
Abstract
Background:
Aggregation and deposition of amyloid-β (Aβ) in the brain is the main pathological change of Alzheimer’s disease (AD). Decreased Aβ42 in the cerebrospinal fluid has been confirmed as a biomarker of AD; however, the relationship between plasma Aβ and cognitive impairment is currently unclear.
Objective:
The aim was to explore the relationship between plasma Aβ and cognitive impairment in a cross-sectional study.
Methods:
A total of 1,314 subjects (age above 40) from a village in the suburbs of Xi’an, China were enrolled between October 8, 2014 and March 30, 2015. A validated Chinese version of the Mini-Mental State Examination and neuropsychological battery were used to assess cognition. Levels of plasma Aβ42 and Aβ40 were tested using commercial enzyme-linked immunosorbent assay. Relationship of plasma Aβ and cognitive impairment was analyzed using logistic regression analysis.
Results:
Of the enrolled subjects, 1,180 (89.80%) had normal cognition, 85 (6.47%) had possible cognitive impairment and 49 (3.73%) had probable cognitive impairment. Logistic regression analysis showed that the Aβ42/Aβ40 ratio (OR = 4.042, 95% CI: 1.248–11.098, p = 0.012) and plasma Aβ42 (OR = 1.036, 95% CI: 1.003–1.071, p = 0.031) was higher in the possible cognitive impairment than that in the normal cognition group. Furthermore, the plasma Aβ42/Aβ40 ratio was higher in the possible cognitive impairment group than that in the probable cognitive impairment group (OR = 0.029, 95% CI: 0.002–0.450, p = 0.011).
Conclusions:
Levels of plasma Aβ42 and Aβ42/Aβ40 ratio were elevated in patients with possible cognitive impairment, indicating that plasma Aβ42 and Aβ42/Aβ40 ratio increases may be more pronounced in early stage of cognitive impairment.
INTRODUCTION
Cognitive impairment includes stages that increase in severity from mild cognitive impairment (MCI) to dementia. The most common cause of dementia is Alzheimer’s disease (AD), accounting for 65% of all cases. Senile plaques, a hallmark of AD in pathology [1] are primarily composed of amyloid-β (Aβ)40 and Aβ42, generated by sequential β- and γ-secretase mediated proteolytic cleavage of the amyloid-β protein precursor (AβPP) [2]. The amyloid cascade hypothesis is widely considered to underlie the pathogenesis in AD [3].
Sources of Aβ deposited in the brain and cerebral vasculature include neurons, astrocytes, microglia, and the circulatory system [4]. In peripheral circulation, various blood cells, most notably platelets, have been found to express AβPP and release Aβ into plasma [5]. Cerebrospinal fluid (CSF) and plasma Aβ levels have been shown to exist in dynamic equilibrium in both animal models and healthy individuals [6, 7]. Peripheral administration of antibodies to sequester Aβ in the plasma is associated with decreased Aβ burden in the brain [8]. Recent studies have also shown that plasma exchange with human albumin resulted in modified CSF and plasma Aβ42 levels in AD patients [9]. Transport of Aβ between peripheral circulation and the central nervous system (CNS) occurs via two receptors. The predominant pathway for Aβ clearance from the brain occurs via the low-density lipoprotein receptor related protein 1 (LRP1) [10]. In the other direction, receptor for advanced glycation end products (RAGE) mediates influx of plasma-derived Aβ from peripheral circulation into the CNS [11]. Circulating Aβ binds to soluble LRP1 (sLRP1) to prevent free Aβ from entering the brain [12], and sLRP1-Aβ complexes and free Aβ in the plasma are then cleared through the liver and kidneys [13, 14]. Dysfunction of peripheral Aβ clearance, or an imbalance between production and clearance, may elevate plasma Aβ levels, and increase Aβ accumulation and deposition in the brain.
Several studies found that in familial AD patients, plasma Aβ levels are elevated prior to onset of AD, and decline after the onset of dementia [15]. However, the relationship between plasma Aβ level and cognitive impairment is inconsistent in cross-sectional studies [16–20], possibly driven by differences in inclusion criteria, exclusion criteria, and test methods.
Moreover, in previous studies, data have been collected from white subjects in Europe and the United States; data from Chinese subjects, especially from west rural areas, are lacking. To determine the relationship between plasma Aβ and cognitive impairment, more studies are necessary. Therefore, we analyzed the relationship between plasma Aβ and cognitive impairment in mid to late life (40–85) in subjects from the west rural area of China.
METHODS
Study population
This is a population-based cross-sectional study. From October 8, 2014, to March 30, 2015, individuals from a village in the suburbs of Xi’an, located in northwestern China, were recruited. Inclusion criteria were the following: 1) 40 or more years old, i.e., born before December 31,1973; 2) permanent resident of the village, meaning that the subject was currently a resident of the village and had lived there for at least 3 years; 3) agreed to participate in the study and completed the questionnaire survey; 4) agreed to donate a blood sample, and completed plasma Aβ measurement. Exclusion criteria were the following: 1) individuals who suffered from medical conditions that could lead to cognitive impairment, e.g., inflammation of CNS (HIV, syphilis), brain trauma, epilepsy, Parkinson’s disease, congenital malformation of the nervous system, congenital mental retardation, nervous system tumor, drug intoxication, alcoholism, carbon monoxide poisoning, untreated hypothyroidism, hepatic encephalopathy, pulmonary encephalopathy, and vitamin deficiency; 2) individuals who suffered from psychosis, e.g., schizophrenia, bipolar affective disorder, severe depression, delirium; 3) individuals who suffered from an uncorrectable visual or hearing dysfunction, or had difficulty completing the neuropsychological test; 4) individuals who displayed at least one aberrant plasma Aβ40 or Aβ42 level (exceeding±3 SDs from the mean). The study protocol and the selection of subjects are shown in Fig. 1. The study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University. Written informed consent was obtained from all participants.
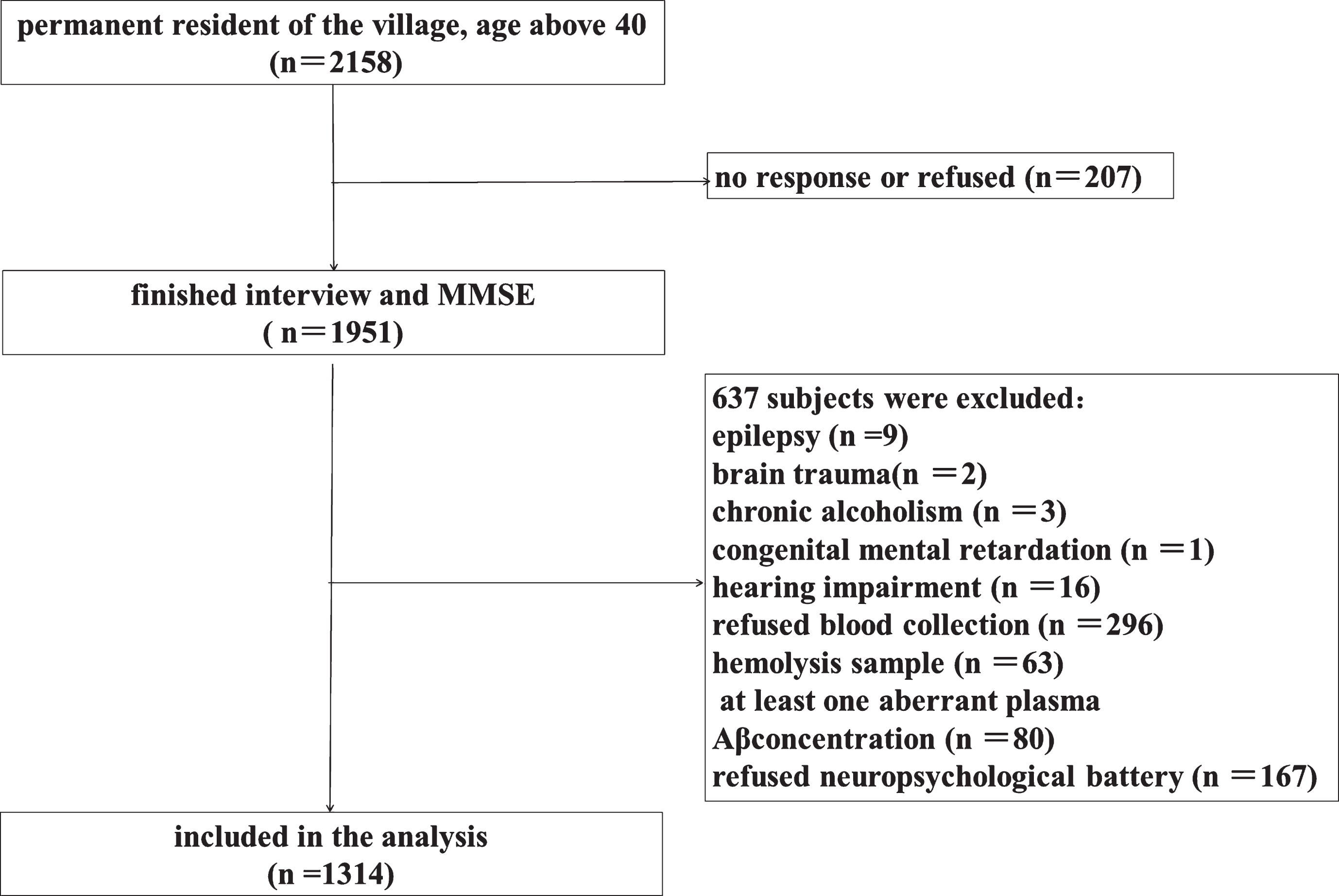
Flow chart of participant selection.
Diagnosis of cognitive impairment
Diagnosis of cognitive impairment followed a three-step protocol as previously described [21]. First, the Mini-Mental State Examination (MMSE) was used as a global assessment to screen for cognitive impairment [22]. Cutoff values were ≤17 for subjects with illiteracy, ≤20 for primary school educated subjects, and ≤24 for those educated at the junior high school level or above [23]. Second, individuals with positive screens (MMSE score below the cutoff value) underwent a neuropsychological battery that assessed different cognitive domains. The neuropsychological battery included: Clock Drawing Task [24], Fuld Object Memory Evaluation [25], Rapid Verbal Retrieval [26], Block Design Test [27], Digit Span Test [28], and Trail Making Test. Third, subjects who underwent both the MMSE and the neuropsychological battery were examined by a neurologist and were given a diagnosis according to their clinical history and neuropsychological test outcomes. The diagnosis and subtype of cognitive impairment was determined in accordance with international criteria for dementia (DSM-IV) [29], AD (NINCDS-ADRDA) [30], vascular dementia (NINDS-AIREN) [31], and mild cognitive impairment (MCI) (Petersen MCI criteria) [32].
Possible cognitive impairment was defined as subjects having an MMSE score below the cutoff value and normal results on the neuropsychological battery, while probable cognitive impairment was defined as subjects with an MMSE score below the cut off and who met criteria for MCI or dementia, and/or abnormal results on the neuropsychological battery. Investigators underwent formal training in order to ensure uniform administration of the questionnaire and standard instruction to subjects. Consistency between investigators (Kappa 0.76-1) was evaluated before the beginning of the study.
Plasma Aβ measurement
Fasting blood samples were drawn into tubes containing EDTA, an anticoagulant, at a fixed time (8-9 am), centrifuged (3000 g, 10 min) within 60 min and aliquots of plasma were stored at – 80°C pending biochemical analyses. Quantification of Aβ42 and Aβ40 in plasma was performed using sandwich enzyme-linked immunosorbent assay kits (ELISA, Yuanye Co. Shanghai, China) as previously described [33, 34]. There is no cross-reactivity of neither the Aβ42 assay with Aβ40 nor the Aβ40 assay with Aβ42. The recovery of Aβ42 assay range from 75% to 106%, 92% in average. The recovery of Aβ40 assay range from 78% to 105%, 90% in average. Measurements were performed on a RT-6000 analyzer (Rayto Co. Shenzhen, China) at 450 nm, then concentrations were calculated using the standard curve. The limit of detection for each assay was 1.0 pg/ml. All samples were measured in duplicate and the results averaged. The intra-assay and inter-assay coefficients of variation were less than 7% and 9%, respectively.
Covariates
Interviewers had been trained to administer a standardized questionnaire to collect demographic data (gender, age, and level of education), lifestyle information (smoking, drinking, and exercise habits), comorbidities (stroke, transient ischemic attack, hypertension, diabetes mellitus, coronary heart disease), physical examination results (heart rate, height, weight, waist circumference, hip circumference) and laboratory test parameters (fasting glucose, blood lipid levels including triglyceride, total cholesterol, low density lipoprotein cholesterol, and high density lipoprotein cholesterol). Laboratory test parameters were examined in the clinical laboratory of the First Affiliated Hospital of Xi’an Jiaotong University. Smoking was defined as ten cigarettes daily for at least six months, with no distinction made between current and past smokers. Drinking was defined as an alcoholic beverage at least once a week. Lack of physical exercise was defined as exercising fewer than three times a week, for thirty minutes. Hypertension and diabetes mellitus were defined as a self-reported medical diagnosis, antihypertensive/anti-diabetic medication use, or were newly diagnosed according to guidelines [35, 36]. Coronary heart disease was defined as a self-reported medical diagnosis or taking medication to treat heart disease. Stroke and transient ischemic attack were defined as a self-reported medical diagnosis or newly diagnosed according to diagnostic criteria [37, 38]. Heart rate was measured for one minute after the subjects had rested for at least five minutes. BMI was calculated as weight divided by height squared (kg/m2). Waist:hip ratio was calculated as waist circumference divided by hip circumference.
Statistical analysis
Means and standard deviations were calculated for all quantitative variables with approximately normal distribution. Median (25% percentile, 75% percentile) was calculated for severely skewed continuous variables, and frequencies and percentages were established for categorical variables.
For univariate analyses, χ 2 tests, t tests, ANOVA, and non-parametric tests were chosen to compare different types of variables. In the logistic regression models, cognitive impairment or possible cognitive impairment (yes or no) were the dependent variables, and the level of plasma Aβ and confounding factors were independent variables. SPSS 18.0 was used for statistical analysis. A p value of less than 0.05 was considered significant.
RESULTS
Demographics and clinical characteristics of the population
Of the 1314 participants aged 40–85 years (mean 55.47±9.94 years), 1180 (89.8%) met the criteria for normal cognition, 85 (6.47%) met the criteria for possible cognitive impairment, and 49 (3.73%) met the criteria for probable cognitive impairment. Detailed information about each group and the differences in covariates in the three groups are presented in Table 1. There were significant differences in age, formal education, diabetes mellitus, stroke and LDL-C between the three groups.
Demographic data and clinical characteristics of the study population
CHD, coronary heart disease; TIA, transient ischemic attack; HR, heart rate; BMI, body mass index; TG, triglyceride; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Plasma Aβ levels in the normal cognition group, possible cognitive impairment group, and probable cognitive impairment group
Plasma Aβ40 and Aβ42 levels were not significantly different across the three groups, while the plasma Aβ42/Aβ40 ratio was (p = 0.009). Post hoc comparisons showed that there was no difference in plasma Aβ40 between groups, but plasma Aβ42 was higher in the possible cognitive impairment group than in the normal cognition group (p = 0.026), and plasma Aβ42/Aβ40 ratio was higher in the possible cognitive impairment group than that in the normal cognition group (p = 0.011) and in the probable cognitive impairment group (p = 0.004). (Table 2)
Comparison of plasma Aβ40, Aβ42, and Aβ42/Aβ40 in the three groups
Significant differences are indicated as follows: *p = 0.011, versus normal cognition group; # p = 0.004, versus probable cognitive impairment group.
Univariate analysis showed that none of the confounding variables (including age, gender, degree of education, smoking, drinking, stroke, transient ischemic attack, hypertension, diabetes mellitus, coronary heart disease) had any effect on plasma Aβ40, Aβ42 or Aβ42/Aβ40 ratio (Table 3).
Comparison of plasma Aβ levels in subgroups of covariates
DM, Diabetes mellitus; CHD, coronary heart disease; TIA, transient ischemic attack.
Multivariate analysis of plasma Aβ and cognitive impairment
Multivariate logistic regression analysis was used to analyze correlations between plasma Aβ and cognitive impairment. First, we chose individuals from the normal cognition group and the possible cognitive impairment group as study subjects, with possible cognitive impairment (yes or no) as the dependent variable, and plasma Aβ parameters (Aβ40, Aβ42 and Aβ42/Aβ40) and covariates as independent variables to establish a logistic regression model. This showed that the Aβ42/Aβ40 ratio (OR = 4.042, 95% CI: 1.248–11.098, p = 0.012) and plasma Aβ42 (OR = 1.036, 95% CI:1.003–1.071, p = 0.031) was higher in the possible cognitive impairment than that in the normal cognition group, but plasma Aβ40 had no difference between groups (OR = 0.991, 95% CI:0.966–1.016, p = 0.476). (Table 4).
Multivariate analysis of plasma Aβ in possible cognitive impairment group and normal cognition group
Next, individuals from the possible cognitive impairment group and the probable cognitive impairment group were chosen as study subjects, probable cognitive impairment (yes or no) was set as the dependent variable, and plasma Aβ parameters (Aβ40, Aβ42, and Aβ42/Aβ40) and covariates as independent variables to establish a logistic regression model. Detailed information of the models is shown in Table 5. Covariates were chosen according to previously described univariate analyses as well as covariates reported to be related to cognition in previous studies.
We found that plasma Aβ42/Aβ40 ratio in the possible cognitive impairment group was higher than that in probable cognitive impairment group (OR = 0.029, 95% CI: 0.002–0.450, p = 0.011) (Table 5).
Multivariate analysis of plasma Aβ in possible cognitive impairment group and probable cognitive impairment group
DISCUSSION
In this population-based study, we found that plasma Aβ42 levels and Aβ42/Aβ40 ratio was higher in subjects with possible cognitive impairment than that in subjects with normal cognition and with probable cognitive impairment. After correcting for confounding factors (including age, gender, degree of education, vascular risk factors, habits of living) in the multivariate logistic regression analysis, the results were consistent with those in the univariate analysis.
The relationship between plasma Aβ level and cognitive impairment in previous cross-sectional studies has been inconsistent. Plasma Aβ42 has been found to be elevated [4, 17], or decreased [18, 19], plasma Aβ40 has been observed to be elevated [16] and the Aβ42/Aβ40 has been shown to be decreased [18–20] in AD patients compared to cognitively normal subjects. These inconsistencies are likely due to different inclusion criteria, exclusion criteria and test methods. In these previous studies, investigators either divided the study population into two groups (cognitively normal versus cognitively impaired, or non-dementia versus dementia) or three groups (normal cognition, mild cognitive impairment, and dementia group).
Unlike the previous studies, in the present study we divided subjects into three groups: normal cognition group, possible cognitive impairment group, and probable cognitive impairment group and found that plasma Aβ42 level was elevated in possible cognitive impairment group than that in normal cognitive group and in probable cognitive impairment group. Subjects in the possible cognitive impairment group had no clinical symptoms and performed normally on the neuropsychological battery; however, their MMSE score was below the cutoff value. These subjects may progress to MCI or dementia in the future, and thus, this group may reflect early stages of the disease, comparable to reports of pre-clinical or pre-symptomatic AD [39]. The result was similar to the previous studies in familial AD patients, in which they found that plasma Aβ42 levels are elevated prior to onset of dementia and declined after the onset of dementia [15]. However, it seems to be opposite to recent two studies [40, 41]. In these studies, authors classified subjects into Aβ (+) group and Aβ (–) group according to PIB-PET imaging or Aβ42 levels in cerebrospinal fluid and found that Aβ (+) group had lower plasma Aβ42 concentration, which was detected using the immunoprecipitation coupled with mass spectrometry. The plasma Aβ42 decrease had more than 90% sensitivity and specificity to discriminated Aβ (+) subjects from Aβ (–) ones. Both Aβ (+) and Aβ (–) group contained normal cognitive, mild cognitive impairment, and dementia subjects, however, they did not compare the levels of plasma Aβ42 among them. In present study, we found that plasma Aβ42 was elevated in the possible cognitive impairment group, but not in the probable cognitive impairment group. Plasma Aβ42 had a tendency to decrease in probable cognitive impairment group comparing with possible cognitive impairment group. These indicated that plasma Aβ42 level was elevated in early stage of AD and declined after cognitive impairment onset.
Some previous studies have shown that plasma Aβ levels are influenced by many factors, including age [42], however we found that none of the identified potential confounding variables had an effect on plasma Aβ levels. As such, the most likely explanation for the difference in plasma Aβ observed between the three groups is cognitive state. The mechanism underlying the association between plasma Aβ and cognitive impairment is not well understood. Aβ has been shown to be generated primarily in the brain, where it can accumulate in the senile plaques of AD patients. Aβ levels are in dynamic equilibrium between CSF and plasma, so increased plasma Aβ may be associated with elevated Aβ generation in the brain and dysfunction of Aβ clearance [43].
The reason for that plasma Aβ42 level increase first and then decline after onset of cognitive impairment is unclear. Prior to diagnosis of cognitive impairment, production of Aβ may be increased in the brain but is not yet deposited in senile plaques, which lead to the increase of Aβ transport from brain into plasma. CSF Aβ42 decreases in typical late onset AD patients is likely due to deposition of Aβ in the brain, leading also to decreased plasma Aβ42 [44].
In present study, we also found that plasma Aβ40 had no difference between the three groups. Hence, the change in plasma Aβ42/Aβ40 is likely driven by the increase of plasma Aβ42 in subjects with possible cognitive impairment. This raises the important question of why we found changes in plasma Aβ42 but not plasma Aβ40. This may be due to the different physiological roles played by Aβ40 and Aβ42. Aβ42 has greater neurotoxicity than Aβ40 and is the main element of senile plaques [45, 46], while Aβ40 can control cerebral vascular constriction, decreasing cerebral flow and cerebral blood volume, and has been shown to play a role in cerebral amyloid angiopathy [47–49]. Therefore, one possible explanation for the specificity of our findings is that Aβ42 levels are more closely related to cognitive impairment than Aβ40.
In summary, this population based cross-sectional study demonstrated that plasma Aβ42 levels and Aβ42/Aβ40 ratio were elevated significantly in patients with possible cognitive impairment, indicating that plasma Aβ42 increases may be more pronounced in early stage of cognitive impairment.
Limitations
First, our study utilized a cross-sectional design, which makes it difficult to determine causal relationships between plasma Aβ and cognitive impairment. It is thus essential to conduct prospective cohort studies to identify the causality of plasma Aβ in cognitive impairment. Second, measurement of Aβ deposition in brain or CSF could not be obtained, which meant that we were unable to determine whether any cognitive impairment observed was due to AD. Finally, investigating other factors that might affect the level of plasma Aβ or cognitive impairment, such as serum creatinine, ApoEɛ4 genotype, the parameters related to Aβ clearance, would improve future studies.