive trajectory. Furthermore, all testing of participants was conducted at their facility of residence, enabling more people to participate in the study. In particular, this meant that participants who are traditionally omitted from laboratory-based studies, such as those who are unwilling or unable to travel, were recruited, resulting in a sample more representative of independent living retirement village community. Additionally, participants were not excluded from the study on the basis of their medication, so long as the medication dosage was stable for at least six months. The majority of older adults in developed countries take some form of prescription medication [56–58]; this study therefore reflects a more typical aging population, and indicates that a focus on physical fitness for cognitive health in older people may be an important adjunct to pharmacological interventions.
The structural model derived from this study explains a third of the variation in performance in SWM in older people. This model provides a platform for future research in the area of cognitive aging, and future studies should be conducted to supplement and refine the model. In particular, other potential mediators of the relationship between fitness and cognitive ageing should be investigated, such as insulin sensitivity, stress, neurogenesis, and inflammation [16]. Further studies in this area would also benefit from a greater sample size, to determine whether other cognitive domains are also influenced by fitness and central arterial stiffness. Additionally, longitudinal studies in this area are recommended to examine the effects that changes in fitness will have on cognitive performance in this age group.
This study demonstrated that both higher fitness (measured with the 6 MW) and lower central arterial stiffness (measured with CFPWV) predict better spatial working memory in older people. Importantly, in combination these two factors completely mediate the effect of age. The effect of age on short term memory performance can be explained by the reduction of physical fitness and increasing central arterial stiffness associated with increasing age in older people. This provides a potential physiological explanation for the reduction in cognitive performance commonly observed with increasing chronological age. Additionally, we have elucidated that central arterial stiffness appears to work independently of current fitness, rather than being a mediating mechanism. Limiting the stiffening of the central arterial system that occurs with age, in combination with increased fitness may help to ameliorate cognitive decline in older people and assist in protecting from cognitive impairment and dementias.
Footnotes
ACKNOWLEDGMENTS
The resources of Centre for Human Psychopharmacology, Swinburne University of Technology, Melbourne, have been used to conduct this study. Collection and storage of biological sample were provided by Dorevitch Pathology. Access to participants and facilities was provided by Australian Unity Ltd, BaptCare Ltd, Churches of Christ in Queensland Ltd., and Catholic Homes Ltd. This study would not be possible without these supporters, and it is greatly appreciated by the Swinburne LIILAC team.
Additional review and advice on the development and structure of this manuscript was provided by Mr. Jeffery Reddan and Dr. Lee Lawrence.