
Abstract
In many cohort studies of dementia, while differences in sociodemographic characters between responders and non-responders of dementia screening have been reported, differences in dementia beliefs have been relatively less known. The aims of this study were to clarify dementia beliefs and to explore potential impacts on an intention to attend a future dementia screening in public screeners and in-home screeners, respectively. We performed a cross-sectional population-based study using a question about an intention to attend a future dementia screening and a questionnaire on dementia beliefs. Subjects were all residents aged 65 years or older in the north area of Nakajima, Japan (n = 385). All subjects were asked to attend a public dementia screening first. An in-home dementia screening was subsequently conducted in subjects with non-responders to a public screening. The questionnaire consisted of four dementia beliefs: “perceived susceptibility,” “perceived severity,” “perceived barriers,” and “perceived benefits.” Public screeners significantly expressed an intention to attend a future dementia screening more than in-home screeners (p = 0.002). In in-home screeners, low “perceived severity” were significantly associated with an intention to attend a future dementia screening [adjusted OR (95% CI) = 0.51 (0.32–0.80)]. In both public and in-home screeners, high “perceived benefits” were significantly associated with an intention to attend a future dementia screening [adjusted OR (95% CI) = 2.13 (1.46–3.10); adjusted OR (95% CI) = 2.56 (1.22–5.35), respectively]. It is necessary to reduce “perceived severity” among in-home screeners to increase dementia screening participants.
INTRODUCTION
It is expected that the number of people with dementia worldwide will increase year by year. A systematic review of epidemiological studies showed that estimated number of people having dementia was 35.6 million worldwide in 2010 [1]. This crude prevalence of dementia was 4.7% in people aged 60 years or older [1]. Furthermore, the number would be predicted to be increased two-fold every 20 years [1]. On the other hand, some studies reported in recent years that incidence or prevalence of dementia decreased or tend to decrease as compared with the past [2–7]. The reason for these trends has been unclear, whereas these studies proposed that the incidence or prevalence might be decreased by better education or better medical therapies [2, 3]. We have conducted a dementia screening in public halls as part of a population-based cohort study to investigate the correlation between lifestyle and the prevalence of dementia since 2006. However, more than 60% of the eligible residents did not respond to our invitation to participate in public screenings [8].
Many community-based studies have reported differences in socio-demographic characteristics such as gender [9], age [8–11], and years of education [8, 11] between responders and non-responders to a dementia screening. Meanwhile, there is a few community-based studies to deal with psychological factors toward intention or behavior to attend a dementia screening. An Irish survey reported that barriers to help-seeking intention were a lack of knowledge, fear, loss, stigma, and inaccessible services [12].
The health belief model (HBM) is a representative theory for health promotion and disease prevention. In the HBM, four perceived beliefs are assumed: susceptibility to a condition, severity of a health problem, and benefits and barriers to taking action concerning health promoting behavior [13]. Although cue to action, a trigger of the decision-making process, has been recommended to be included in the HBM [13], a few studies have included it [14, 15]. There have been many HBM-based studies on cancer [16–25] but a few on dementia [26–30]. As far as we know, there are two studies about the psychological factors with HBM in subjects with community residents [26, 30]. However, it may be unusual for the community residents in their survey area to attend a free dementia screening in public halls regularly. We have conducted a cohort study (the Nakajima Study) in subjects with all residents aged 60 years or older in our survey area Nakajima since 2006 and the residents can attend it every year. Individual dementia beliefs related to an intention to attend a dementia screening would vary depending on whether they can regularly attend it or not.
The aims of this study were to clarify dementia beliefs and to explore potential impacts on an intention to attend a future dementia screening, using a questionnaire based on the HBM in non-demented public screeners and in-home screeners, respectively.
METHODS
Study subjects
Since 2006, the Nakajima Study was conducted in subjects with all residents 60 years or older in Nakajima, Ishikawa Prefecture, Japan and supported by Nanao City, and information from this residence was used to list target candidates and send invitations. This current cross-sectional study was performed between September 2012 and February 2013 as a part of the Nakajima Study. All residents who live in the northern area of Nakajima on Prevalence Day (1 April 2012) aged 65 years or older were this study subjects (n = 385).
We started recruitment for this survey in May 2012 by advertising in individual letters and flyers around public halls. They carried information that public dementia screenings were performed in public halls. Their public halls were located within 4 km from individual households. This distance means a general standard of elementary school establishment in Japan. Subsequently, we visited those whom did not attend a public dementia screening (in-home screening). Both screenings were free. The in-home screening was conducted in order to assess cognitive functions, an intention to attend a future dementia screening, and dementia beliefs of non-participants in the public screening. Both screenings included the same questionnaires on personal lifestyle, medical conditions, activities of daily living (ADLs), an intention to attend a future dementia screening, and dementia beliefs as well as the same neuropsychological tests. Before scheduling the in-home screening, a letter was sent to each potential candidate explaining the study objectives.
This study was performed with the help of collaborators from the neighborhood association (local welfare commissioners and neighborhood association chairmen). They asked the subjects to participate in this survey in addition to the invitation letter and the flyer. We used Japanese in all situations and all participants could understand Japanese. The present study was performed by five neurologists, two psychologists, five nurses, one physiotherapist, and one occupational therapist, all of whom were specifically trained for this study.
Intention to attend a future dementia screening
An intention to attend a future dementia screening was assessed with a single question: “If you were invited to take a dementia screening test in the future, would you take up the offer?” The response options provided were as follows: “Yes, definitely,” “Yes, probably,” “Not sure,” “Probably not,” or “Definitely not.” Participants who answered “Yes, definitely” or “Yes, probably” were classified into the subgroup “with an intention” to attend a future dementia screening. Participants who answered “Not sure,” “Probably not,” or “Definitely not” were classified into the subgroup “without an intention” to attend a future dementia screening.
Development of the dementia belief scale
In order to fix items on a questionnaire on dementia beliefs (dementia belief scale), we referred to previous studies based on HBM, which included not only for dementia but also for other disease (e.g., cancer) because there were only a few studies for dementia at that time. We collected items for these previous scales and adopted 15 items on the dementia belief scale (Table 1), considering characteristics of region and general older people. The response of each item was scored: three points for “strongly agree” or “agree,” two points for “not sure,” and one point for “disagree” or “strongly disagree”.
Items of the dementia belief scale
The dementia belief scale consisted of above-mentioned 15 items before factor analysis was conducted and 11 items were adopted after the factor analysis.
Data collection
Each participant completed self-administered questionnaires as follows: socio-demographic data (including gender, age, and years of education), the Barthel index items [31], and the Geriatric Depression Scale (GDS-15) items [32]. In addition, participants also filled out the question about an intention to attend a future dementia screening and the dementia belief scale. Completed questionnaires were reviewed by the trained researchers to identify unreliable answers (e.g., vague, careless, or irresponsible answers). The Barthel index determined whether the individual could perform 10 ADLs tasks “independently,” “with some help,” or “not at all.” The following activities were evaluated: feeding, transfers, grooming, use of toilet, bathing, mobility, use of stairs, dressing, bowel function, and bladder function. Barthel index scores of 100 indicate normal function, while scores of 95 or lower indicate functional disability. The GDS-15 inventory measures depressive symptoms. Subjects scoring six or more were considered to have depressive symptoms. To assess cognitive status, all participants completed neuropsychological tests, including the Mini-Mental State Examination (MMSE) [33] and Clinical Dementia Rating (CDR) [34, 35]. Their neuropsychological batteries were conducted by the trained researchers. Low MMSE scores are associated with cognitive decline. CDR is a dementia staging instrument used to rate cognitive function along five levels of impairment from none to maximal (rated as 0, 0.5, 1, 2, or 3) in each of the following six domains: memory, orientation, judgment and problem solving, function in community affairs, home and hobbies, and personal care. Global CDR scores were calculated using an algorithm that considers each subscore. The overall possible range for global CDR score is as follows: 0 (indicating a normal healthy individual with no cognitive or functional deficits), 0.5 (a normal healthy individual but with questionable cognitive and/or functional abilities), 1 (mild dementia), 2 (moderate dementia), and 3 (severe dementia).
Diagnosis of dementia
The diagnosis of dementia was based on the guidelines of the Diagnostic and Statistical Manual of Mental Disorders, third edition, revised (DSM-III-R) [36]. The criteria have been used for following up all participants in our cohort study since 2006.
Standard protocol approval and patient consent
This study was performed with the approval of the medical ethics review board of Kanazawa University (Kanazawa, Japan). All participants provided written informed consent using a form that included the purpose and procedures of the study, potential risks and benefits associated with participation, strict voluntary nature of participation, right to withdraw from the research without prejudice or penalty, and a guarantee of confidentiality and security of personal data.
Statistical analysis
Factor analyses and Chronbach’s α coefficient were performed to verify construct validity and internal consistency of the dementia belief scale. Spearman’s rank correlation coefficient was used. Comparisons between groups of subjects (i.e., public screeners versus in-home screeners) were performed using analysis of variance, chi-square, or Mann-Whitney tests as appropriate. Multivariate logistic regression models were used to determine the effect of dementia beliefs on an intention to attend a future dementia screening. Model 1 was gender-, age-, and education-adjusted. Model 2 was further adjusted for the dementia belief scale score. Statistical significance was defined as p < 0.05. Statistical analyses were performed using the SPSS software package (version 22.0J; SPSS Inc., Chicago, IL, USA).
RESULTS
Study participants
Of the 385 potential candidates, 17 were excluded: eight died, eight moved, and one was uncontactable (Fig. 1). The remaining 368 residents were considered as baseline candidates. A total of 207 candidates participated in the public dementia screenings in public halls (participation rate = 56.3%). These subjects were considered as “public screeners.” Residents who participated in the in-home screeners (n = 114, 31.0%) were considered “in-home screeners.” In total, 337 residents (91.6% of baseline candidates) participated in the present study. We excluded 93 subjects, including those with dementia (n = 43), those with mental disorder (n = 1), those who failed to complete the questionnaires or examinations (n = 33), and those who were institutionalized (n = 16). Overall, data from 244 subjects (107 men and 137 women) were analyzed. Concerning the final non-responders who were 8.4% of the baseline candidates, we did not have any information about either the socio-demographic characteristics, an intention to attend a future dementia screening, or dementia beliefs.
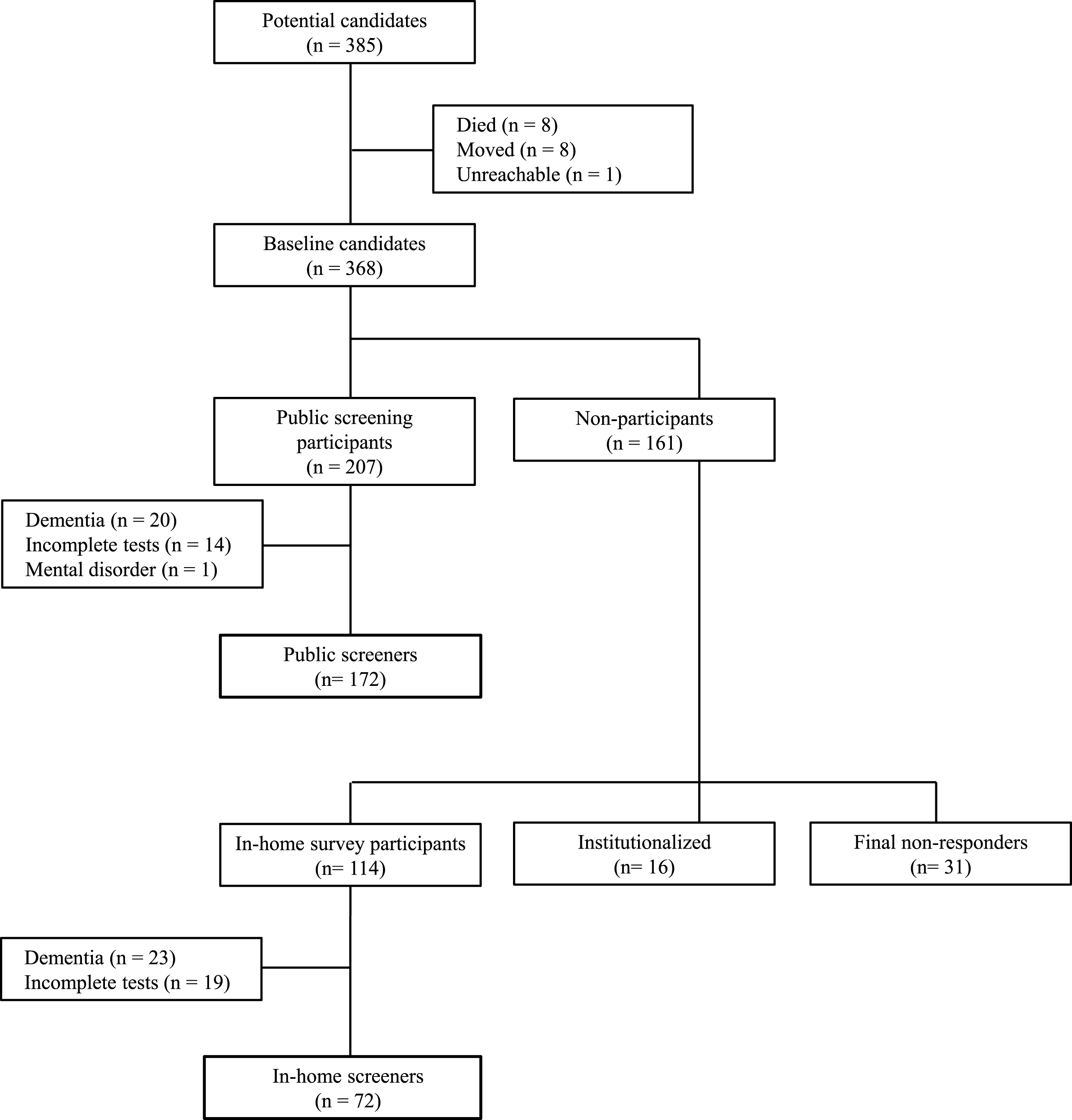
A flow chart of the subjects. The process of classifying into public screeners and in-home screeners were shown in this chart.
Differences in characteristics between public and in-home screeners
The characteristics of the study subjects are shown in Table 2. A comparison between public and in-home screeners showed no difference in gender ratio, age, or years of education. Compared with public screeners group, in-home screeners group had significantly lower MMSE scores (p = 0.048) and higher frequencies of functional disability (p = 0.013).
Characteristics of public and in-home screeners
1)p values were assessed between public and in-home screeners. GDS, Geriatric depression scale; MMSE, Mini-mental state examination; CDR, Clinical dementia rating.
Intention to attend a future dementia screening
A half (n = 136, 55.7%) of subjects expressed an intention to attend a future dementia screening: 41.8% of subjects expressed definitely, and 13.9% of them expressed probably to attend a future dementia screening. Public screeners significantly expressed an intention to attend a future dementia screening (62.2%) more frequently than in-home screeners (40.3%) (p = 0.002) (Table 2).
The dementia belief scale
Regarding each item on the dementia belief scale, most participants (94.3%) answered “strongly agree” for item Q5 (“Do you think that your family or close friends have a trouble if you get dementia?”). We also found a strong correlation between items Q1 (“Do you have a high probability of getting dementia within a few years?”) and Q2 (“Do you have a high probability of getting dementia in future?”) (r = 0.71, p < 0.01) and relatively strong correlation between items Q1 and Q3 (“Do you have a higher probability of getting dementia than people of the same generation?”) (r = 0.588, p < 0.01) and between Q2 and Q3 (r = 0.567, p < 0.01). Thus, we excluded items Q5 and Q2 from latter analyses. Four factors were extracted using a principal factor method with a direct oblimin rotation for factor analysis. Items Q4 (“Do you think that dementia is not cured?”) and Q11 (“Do not you need to have an examination of cognitive functions, because you do not feel the any kinds of problems as you should be had one?”) were excluded from the last factor analysis because their factor loading was <0.35. The rationale underlying factor formation is described in Table 3. Internal consistency of each factor including more than one item was measured by Chronbach’s α coefficient (ranging from 0–1), with 0.6 or more considered to be a sufficient value. The four factors (Chronbach’s α) were named “perceived barriers” (0.65), “perceived benefits” (0.49), “perceived susceptibility” (0.75), and “perceived severity” (0.67). Consequently, Q1 and Q3 belonged to “perceived susceptibility”; Q6 (“Are you afraid that you think about time to get dementia?”) and Q7 (“Does your whole life worsen if you get dementia?”) belonged to “perceived severity”; Q8 (“Do early dementia detection and treatment get better treatment effect?”) and Q9 (“Can having an examination of cognitive functions detect dementia early?”) belonged to “perceived benefits”; and Q10 (“Are you afraid that you may be stigmatized as dementia due to have an examination of cognitive functions?”), Q12 (“Are you difficult to have an examination of cognitive functions, because you do not have transportation?”), Q13 (“Are you afraid to have an examination of cognitive functions, because you do not know what is examined?”), Q14 (“Are you ashamed to have an examination of cognitive functions?”), and Q15 (“Does having an examination of cognitive functions take time?”) belonged to “perceived barriers” (Table 1).
Factor loading of the dementia belief scale
The result of factor analysis was shown as above. Inter-Factor correlations were as follows: –0.124 between Factor 1 and 2; –0.243 between Factor 1 and 3; –0.193 between Factor 1 and 4; –0.058 between Factor 2 and 3; –0.291 between Factor 2 and 4, and 0.216 between Factor 3 and 4.
Dementia beliefs in public screeners
Dementia beliefs were compared between public screeners with and without an intention to attend a future dementia screening (Table 4). Among public screeners, the “perceived benefits” score for the “with an intention” subgroup was significantly higher than that of the “without an intention” subgroup (p < 0.001).
Characteristics between with and without an intention to attend a future dementia screening in public and in in-home screeners
1)p values were assessed between public screeners with and without intention to attend a future dementia screening. 2)p values were assessed between in-home screeners with and without intention to attend a future screening. GDS, Geriatric depression scale; MMSE, Mini-Mental State Examination; CDR, Clinical dementia rating.
Dementia beliefs in in-home screeners
Dementia beliefs were compared between in-home screeners with and without an intention to attend a future dementia screening (Table 4). With regard to public screeners, compared with the “without an intention” subgroup, the “with an intention” subgroup had a significantly higher “perceived benefits” score (p = 0.017) and tendency toward lower “perceived severity” scores (p = 0.064) (Table 4).
Relation between an intention to attend a future dementia screening and dementia beliefs in public screeners
In multivariate analysis adjusted sociodemographic factors (gender, age, and years of education) among public screeners, there is no relation to an intention to attend a future dementia screening. In multivariate analysis adjusted four factors on the dementia belief scale in addition to the sociodemographic factors, high “perceived benefits” scores were significantly associated among public screeners with an intention to attend a future dementia screening [adjusted OR (95% CI) = 2.13 (1.46–3.10)] (Table 5).
Odds ratios from logistic regression analyses of an intention to attend a future dementia screening in public screeners
a)Model 1 was adjusted to gender, age and education, and χ2 = 0.682 with 4 df (p = 0.953). b)Model 2 was adjusted to perceived susceptibility, perceived severity, perceived benefits and perceived barriers in addition to model 1, and χ2 = 21.925 with 8 df (p = 0.005).
Relation between an intention to attend a future dementia screening and dementia beliefs in in-home screeners
In multivariate analysis adjusted sociodemographic factors (gender, age, and years of education) among in-home screeners, there is no relation to an intention to attend a future dementia screening. In multivariate analysis adjusted four factors on the dementia belief scale in addition to the sociodemographic factors, low “perceived severity” scores and high “perceived benefits” scores were significantly associated with an intention to attend a future dementia screening [adjusted OR (95% CI) = 0.51 (0.32–0.80) and 2.56 (1.22–5.35), respectively] (Table 6).
Odds ratios from logistic regression analyses of an intention to attend a future dementia screening in in-home screeners
a)Model 1 was adjusted to gender, age and education, and χ2 = 3.528 with 4 df (p = 0.474). b)Model 2 was adjusted to perceived susceptibility, perceived severity, perceived benefits and perceived barriers in addition to model 1, and χ2 = 22.045 with 8 df (p = 0.005).
DISCUSSION
In the present study, we clarified dementia beliefs in public screeners and in-home screeners, respectively, and revealed that each group had different dementia beliefs which impacts on an intention to attend a future dementia screening. We clarified for the first time that predictors of lack of an intention to attend a future dementia screening were different between public screeners and in-home screeners. In our study, 55.7% of subjects expressed an intention to attend a future dementia screening, and public screeners significantly expressed the intention more than in-home screeners (p = 0.002). The intention to attend a future dementia screening was significantly inversely related to “perceived severity” in-home screeners [adjusted OR (95% CI) = 0.51 (0.32–0.80)]. The high intention was significantly associated to high “perceived benefits” in the both the groups [adjusted OR (95% CI) = 2.13 (1.46–3.10); adjusted OR (95% CI) = 2.56 (1.22–5.35)].
The characteristics that affect the differences in an intention to attend a future dementia screening between public and in-home screeners
In-home screeners significantly expressed a lower intention to attend a future dementia screening than public screeners (p = 0.002). Differences in the intention might depend on difference in characters between public screeners and in-home screeners. The in-home screeners showed significantly lower MMSE score (p = 0.048) as compared with public screeners, although we collected data of non-demented screeners and gender, age, years of education, or CDR was not significantly different between public screeners and in-home screeners. It was reported that a decline in MMSE total score in non-demented subjects was associated with future dementia in the community-based study [37]. Therefore, our results raise the possibility that in-home screeners are easier to progress to dementia than public screeners. Moreover, in-home screeners had significantly higher frequencies of functional disability than public screeners (p = 0.013). Functional disability might be associated with decline of the intention. Additionally, in-home screeners also expressed significantly lower “perceived benefits” as compared with public screeners (p = 0.045).
The relationship between an intention to attend a future dementia screening and perceived severity among in-home screeners
We clarified for the first time that “perceived severity” was a predictor for non-demented in-home screeners (non-responders of the dementia screening in public halls). As far as we know, there have been two previous HBM-based studies on dementia with community residents similar to our study. One study concluded that “perceived barriers” and cue to action were significant predictors of an intention to seek a cognitive status examination [26]. Another study reported that “perceived benefits” was a main predictor of participation in a cognitive impairment screening [30]. Whereas other previous studies without the HBM indicated that fear might prevent to help-seeking intention [12, 38]. Fear is related to perceived severity and susceptibility, because these beliefs constitute threat and threat is one of an external stimulus of fear appeal [39]. Our result suggests that it is important to consider how to reduce “perceived severity” in order to increase the intention to attend a future dementia screening in in-home screeners. However, it is actually difficult to find a universal way to reduce “perceived severity” and thus it is necessary to make steady efforts: trained experts regularly contact with community residents who avoid to attend a dementia screening, build trusting relationship with them individually and advise them to reduce excessively high “perceived severity”.
The relationship between an intention to attend a future dementia screening and perceived benefits of a dementia screening in both public and in-home screeners
In both public and in-home screeners, “perceived benefits” proved to be a predictor of an intention to attend a future dementia screening. Our results indicated that the person who has an idea that early detection of dementia is useful for early treatment and better prognosis tends to have an intention to attend the dementia screening, which is consistent with the previous study [30].
Strength and limitations
The strengths of our present study include the community-based study design and high response rate (91.6%), whereas one important limitation is that we could not analyze the association between the behavior to attend a future dementia screening and beliefs for final non-responders who comprised 8.4% of the baseline candidates. The second limitation of our study is the low internal consistency between “perceived benefits” variables (Chronbach’s α= 0.49). In addition, we did not examine knowledge about dementia, mental status or personality, social support, or cue to action. Development of a more suitable version of the dementia belief scale with evaluation studies is needed for future study.
Conclusion
In conclusion, dementia beliefs related to an intention to attend a future dementia screening were different between public screeners and in-home screeners. “Perceived severity” is a significant predictor of lack of an intention to attend a future dementia in in-home screeners. Furthermore, “perceived benefits” also proved to be a predictor of the intention in both public and in-home screeners.
Footnotes
ACKNOWLEDGMENTS
We are grateful to all the residents of Nakajima for their participation in the present study. This study was supported in part by a Grant for the Hokuriku Innovation Cluster for Health Science from the Ministry of Education, Culture, Sports, Science, and Technology, Japan, and by a Health and Labour Sciences Research Grant from the Ministry of Health, Labour and Welfare, Japan (Research on Dementia). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.