
Abstract
Background:
Many patients with early-onset Alzheimer’s disease (EOAD; age of onset <65 years) have non-amnestic presentations involving language (logopenic primary progressive aphasia, lvPPA), visuospatial abilities (posterior cortical atrophy, PCA), and even asymmetric symptoms consistent with corticobasal syndrome (CBS). An inferior parietal lobule variant of EOAD commonly presents with progressive difficulty with calculations.
Methods:
We reviewed 276 EOAD patients for presentations with predominant acalculia. These patients were diagnosed with clinically probable Alzheimer’s disease (AD) verified by positron emission tomography (PET) or cerebrospinal fluid amyloid-β or tau biomarkers.
Results:
We identified 18 (9M/9F) (6.5%) EOAD patients with progressive acalculia that did not meet most criteria for lvPPA, visual PCA, or CBS. Their ages of onset and presentation were 56.6 (5.0) and 59.4 (6.5), respectively. Their acalculia was consistent with a primary acalculia (“anarithmetia”) not explained by language or visuospatial impairments. Many also had anomia (14/18), ideomotor apraxia (13/18), and the complete Gerstmann’s syndrome (7/18). Visual analysis of their diverse magnetic resonance imaging disclosed biparietal atrophy, disproportionately worse on the left.
Conclusions:
Primary acalculia may be the most common manifestation of an inferior parietal presentation of EOAD affecting the left intraparietal sulcus. This parietal variant also commonly involves progressive anomia, ideomotor apraxia, and other elements of Gerstmann’s syndrome. The early recognition of patients with this variant, which is distinguishable from lvPPA, visual PCA, or CBS, would be facilitated by its recognition as a unique subtype of EOAD.
INTRODUCTION
Although Alzheimer’s disease (AD) is a major and growing healthcare problem, it can be difficult to diagnose on initial presentation. Most clinicians recognize AD among elderly persons presenting with memory impairment, a presentation that is supported by the clinical diagnostic criteria for AD [1]. However, AD among middle-aged or younger patients (EOAD; age of onset <65 years), such as Alois Alzheimer’s original patient, Auguste Deter [2], may have predominant non-amnestic presentations that are less typical of AD. Clinicians often fail to initially recognize these early-onset AD (EOAD) patients as having AD, resulting in significant delays in diagnosis [3].
In order to improve recognition and diagnosis, investigators have proposed classifications and specific diagnostic criteria for the major non-amnestic, focal cortical EOAD syndromes [4–7]. These include logopenic variant primary progressive aphasia (lvPPA), which presents with impairments in naming and sentence repetition [8, 9], posterior cortical atrophy (PCA), which presents with disproportionate visuospatial and visuoperceptual deficits [10], and asymmetric involvement with motor and other changes consistent with corticobasal syndrome (CBS) [11]. Another EOAD variant, known as the behavioral/dysexecutive variant, may affect frontal regions of the brain, similar to frontotemporal dementia [12].
A further, incompletely characterized subtype of EOAD is a “parietal variant” presenting with progressive acalculia, or disturbances in the manipulation of numbers or quantities. Acalculia has many causes and can be a primary disturbance of mathematical abilities or secondary to language, visuospatial, working memory, or other cognitive impairments. Acalculia in the parietal variant may occur with other elements of Gerstmann’s syndrome (agraphia, right-left confusion, digit agnosia) consequent to involvement of the left inferior parietal lobule [13]. Acalculia in AD may also occur with other left parietal symptoms, such as ideomotor apraxia, or may overlap with lvPPA, PCA, or CBS.
Although prior research has described acalculia and disturbed mathematical abilities as a symptom of AD [14–20], they have not focused on an acalculia variant. These studies have primarily focused on describing the identification of acalculia in AD patients, particularly in comparison to normal controls, and the correlation of worse calculation difficulty with increased severity of dementia [18, 19]. Several describe acalculia as a hallmark cognitive feature of AD that should be included as a criterion for dementia [18–20]. They have not reviewed acalculia as the presenting and predominant presentation of a parietal variant of EOAD. This study additionally evaluates the nature of the acalculia and its relationship with Gerstmann’s syndrome and other regional symptoms in AD.
METHODS
Participants
For participation in this study, we retrospectively screened all patients from a subspecialty university clinic who were clinically diagnosed by National Institute on Aging-Alzheimer’s Association (NIA-AA) criteria over a twelve year period [1]. Patients presenting before 2011 had been reevaluated and diagnosed with these NIA-AA criteria. We screened for all patients who met the diagnosis of “probable AD dementia with evidence of the AD pathophysiological process” [1]. The biomarkers indicating the “AD pathophysiological process” included either magnetic resonance imaging (MRI) findings and fluorodeoxyglucose positron emission tomography (PET) imaging as markers of neuronal degeneration or one of two markers of amyloid-β deposition: cerebrospinal fluid (CSF) amyloid-β and tau or amyloid PET imaging. Apolipoprotein E levels were not collected in this clinic cohort. Inclusion criteria also included only patients who had an age of onset of less than 65 years, and exclusion criteria also included patients with proven familial AD (FAD), or family histories of early-onset dementia suggestive of autosomal dominant transmission as FAD may be associated with a unique constellation of neurological findings [21]. The final retrospective screen included a total of 276 EOAD patients.
Clinical evaluation
Among these 276 patients, we identified 18 whose main presentation was difficulty with numbers, quantities, or calculations out-of-proportion to other symptoms or signs and who did not meet criteria for lvPPA, visual PCA, or CBS. Their individual records were extensively reviewed and coded for the characteristics of their acalculia and other cognitive features from their intake evaluations. All patients in this program received an extensive neurocognitive assessment on intake, included assessment of their calculation ability, praxis, and examination for Gerstmann’s syndrome [22]. Calculation ability included [23, 24]: 1) Dot enumeration and number counting, 2) Reading simple numbers (<1000), 3) Quantity estimation (larger versus smaller), 4) Identification of the four common arithmetic signs, 5) Evaluation of alignment or placement of numbers in simple arithmetic, 6) Mental calculations of simple problems, 7) General numerosity (in the sense of application of numeric concepts), and 8) Written calculations, particularly focusing on completion of the problems and errors such as borrowing or carrying-over. In addition, the mechanical aspects of number writing was assessed. The patient’s calculations were available for review and coding from their intake worksheets. We additionally reviewed their neuroimaging, often uploaded from outside institutions and scanners, as well as their CSF biomarkers. This de-identified chart review was approved by the UCLA Institutional Review Board.
Neuroimaging
These patients presented from varying sources and had MRI of their brains from different scanners and different institutions. Referral to the subspecialty clinic required that outside imaging be sent with the patients for review. Because of the different sources of the clinical MRI scans, semi-quantitative visual ratings of parietal atrophy and hippocampal atrophy were employed by the clinicians in our program [25]. Axial fluid-attenuated inversion recovery (FLAIR) MRI images was characterized with the Koedam Parietal Atrophy Scale (PAS) [26]. The PAS scores rated parietal atrophy on a scale of 0 (closed sulci of parietal lobes and cuneus), 1 (mild widening of posterior cingulate and parietal-occipital sulci), 2 (substantial widening of the sulci), and 3 (extreme widening of the posterior cingulate and parietal-occipital sulci). In addition, the medial temporal atrophy (MTA) scale was applied as a measure of hippocampal size on coronal MRIs at mid-pontine level [27]. Noncontrast T1-weighted sequences were preferentially used for these analyses. The scoring for this scale was similar to the PAS but with a range of 0 (no atrophy) to 4 (severe atrophy). For both these scales, right and left side were rated separately and subsequently compared.
Statistical analysis
Simple descriptive statistics were used to describe the patients and findings. The two neuroimaging scale scores were compared between left and right with dependent measures t-tests (two-tailed).
RESULTS
We identified 18 (9M/9F) EOAD patients who presented with 1) chief complaints consistent with predominant difficulty from acalculia, and 2) severe acalculia on testing disproportionate to any problems with language or visuospatial abilities (See Table 1). Their chief complaints ranged from inability to do simple calculations to confusion over large number quantities (See Table 2), and their acalculia testing is described below. These patients did not otherwise differ in basic characteristics from the rest of the EOAD population.
Characteristics of patients with early-onset Alzheimer’s disease (EOAD): acalculia variant versus non-acalculia variants
All numbers are means (standard deviations) except for sex (n = number; % = percent); MMSE, Mini-Mental State Examination on presentation; CDR, Clinical Dementia Rating scores on presentation (not available on all Other Variants).
Presenting symptoms/problems among 18 parietal variant patients
Although most of the 18 patients with acalculia had language difficulty or visuospatial impairments at the time of presentation, these were not their main difficulties and were not as severe as their acalculias, and they did not meet most criteria for lvPPA, visual PCA, or CBS [9, 29]. The language difficulty was consistent with word-finding difficulty with five also showing a prominent alexia, not due to visuospatial difficulties in processing the written words. In addition to language difficulty, a common feature among these patients was ideomotor apraxia, generally involving both upper extremities but worse on the left. The neurocognitive assessments indicated that the patients with limb apraxia, who were screened with both transitive and intransitive acts and pantomime and imitation, did poorly on all of these tasks; However, they retained the ability to recognize gestures. The visuospatial impairments were primarily detected in performing visuospatial constructions, as occurs in most AD patients. None of the 18 patients reported here had major visuospatial symptoms or Balint syndrome, except two more advanced patients who had dressing apraxia and complaints of impaired depth perception. No patient had parkinsonism, myoclonus, or dystonia suggestive of CBS (See Table 3).
Accompanying symptoms/features
*Two patients with problems with depth perception and dressing apraxia and three others with abnormalities on figure-ground and perceptual organization. **Auditory verbal learning scores with additionally poor recognition memory on multiple choice testing.
The acalculia was most consistent with a primary acalculia or “anarithmetia”. Although there was some heterogeneity in the mathematical difficulty, the neurocognitive assessment did not suggest secondary causes of acalculia, such as impairments in reading or writing numbers, predominant problems with number placement or alignment as in spatial acalculia, or mechanical difficulties. The exception is the difficulty evident in simple mental calculations; However, all of these patients had difficulty in written simple calculations as well, indicating that working memory was not the main problem. Most patients had at least one other element of the full Gerstmann’s syndrome, with agraphia, and not right-left discrimination or digit agnosia, being the second most common symptom after acalculia. The entire Gerstmann’s syndrome was present in 39% (See Table 4).
Calculation characteristics of 18 patients
The laboratory studies were consistent with a biparietal variant of AD, with worse involvement of the left parietal lobe. MRI brain scans showed significantly more involvement of the left parietal region on the PAS (Right: 1.94±0.75 versus Left: 1.35±0.61); difference scores: –0.06±0.12; t (for two dep means) = –4.781, p < 0.001 (two-tailed). For the MTA scale, the patients had worse left temporal atrophy (Right: 1.06±0.80 versus Left: 1.78±0.88); difference of –0.72±0.19; t (for two dep means) = –3.71, p = 0.001 (two-tailed). Cerebrospinal fluid β amyloid and tau biomarkers among 9 patients were consistent with AD (averages for these 9 patients: Aβ42 of 304.1±92.1, total tau (t-tau) of 620±365.2, phosphorylated tau (p-tau) of 82.3±33 and a Aβ42/t-tau index (ATI, calculated as Aβ42/(240 + 1.18 t-tau)) of 0.33±0.06). The other 9 patients who had FDG-PET scans instead of CSF biomarkers showed hypometabolism consistent with biparietal dysfunction greater in the left than the right parietal lobe (See Fig. 1 for an illustration of one of these patients).
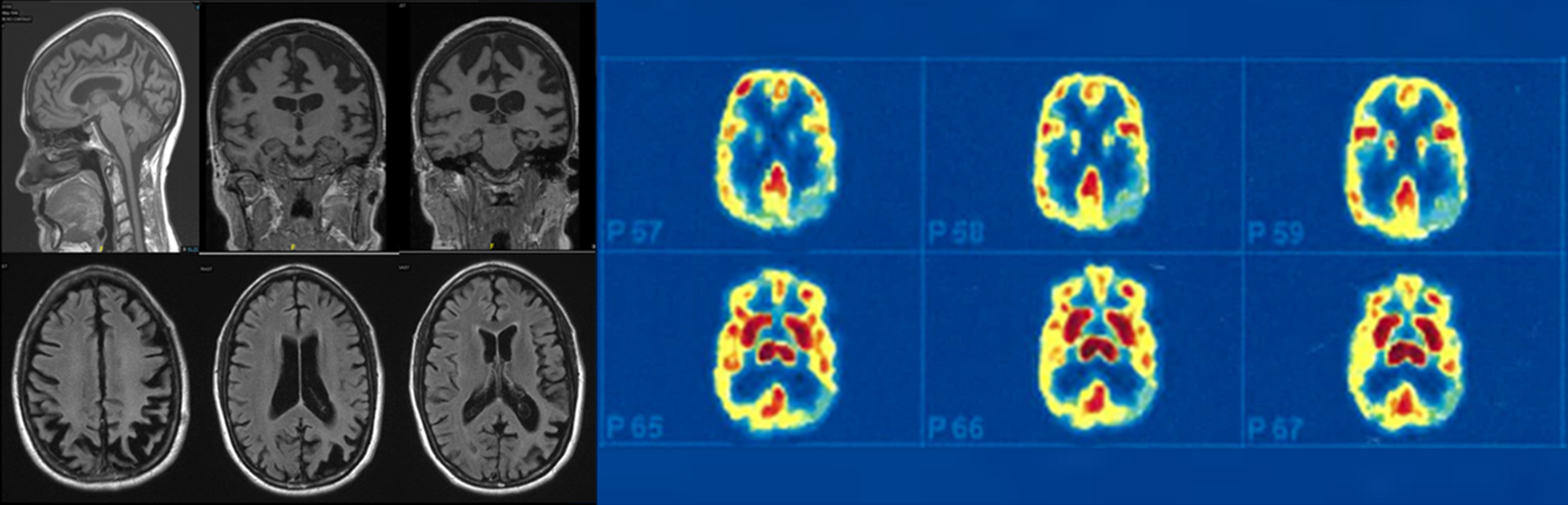
The left side shows a magnetic resonance imaging scan with biparietal atrophy (parietal atrophy scores of 3 on left and 2 on right). The right side shows that the corresponding fluorodeoxyglucose positron emission tomography (FDG-PET) scan with biparietal hypometabolism, significantly worse on the left.
DISCUSSION
This report characterizes the “acalculia” parietal variant of EOAD, with the combination of symptoms referable to disproportionate involvement of the left more than the right parietal lobe. These 18 patients presented with primary acalculia, or anarithmetia, as evidenced by their calculation characteristics. This variant is most commonly associated with other elements of Gerstmann syndrome, and has been included as part of a biparietal variant or even a non-visual PCA (“PCA2”) variant [5, 30]. Although these patients may have features that overlap with lvPPA, PCA, and even CBS, the primary acalculia or anarithmetia, along with ideomotor apraxia and anomia, suggests a unique inferior parietal (supramarginal and angular gyri and adjacent intraparietal sulcus) pathology, with greater involvement of the left hemisphere.
There are a number of EOAD subtypes that present with relative sparing of memory [5, 31]. These variants have hippocampal sparing on neuropathology with greater cortical neurofibrillary tangles [32], particularly in left hemisphere language areas in lvPPA [33, 34] and in visual neocortex in PCA [35, 36]. One of the most common EOAD variants may be lvPPA, which is characterized by anomia with word-finding difficulty and some effortful or halting speech, phonemic paraphasic errors, and decreased sentence repetition [7–9, 37]. Most investigators describe PCA as a visual variant with predominant visuospatial problems in spatial localization and problems with visual perception due to pathology extending into the occipital lobes [10, 38–40]. The presence of abnormalities of tests of visuospatial constructions is common across all forms of AD and does not, by itself, define PCA. Others describe a behavioral/dysexecutive variant with AD pathology extending to frontal lobes [6, 12]. In addition, patients with CBS, characterized by progressive limb apraxia and motor changes, have AD in a large percentage of autopsies [28], indicating another manifestation of variant EOAD. The international Working group criteria proposed specific diagnostic criteria for most of these atypical forms of AD, but did not include a separate non-visual, acalculia variant or biparietal variant [41].
This parietal predominant variant appears to be a sufficiently separate syndrome requiring clinical consideration for the early diagnosis of these EOAD patients [42, 43]. Reports have referred to these patients as having progressive biparietal atrophy [44], left parietal apraxia variant [6], slowly progressive apraxia [45, 46], progressive acalculia [43], and apraxia/visuospatial or aphasic-apraxic-agnosic subtype when language is additionally affected [5]. Limb apraxia is a common symptom of this variant [44, 47–51], which is ideomotor with difficulty with both pantomime and imitation, rather than the conceptual or ideational limb apraxia seen in more advanced AD patients [52–56]. Some investigators have expanded PCA criteria to essentially include two main posterior or PCA variants of AD, a typical visual PCA and a biparietal predominantly nonvisual PCA2 [30, 57]. However, in these PCA patients, acalculia, along with limb apraxia and Gerstmann’s syndrome [58, 59], correlate with left inferior parietal damage, distinct from the bilateral occipitoparietal or occipitotemporal damage in typical visual PCA. Furthermore, the non-visual characteristics are quite distinct and, including them in PCA not only obscures the distinct nonvisual biparietal presentation, but it also obscures the unique clinical presentation of PCA as a visual variant of AD. Nevertheless, the inferior parietal variant can overlap with visual PCA. Among the patients in this report, two showed overlap symptoms in having dressing apraxia not due to ideomotor apraxia, and difficulties with depth perception, but not other complex visual complaints. These two patients differed in being further along in their disease (both presented six years after onset) and having greater involvement in the right parietal region, along with left parietal atrophy/hypometabolism. Right parietal dysfunction is often present with dressing apraxia, a disturbance of spatially orienting a body part to clothing [60], and difficulty integrating monocular as well as binocular depth cues [61].
Acalculia, more than other nonvisual symptoms, may define a truly parietal form of AD focused on the inferior parietal region. In AD, relatively isolated “progressive acalculia” occurs from selective involvement of the inferior parietal cortex [43]. Prior research has described acalculia and disturbed mathematical abilities as a prominent symptom of AD in comparison to normal controls and in relation to the severity of dementia [14–20]. In AD, the loss of number processing and calculation can be heterogeneous, unrelated to other cognitive domains [20], with some preservation of numerosity knowledge, retrieval of arithmetic facts, and ability for magnitude comparisons [15–17]. Multiple different types of calculation errors occur in AD, including in borrowing, carrying-over, number position and ordering, and other procedures [14, 19], but the earliest may be numeral transcoding deficits, especially intrusion of digits into the alphabetic script [18, 62–64]. Parietal injury, However, may leave relatively intact the processing of simple number quantity (number comparison) [14], as in our patients. In contrast, there may be associated features of parietal injury, such as ideomotor apraxia, verbal and written language difficulty, and non-acalculia elements of Gerstmann’s syndrome (agraphia, digit agnosia, left-right discrimination difficulties [13]).
Our patients had a primary acalculia, which commonly results from disturbances in the left parietal cortex, rather than a secondary form of acalculia from other cognitive impairments [65]. Primary acalculia, or anarithmetia, presents with impairment of numerical concepts and procedures and, although an element of Gerstmann’s syndrome, primary acalculia may be dissociated from digit agnosia and its other components [13, 66]. Primary acalculia occurs in patients with damage to the horizontal segment of the intraparietal sulcus (HIPS) [67, 68], which borders the superior aspect of the inferior parietal lobule. The HIPS region plays a role in quantity processing and calculations or a central amodal representation of quantity [67, 68]. Secondary acalculias can result from linguistic defects (oral or written), executive dysfunction, and visuospatial deficits. None of these patients had sufficient language impairment to explain the disproportionate problems with calculations, but a contribution from agraphic acalculia cannot be ruled-out. We also cannot exclude further difficulty in calculations from a degree of executive dysfunction. Finally, examination of the errors on performing double-digit addition or subtraction did not indicate particular problems in alignment, which would be suggestive of spatial acalculia.
A number of factors may limit the interpretation of our results. First, the data used in this study were gathered through clinical review, and this study was not prospective. However, the clinical intake evaluations were detailed with a neurocognitive evaluation that includes worksheets with results of their calculations. Second, the calculation evaluations did not include assessments of transcoding, ordinal/ordering of digits, and mathematical facts. Nevertheless, much information was available from the actual performance on their worksheets and reports sufficiently to characterize a primary acalculia. Third, the neuroimaging was from different sources and times, hence, we used a visual semi-quantitative analysis. Further evaluation would benefit from formal quantitative neuroimaging.
Conclusions
This report characterizes a progressive primary acalculia presentation, with anomia, ideomotor apraxia, and other elements of Gerstmann’s syndrome, as a parietal variant of EOAD, distinguishable from other variants, such as lvPPA, visual PCA, and CBS. Clinicians often fail to recognize these patients early in their course, because of lack of awareness of this nonvisual posterior cortical variant of EOAD. The syndrome appears to reflect greater involvement of the left inferior parietal lobule and HIPS, suggesting a greater clinical saliency and earlier presentation when the left parietal lobe is involved more than the right. Additional characterization of these patients, including neurodegenerative and amyloid or tau biomarkers, can further elucidate this form of Alzheimer’s disease.