
Abstract
Background:
Hip fracture is a major health problem and a patient’s biological age, comorbidity, and cognitive vulnerability have an impact on its related outcomes. Length of stay (LOS) for these highly vulnerable patients is rather long and the possible causes have not been clearly identified yet.
Objective:
We aimed to assess the main clinical factors associated with protracted LOS, focusing on delirium with or without dementia in older age hip fractured patients.
Methods:
218 subjects (mean age 86.70±6.18 years), admitted to the Orthogeriatric Unit of the Ospedale Policlinico San Martino (Italy), were recruited. All patients received physical and comprehensive geriatric assessment. Days to surgery, days from surgery to rehabilitation, and LOS were recorded. In-hospital and three months’ mortality were reported.
Results:
Prevalent delirium at hospital admission was of 3.1%. 35% of patients developed incident delirium. 56.4% were affected by dementia of Alzheimer-type. In addition, 52% of patients developed delirium superimposed to dementia. Mean LOS was 13.5±4.99 days. Namely, delirium, time to surgery, and complication rate disproportionally affected LOS. The analysis with 3 months mortality, based on cognitive vulnerability profiles, showed how delirium mainly affect short-term mortality in patients with dementia.
Conclusion:
Our exploratory study originally pointed out the high incidence of delirium superimposed to dementia in orthogeriatric wards and how delirium turns to be a moderator of LOS. The results meet the need for additional research by virtue of a deeper understanding of the impact of delirium and dementia on orthogeriatric clinical management and outcomes.
INTRODUCTION
Hip fracture is a major health problem in the western world with increasing incidence and mortality in elderly patients, especially in those aged 85 years and more [1, 2] and approximately one third of patients with hip fracture die within the first year after the fracture event, while one third never regain the previous functional ability after hip injury and hospitalization [3].
Within Europe, Sweden and Norway showed the highest prevalence of hip fracture while France and Switzerland the lowest [4]; Italy shows an intermediate prevalent rate and a great variability among its different counties (Regioni) [5].
Several studies show that the orthogeriatric team and/or the co-management between orthopaedics and geriatricians lead to better clinical outcomes in patients with hip fracture, including mortality [6–8]; however, patient’s chronological age, pre-existing comorbidity, disability, cognitive vulnerability, including dementia and incident delirium all have a major impact on hip fracture related outcomes [9–11].
In addition, length of hospital stay (LOS) and the related complications represent other precipitating factors for exceeding disability and mortality in such a vulnerable population [12], and although LOS is usually considered as a good marker of efficiency and effectiveness of treatments, a shorter LOS was shown to correlate with reduced cost and improved clinical outcomes [13].
On the other hand, a too-short hospital stay can be associated with higher adverse clinical outcomes in elderly hip fractured patients, being this especially true for the older and frail patients [14]. Indeed, even if LOS has fallen over time in both Europe and the United States [15], recent work has suggested that a longer hospital stay after hip fracture is associated with decreased mortality following discharge [16].
The critical differences of healthcare systems in the treatment of hip fractures between European countries could reflect significant difference in LOS prolongation and related clinical outcomes and, namely, in our county, Liguria, the mean age of hip-fractured patients admitted at the emergency room is growingly higher (oldest old patients: >85 years) due to the specific demography of aging [17].
Notwithstanding the presence of an orthogeriatric team, the LOS for these highly vulnerable patients is rather long and the possible causes underlying such a delay in patient’s discharge have not been clearly identified yet.
In this study, we aimed at assessing the main clinical factors associated with protracted LOS and three months’ mortality, in a cohort of octogenarian patients admitted to our hospital for proximal hip fracture, with a specific focus on delirium and delirium superimposed to dementia (SDS).
SUBJECTS AND METHODS
Participants, data collection, and outcomes clinical measurement
A consecutive series of 265 patients with proximal femur fracture and admitted to the Orthogeriatric Unit of the Ospedale Policlinico San Martino-IST (Genoa, Italy) from November 1, 2015 to April 30, 2016, were consecutively recruited. 17 patients refused to participate the study, 5 patients were considered not eligible for surgery, and 25 patients withdrew the study.
A total of 218 subjects (160 women and 58 men; mean age respectively, 86.70±6.18 and 86.09±5.60 years) entered the study.
All patients and/or their next of kin agreed with the study participation after written informed consent was obtained. Ethics approval was granted by the Ethics Committee. All the procedures involving experiments on human subjects are done in accord with the ethical standards of the Committee on Human in accord with the Helsinki Declaration of 1975.
All patients received integrated treatment by a team of orthopaedics and two geriatricians, physiotherapists, and nurses with skills in geriatrics. During weekends and holidays, the integrated team was not available. Geriatricians and orthopaedics had shared responsibility through the patient’s hospital care. The geriatric integrated team performed basal physical and comprehensive geriatric assessment (GCA) [18] for each patient. Namely, the activity of daily living (ADL) [19], the instrumental activity of daily living (IADL) [20], and the Barthel index [21] were used assess the pre-fracture functional status; CIRS (Cumulative Illness Rating Scale) [22] was used to assess patients’ multimorbidity; Mini Nutritional Assessment Short form (MNA–SF) [23] was used to assess the nutritional status.
The diagnosis of dementia at hospital admission was made according to the patients’ clinical history.
Prevalent delirium at hospital admission was diagnosed by an experienced geriatrician, using DSM-V criteria at baseline for operative definition of delirium and 4AT screening test assessment, respectively [24, 25]. This same geriatrician was in charge of patients post operatively. In addition, 4AT screening test [25] was used by a second independent geriatrician to assess incident post-operative delirium after 48 h from surgery. Incident post-operative delirium was used as the reference delirium variable in the results analysis.
The mean number of drugs at hospital admission and patients’ pre-fracture residence were also collected.
Days to surgery, days from surgery to rehabilitation training, and LOS, expressed as the number of consecutive days from admission to discharge, were recorded.
Type of fracture was diagnosed as intra- or extracapsular hip fracture [26].
Osteoporosis treatment was administered at admission as a supplementation of oral vitamin D in all deficient patients (300,000 IUs as in hospital single dose and maintenance dose of 25,000 IUs per week after hospital discharge). The orthogeriatric team managed post-operative pain, malnutrition, and dehydration, according to the American College of Surgeons and the Geriatric Society guidelines [27, 28].
Post-operative complications rate and types were also reported.
Mortality was estimated as in-hospital and three months’ mortality rate.
Statistical analysis
Data are expressed as mean±SD. Descriptive analysis was used to assess patients’ clinical characteristics. Chi square and Fisher exact test was used to assess differences between groups for categorical variables. Mann-Whitney non-parametric test was used to compare quantitative variables according to data distribution of the variables (as assessed by the D’ Agostino-Pearson omnibus normality test).
Pearson’s correlation or Spearman’s rank correlation coefficient were used according to data distribution of the two variables. Kruskal Wallis non-parametric test was used to compared tree or more groups.
A p < 0.05 was considered statistically significant.
Multiple linear regression analysis with backward elimination was performed, considering LOS as dependent variable. Variables entered the model if univariate p < 0.25 and, using backward elimination, remained in the final model if p < 0.05.
All significant measures at univariate analysis were selected with a stepwise approach to be included into the multivariable model (logistic regression analysis), with three months’ mortality as dependent variable. A p-value of 0.10 was used as threshold for inclusion into the model and a p < 0.05 was considered as statistically significant.
Prism 5 software (Graph-pad 5.0 b version) and Excel 2010 (Microsoft Corporation, Redmond, WA) and Stata (v.14; Statacorp) were used for the computation.
RESULTS
The sociodemographic data of patients showed that 73% were females (160 women) and 27% were male (55 men). Mean patients’ age was of 86.70±6.18 years (range 71–103 years) for women and 86.09±5.60 years (range 74–101 years) for men. 66% of patients were oldest old (>85 years).
The clinical characteristics of patients showed high clinical vulnerability, including multimorbidity, functional decline, cognitive impairment and poor nutrition at baseline (Table 1).
Patients’ clinical characteristics at baseline before orthopaedic surgery. Delirium was assessed at baseline (prevalent delirium) and after 48 hours from surgery (incident delirium)
*Mean of standard deviation. BADL, Basic Activities of Daily Living-functional status; Barthel Index, functional status; IADL, Instrumental Activities of Daily Living –functional status; CIRS, Cumulative Illness rate scale for geriatrics –multimorbidity and severity; MNA SF, Mini Nutritional Assessment Short Form –nutritional status; SPMSQ, Short Portable Mental Status questionnaire –cognitive status; 4AT test, rapid assessment test for delirium –screening test for delirium.
91% (n = 198) of the patients were community-dwelling while 9% (n = 20) of them were resident in Nursing Home. A previous fall event was reported indoor in 85% (n = 185) of the examined patients in the last year.
Prevalent delirium at hospital admission, before surgery was of 3.1% (n = 8 out of 218). 56% of patients (123 out of 218 patients) were affected by dementia of Alzheimer-type.
In addition, 35% (n = 77 out of 218) patients developed post-operative incident delirium; in particular, 52% of patients (n = 40 out of 77) developed delirium superimposed to dementia (DSD).
29% of patients had intracapsular hip fracture and 71% of them had extracapsular type fracture.
The time before surgery was 2.25±1.24 days and 62% of patients was submitted to hip replacement within 48 h.
The mean time from surgery to rehabilitation was 4.00±2.15 days (range 1–16 days). The main post-operative complications were post-surgery anemia (n = 143, 66%), delirium (n = 77, 35%), kidney complications (acute pre-renal failure; n = 46, 21%; urinary tract infections; n = 29, 13%), cardiac complications (arrhythmias, acute heart failure) (n = 27, 15%), respiratory complications (infections, acute COPD exacerbation) (n = 27, 12%), pressure ulcer (n = 25, 11%), stroke (n = 3, 1.4%), gastro-intestinal bleeding (n = 3, 1.4%), and orthopaedic complications (n = 2, 1%).
Mean LOS was 13.5±4.99 days (range 1–30 days) (Fig. 1).
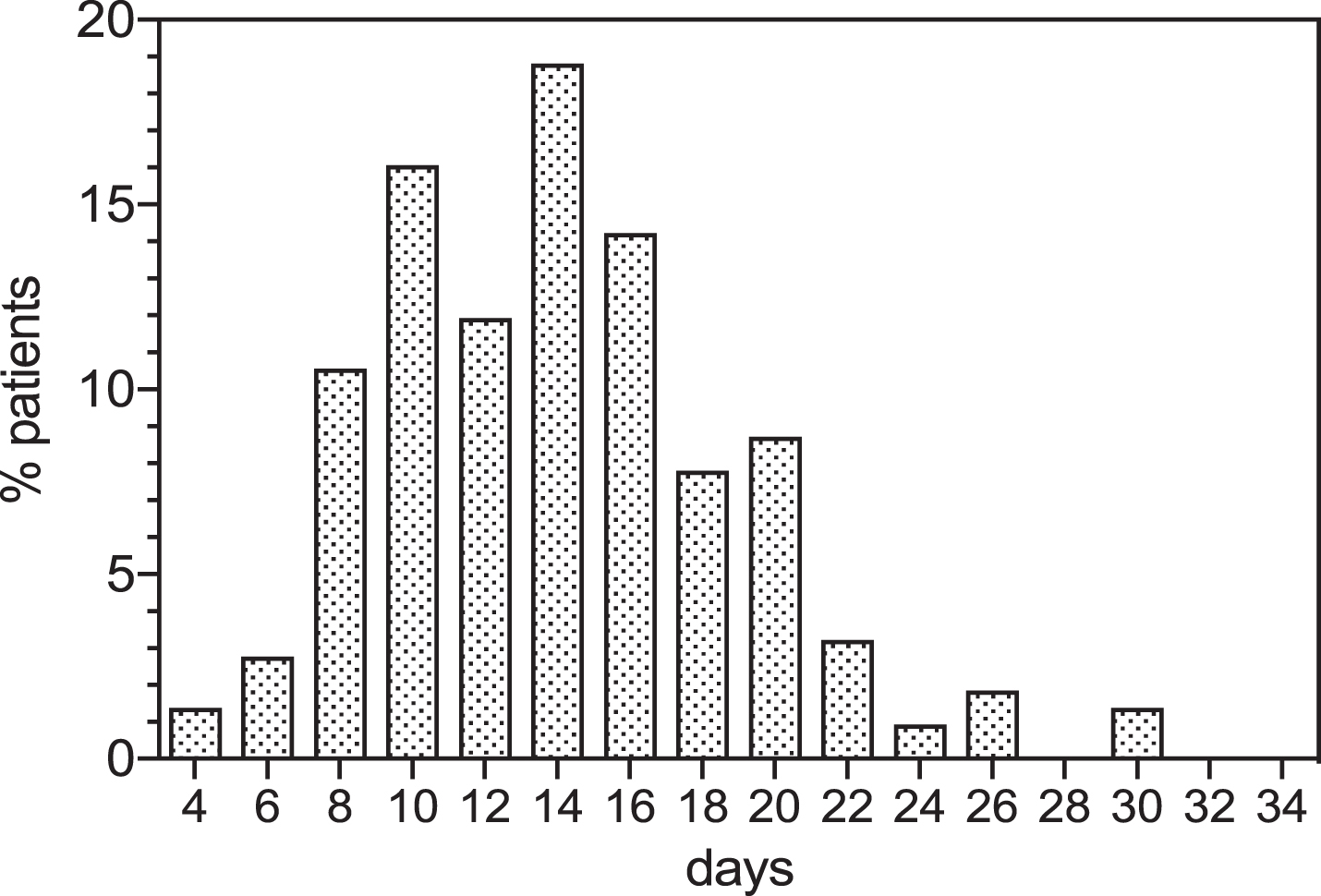
Mean length of stay in the examined cohort of octogenarian patients with hip fracture.
In-hospital mortality was 4.12% and the mortality rate after three months was of 11%. DSD was associated with higher clinical vulnerability due to severe sarcopenia, malnutrition and functional decline, as illustrated in Table 2.
Comparison of patients’ clinical characteristics among the three examined groups: namely, patients without incident delirium, patients with delirium and non- dementia and DSD patients
Barthel index: **without incident delirium versus DSD patients: mean rank difference: 51.8 p < 0.0001. γ incident delirium no-dementia versus DSD patients: mean rank difference: –69.44, p < 0.0001. ADL: ***without incident delirium versus DSD patients: mean rank difference: 44.16; p < 0.0001. f incident delirium non-dementia patients versus DSD patients: mean rank difference: –66.32; p < 0.0001. IADL: Ψ without incident delirium versus DSD patients: mean rank difference: 62.29, p < 0.0001. ϖ incident delirium non-dementia patients versus DSD patients: mean rank difference: –80.89, p < 0.0001. MNA SF: υ without incident delirium versus DSD patients: mean rank difference: 44.25, p < 0.0001. τ incident delirium non-dementia versus DSD patients. Mean rank difference: –50.81, p < 0.002.
The age and gender adjusted multiple linear regression analysis (n = 213; F = 18.72; R = 0.624, p < 0.001), showed that delirium (coeff: 0.93, p < 0.0022), time to surgery (coeff: 1.08, p < 0.0001), complication rate (coeff: 0.34, p < 0.003) were independent predictors for in hospital prolongation.
In addition, the logistic regression analysis showed a trend for MNA (malnutrition) in predicting three month’s mortality (OR = 0.91 (95% CI: 0.81–1.02; p = 0.10). However, when performing the sub analysis, on the basis of patients’ cognitive vulnerability, some clinical associations with short-term mortality were observed.
Namely, in delirious patients, malnutrition (MNA) (n = 77; OR: 0.83; Z = –2.55; 95% Conf int: 0.73–0.96; p = 0.011) was associated with increased three months’ mortality.
Moreover, in patients with dementia, delirium (n = 123; OR = 7.88; Z = 1.94; 95% Conf int: 0.97–63.71; p = 0.053 as a trend), anemia (n = 123; OR = 4.29; Z = 1.83; 95% Conf int: 0.90–20.39; p = 0.067 as a trend), and malnutrition (MNA) (n = 123; OR = 0.81; Z = –2.44; 95% Conf int: 0.69–0.96; p = 0.015) were independent predictors for increased three months’ mortality.
In non-delirious patients, the male gender (n = 78; OR: 4.32; Z = 2.04; 95% Conf int: 1.06–17.63; p = 0.041) was associated with increased three months’ mortality.
Longer rehabilitation time frame (n = 91; OR: 1.27; Z = 1.93; 95% conf int: 0.99–1.63; p = 0.054 as a trend), resulted the most predictive value of increased short-term mortality in patients without dementia.
DISCUSSION
The optimal LOS after hip fracture is still a matter of debate with great variability among countries, ranging from 7 to over 30 days, mainly due to the heterogeneity of healthcare settings and population selection. Several studies have reported that a reduction in LOS [29] is associated with elderly patients’ better clinical and functional recovery, while a Swedish study found that an early patient’s discharge (LOS reduction to up to 11 days) is associated with higher short-term mortality [30]. Notably, a recent Canadian study of hip fractured patients aged 85 or older has shown that a worse quality of care and the shifting of death occurrence to post-acute settings could account for a shorter hospital stay [31]. If this is the case, it is expected that older patients could have higher clinical vulnerability, leading to prolonged LOS, independent of the efforts of the orthogeriatric team.
Notably, the present findings showed that delirium disproportionally affected in hospital stay (Fig. 2). In particular, incident DSD was observed in over 50% of hip fractured patients, who also showed higher clinical vulnerability, including sarcopenia, malnutrition, and functional decline. It is noteworthy that this comorbidity cluster, and in particular malnutrition, is a key determinant of frailty and along with dementia and delirium could accelerate frailty trajectories, being a true moderator of in hospital care [32]. Recent reports [33, 34], have demonstrated how a pre-existing diagnosis of dementia and an age older than 80 years were the most powerful predictors of post-operative delirium after hip fracture, even adjusted for several clinical factors in multivariate models, including comorbidity.
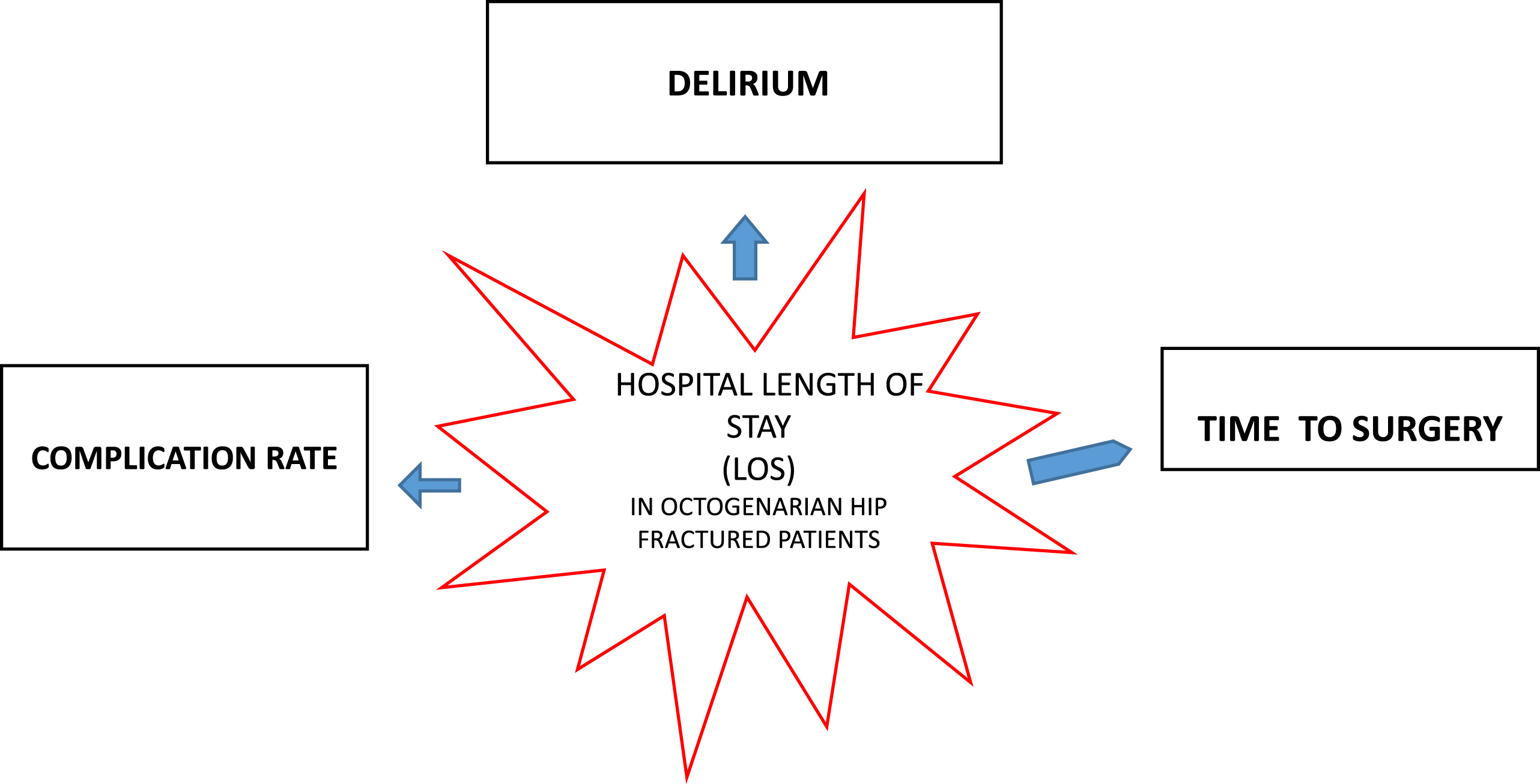
Clinical factors associated with prolonged length of stay in octogenarian hip fractured patients.
A recent meta-analysis [35] that calculated the dimensions of specific determinants of LOS for targeted orthogeriatric care models, has shown that only selected comorbidity and complications rate have been systematically included. Conversely, clinical variables such as time to surgery, delirium and functional status were measuredly infrequently to assess their impact on LOS, with limited and heterogeneous evidence.
To fill this gap and, to our best knowledge, it is among the fewer reports to evaluate the contribution of incident delirium to LOS in the orthogeriatric setting and to estimate the incidence of DSD. In keeping with these present findings, Lee et al. [36] has shown how delirium after hip fracture modified the risk of mortality over the first postoperative year in patients with dementia, with two-fold greater odds of one-year mortality for DSD patients than those without dementia or delirium.
In addition, Mosk et al. [37] has reported how delirium was correlated with higher LOS, complication rate, functional dependence and mortality. In particular, the authors showed a trend toward a higher incidence of 6-month mortality after an episode of delirium in patients with dementia.
Delirium turns to be a key relevant modulator of hospital stay, indicating the major role of cognitive vulnerability in driving hospitalization.
In addition, patients with pre-existing dementia who were comorbid for incident delirium, malnutrition and higher functional decline displayed increased three-month’s mortality. Conversely, in non-delirious and in non-dementia patients, the co-occurrence of higher disability, malnutrition, delayed time to rehabilitation, and male gender were associated with poorer short-term survival. Thus, the geriatric giants (malnutrition, functional decline, dementia, and delirium) drive patient’s clinical trajectories; a deeper understanding of the intertwined role of delirium and dementia could shed light on the role of cognitive vulnerability on adverse outcomes.
Moreover, to fill another gap, these present findings originally describe the incidence of DSD in a dedicated orthogeriatric care. So far, little is known of its natural history in hospitalized elders [38]. A recent study has provided valuable data on the correlates and outcomes of DSD in hospitalized (mainly non-orthogeriatric setting) elders [36, 39], concluding that DSD was associated with higher LOS, functional decline, worsen cognitive trajectory and short-term mortality, compared to dementia individuals.
The present findings indicate how strongly delirium, irrespective of dementia, is able to predict longer LOS. In addition, delirium, even as a trend in our exploratory analysis, seems to drive higher three months’ mortality, especially in subjects with pre-existing dementia. If this is the case, it can be hypothesized that the longitudinal observation of patient’s trajectories will help providing deeper insight into the role of this emerging and threatening cognitive comorbidity [37].
Not least, the results also showed that LOS was prolonged by virtue of delayed surgery (>48 h) compared to patients submitted to early surgery. It is largely accepted that each additional day in time-to-surgery after the first 48 h is associated with increased complication rate and adverse events [40, 41]. Even if early surgical intervention has not been clearly associated with improved mortality or functional recovery, especially in older and comorbid patients [42], growing evidence, mostly retrospective in nature, agreed with the protective role of early surgery in reducing post-operative complications and in hospital length of stay [43].
The main limitations of the study are that it was carried out at a single institution and it may suffer from potential selection bias, referral bias, and information bias. Moreover, there is evidence that frailty in older surgical patients predicts post-operative complications, including LOS [44]. Using a frailty index may help improving the predictive outcomes accuracy, including delirium, with the development of new determinants of LOS [45]. As a further limitation, the differentiation between delirium and dementia is difficult and the use of state-of-the-art methods is still challenging; recently, the observational scale of level of arousal (OSLA) has demonstrated higher accuracy for DSD detection. However, growing evidence indicates that level of consciousness, that is part of 4AT assessment, is considered a valuable clinical indicator for delirium screening strategies in people with dementia [45]. Delirium assessment was carried out at a single assessment point, that prevented delirium duration, severity, and any change of clinical subtype from longitudinal assessment. However, it is generally accepted that the higher incidence of post-operative delirium occurred at day 1 after surgery, reflecting higher stressors such as anesthetics, type of surgery, inflammatory response, and pain. Conversely, delirium incidence later on, during the course of hospital stay, could be related to surgical and non-surgical complications.
On the other hand, the strengths of our study include the prospective 2-year observational design study and methods for determining cognitive status and vulnerability profile at baseline in this difficult population.
As a future object of research, the longitudinal assessment of patients’ trajectories could shed light on the predictive role of cognitive vulnerability (delirium and dementia) in a dedicated orthogeriatric pathway, meeting the need for additional research for the definition of new geriatric care pathways after hip fracture.
Eventually, this is one the fewer studies exploring the ‘’real world” impact of delirium on in hospital stay, in an orthogeriatric acute setting, focusing as well on the emerging incidence of a challenging cognitive vulnerability such as DSD.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0153r3).