
Abstract
Background:
Differences in management and outcomes of oral anticoagulant (OAC) use may exist for people with and without dementia or cognitive impairment (CI).
Objective:
To systematically review the prevalence and safety and effectiveness outcomes of OAC use in people with and without dementia or CI.
Methods:
MEDLINE, EMBASE, and CINAHL were searched for studies reporting prevalence or safety and effectiveness outcomes of OAC use for people with and without dementia, published between 2000 to September 2017. Study selection, data extraction, and quality assessment were performed by two reviewers.
Results:
studies met pre-specified inclusion criteria (21 prevalence studies, 6 outcomes studies). People with dementia had 52% lower odds of receiving OAC compared to people without dementia. Mean OAC prevalence was 32% for people with dementia, compared to 48% without dementia. There was no difference in the composite outcome of embolic events, myocardial infarction, and all-cause death between dementia and non-dementia groups (adjusted hazard ratio (HR) 0.72, 95% CI, 0.45–1.14, p = 0.155). Bleeding rate was lower for people without dementia (HR 0.56, 95% CI, 0.37–0.85). Adverse warfarin events were more common for residents of long-term care with dementia (adjusted incidence rate ratio 1.48, 95% CI, 1.20–1.82). Community-dwelling people with dementia treated with warfarin had poorer anticoagulation control than those without dementia (mean time in therapeutic range (TTR) % ±SD, 38±26 (dementia), 61±27 (no dementia), p < 0.0001).
Conclusion:
A lower proportion of people with dementia received oral anticoagulation compared with people without dementia. People with dementia had higher bleeding risk and poorer anticoagulation control when treated with warfarin.
Keywords
INTRODUCTION
Atrial fibrillation (AF), dementia, and cognitive impairment (CI) are common in older adults, hence they often occur together [1]. AF is a key risk factor for stroke and confers a nearly twofold increased probability of death [2–5]. Further, AF has been associated with an increased risk of developing dementia, with and without prior history of stroke [1, 6]. Diabetes, heart failure, and hypertension are risk factors for both AF and CI [1, 6–9]. Between 26% and 51% of community and hospitalized individuals with AF have CI [10–12]. People with CI have longer durations of hospitalization, poorer post-discharge outcomes, and increased risk of re-hospitalization than people without CI [13, 14].
The presence of dementia or CI affects the management of comorbid chronic disease [15, 16]. Prevention of long-term complications of chronic disease may be de-emphasized in the context of limited life expectancy and changing care goals [16]. Compared to people with AF and normal cognition, people with dementia or CI and AF are less likely to receive vitamin K antagonists (VKA), even though people with dementia demonstrate similar or increased stroke risk [17–21] and increased mortality risk [22, 23]. People with dementia are at increased risk of hemorrhagic complications, such as bleeding linked to falls [24–26]. Further, due to the detrimental effects of amyloid-β on arterial walls, people with dementia may experience increased rates of intracranial hemorrhage [27, 28]. European Society of Cardiology guidelines recommend withholding oral anticoagulant (OAC) in people with dementia only when medication non-adherence is suspected and cannot be assured by a caregiver [22]. American Academy of Neurology guidelines state insufficient evidence is available regarding the safety of OAC for stroke prevention in AF in moderate to severe dementia [29].
The introduction of four direct oral anticoagulants (DOACs): dabigatran, rivaroxaban, apixaban, and edoxaban, has expanded the anticoagulant armamentarium for stroke prevention in AF. Large phase III randomized controlled trials (RCTs) provide evidence of non-inferiority or superiority to warfarin for the prevention of cerebral and systemic embolic events in AF, but reduced risk of intracranial bleeding [30–34]. Well-conducted observational studies support the effectiveness and safety of DOACs compared with warfarin in more inclusive groups [35–39]. DOACs offer practical advantages over VKA therapy as DOAC dosing is based on clinical characteristics and fixed dosing regimens [40]. OAC utilization has increased considerably following DOAC introduction. There has been increasing uptake of DOACs, while the use of VKA has gradually reduced [41–45]. Increasing OAC use has been observed in women [41] and in older people, particularly octogenarians [41, 44]. However, comparative effectiveness and safety studies that include representative samples of people with dementia or CI are lacking [45]. Few people with dementia were eligible to participate in the pivotal DOAC trials [46]. The objective of this systematic review was to identify published data comparing the prevalence and safety and effectiveness outcomes of OAC use in people with AF with and without dementia or cognitive impairment, and to summarize the data using a meta-analysis.
METHODS
The review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [47]. The review protocol was registered in the Prospero International Prospective Register of Systematic Reviews (PROSPERO Number CRD42017050663). Oral anticoagulant medications were defined as oral formulations of VKA, direct thrombin inhibitors and factor Xa inhibitors (Anatomical Therapeutic Chemical (ATC) codes of the World Health Organization: B01AA03 (warfarin), B01AE07 (dabigatran etexilate), B01AF01 (rivaroxaban), B01AF01 (apixaban), and B01AF03 (edoxaban) [48]. Studies of all forms of cognitive impairment and dementia were considered, including mild cognitive impairment, Alzheimer’s disease, vascular dementia, mixed dementias, and Lewy Body dementia.
Search strategy
Studies were identified through a literature search using MEDLINE, EMBASE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases from 1 January 2000 until 30 September 2017. This date range was selected to cover eight to 10 years before and after the introduction of the DOACs. Medical subject headings (MeSH), Emtree terms, keywords and truncated search terms related to dementia or CI (dementia, Alzheimer’s disease, cognitive impairment, cognitive aging) and anticoagulants (anticoagulant, novel oral anticoagulant, NOAC, direct oral anticoagulant, DOAC, apixaban, dabigatran, rivaroxaban, edoxaban, warfarin, VKA, direct thrombin inhibitor, and factor Xa inhibitor) were combined. Searches were limited to English language. Reference lists of identified articles were screened for any additional studies. Full search strategies are available in Supplementary Material 1.
Inclusion and exclusion criteria
Studies of all designs were eligible for inclusion. Studies were included in this review if they reported: original research reporting the prevalence or safety and effectiveness outcomes of oral anticoagulant use for people with and without dementia or CI; prevalence or safety and effectiveness outcomes data separately for people with and without dementia or CI drawn from the same study sample and presented within the study result, for example, sub-group analyses; prevalence data of specific oral anticoagulants or prevalence data for classes of oral anticoagulants such as vitamin K or non-vitamin K antagonists for people with and without dementia or CI;
Studies were excluded if they: reported the prevalence or safety and effectiveness outcomes of oral anticoagulant use in people with dementia or CI only; only reported aggregated results for oral and parenteral anticoagulants combined or antiplatelet and anticoagulant medications combined; did not present original data, or were case reports, conference proceedings, review articles, editorials or letters, or not available in English language.
Study selection
One reviewer (TRA) performed the full search strategy, removed duplicates, and screened article titles. Abstracts were screened independently by two reviewers (TRA, LF). Full-text copies were obtained if studies appeared to meet inclusion criteria or if it was unclear if they met inclusion criteria. Full-text articles were independently reviewed by two investigators (TRA, LF) for inclusion. Discrepancies were discussed with a third investigator (JI) until consensus was reached.
Data extraction
Data were extracted by two reviewers (TRA and LF) independently using a standardized data extraction tool. Data extracted included study details, publication year, study design, study country and setting, study sample characteristics (age, gender), sample size, data sources used, data collection period, prevalence of dementia or CI within study sample, prevalence of OAC use for the overall study sample, prevalence of OAC use among participants with dementia or CI, prevalence of OAC use among participants without dementia or CI, safety and effectiveness outcomes of OAC use for participants with dementia, OAC investigated and OAC indications(s), safety and effectiveness outcomes from OAC use for participants without dementia, dementia type and the method used to identify dementia or CI. Data were extracted separately for participants with and without dementia or CI. Prevalence results include both estimates based on individual oral anticoagulants and grouped oral anticoagulants. When prevalence of OAC use data were clearly reported for these groups, results provided by the authors were used. When data were not clearly reported, but stratification and calculations were possible using the published data, calculations were undertaken to determine prevalence of OAC use among participants with dementia or CI and those without dementia or CI. Data for safety and effectiveness outcomes from OAC use were descriptively extracted from each study and reported separately.
Quality assessment
Two investigators (LF, TRA) independently assessed the methodological quality of prevalence and outcomes studies using adapted versions of the Joanna Briggs Institute critical appraisal tools for analytical cross-sectional studies and cohort studies, respectively [49] (Supplementary Material 2). Quality assessment tools were selected based on study designs of included studies. No RCTs were identified in this systematic review. For cross-sectional prevalence studies, the definition of dementia and medication use, were assessed against pre-specified quality criteria. These quality criteria were applied even when comparing the prevalence of OAC use in people with and without dementia was not the primary objective of each included study (Supplementary Material 2). Any disagreements in assessments were resolved by a third investigator (JI).
Mean OAC prevalence and time trends
The mean OAC prevalence for cardioembolic stroke prevention in AF for dementia/CI and non-dementia/CI groups was calculated by averaging OAC prevalence for all studies combined and stratified by community, hospital, and long term care settings. Trends in OAC prevalence for cardioembolic stroke prevention in AF over the time period 2000 to 2016 were examined by plotting OAC prevalence for dementia/CI and non-dementia/CI groups by mid-year of study observation period. A linear trend line was fit to examine changes in OAC prevalence over time. Two studies did not report time of study observation period and were excluded [50, 51].
Meta-analysis
The prevalence of OAC use for people with AF both with and without dementia or CI and crude odds ratios (OR) were calculated from study data of included articles. Meta-analyses were conducted by pooling all studies, and then stratifying by healthcare settings: community, hospital and long-term care (e.g., residential aged care facilities). Meta-analyses were performed using Review Manager 5.3 [52]. Data were pooled using a random effect model as described by DerSimonian-Laird [53]. The pooled-effect of OAC use for people with and without dementia are reported as OR and 95% confidence intervals (CI). Statistical heterogeneity was assessed among studies by the I2 statistic. To account for both clinical and statistical heterogeneity between studies we utilized a random-effects model. Sensitivity analyses were conducted to investigate the influence of individual studies and characteristics in the pooled ORs for OAC prevalence.
RESULTS
Electronic database searches yielded 4081 articles, of which 27 were finally included in this review (Fig. 1). Of the included 27 studies, 21 studies provided results for prevalence of OAC use for cardioembolic stroke prevention in AF and six studies provided results for safety and effectiveness outcomes from OAC use for cardioembolic stroke prevention in AF among people with and without dementia or CI.
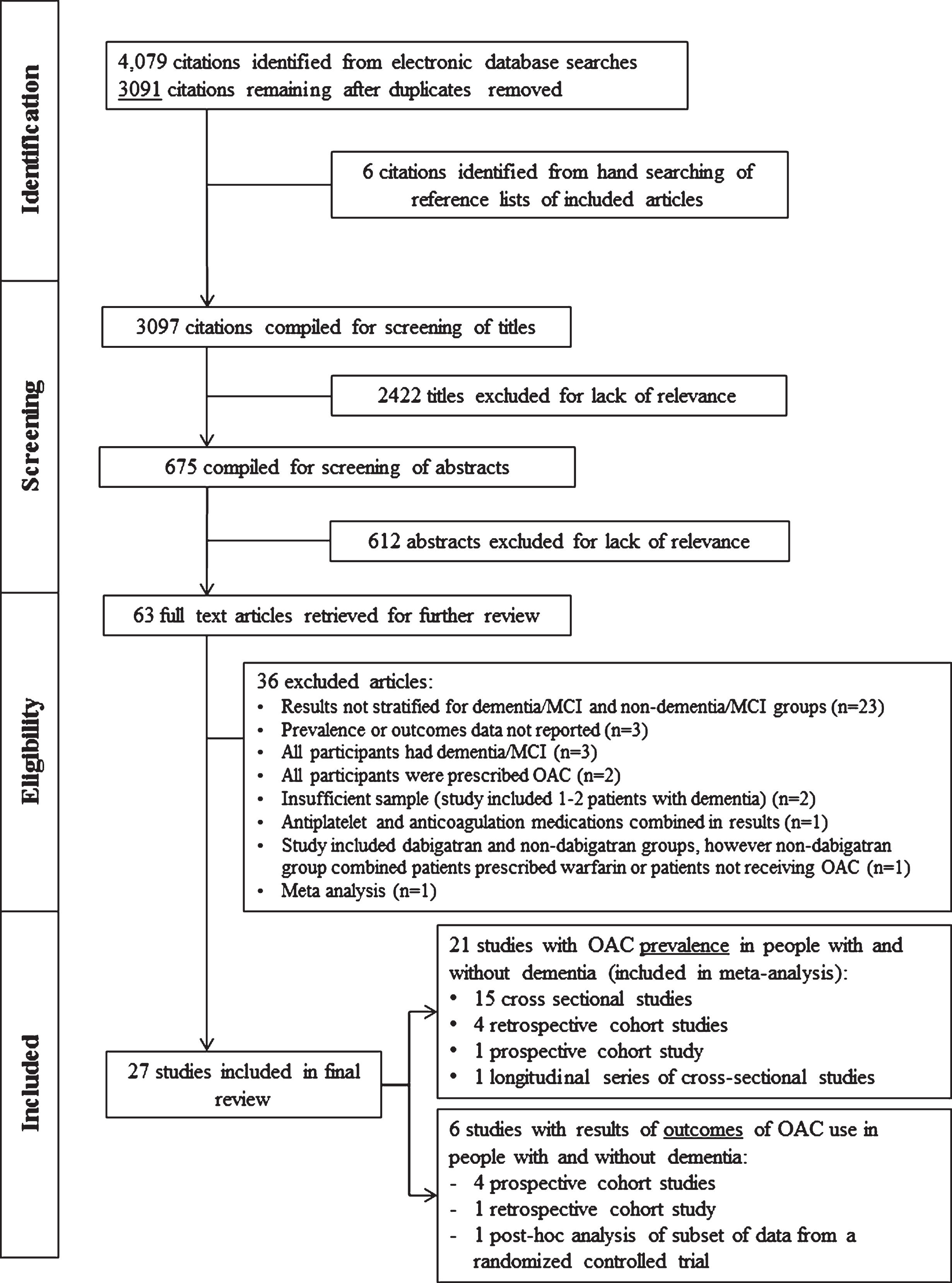
Literature flow diagram of studies identified, screened and included in the meta-analysis and systematic review. OAC, oral anticoagulation.
Study characteristics
Study characteristics are summarized in Table 1. Studies were conducted in United States of America (n = 8) [20, 54–58], Canada (n = 3) [17, 60], United Kingdom (n = 4) [19, 62], and the rest of Europe (n = 11) [50, 63–72], and one study was a multicenter international study [18]. Three prevalence studies utilized data from the Stroke in Atrial Fibrillation Ensemble II (SAFE II) study (multi-site European study) [65, 68].
Methodological characteristics of included studies of prevalence and outcomes of oral anticoagulant use in people with and without dementia or cognitive impairment (by year of publication)
astudy sample was larger, but this group (n-value) were the patients with an identifiable provider in which dementia information was available. AF, atrial fibrillation; CVD, cardiovascular disease; DOAC, direct oral anticoagulant; TIA, transient ischemic attack; MMSE, Mini-Mental State Examination; VTE, venous thromboembolism; INR, international normalized ratio; GP, general practitioner: ICD-9/ICD-10, International Classification of Diseases and Health Related Problems, 9th edition or 10 edition; EMR, Electronic Medical Record; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders 4th edition; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association; NINDS-AIREN, National Institute of Neurological and Communicative Disorders and Stroke and the Association Internationale pour la Recherche et l’Enseignement en Neurosciences.
Of the 21 studies reporting the prevalence of OAC use, 11 were conducted in a hospital setting [17, 70], seven in a community setting [19, 69], and three in long-term care [51, 63]. Fifteen of the studies were cross-sectional designs, four were retrospective cohort studies, one study was a prospective cohort study, and one was a series of cross-sectional studies (Table 1). Data from prevalence studies involved 14,734 people with dementia and 307,961 people without dementia.
Of the six studies that presented safety and effectiveness outcomes data of OAC use, four were conducted in community settings [18, 72], one in a hospital [71] and one in long-term care setting [58]. Four of the studies were retrospective cohort designs [23, 72], one study was a prospective cohort study [58] and one study undertook post-hoc analysis of a subset of data collected in a randomized controlled trial (Table 1) [18].
Warfarin was the anticoagulant investigated for 20 of the 27 studies. One study included dabigatran, rivaroxaban, apixaban, and warfarin [17], one study reviewed warfarin and phenprocoumaron [70], one study reviewed warfarin and acenocoumarol [71], and one study reviewed acenocoumarol alone [72]. Three studies did not specify the exact anticoagulant [50, 64] but stated VKA were used.
The indication for OAC for 24 of the 27 studies was stroke prevention in AF alone. Further, one study included thromboembolic disease, mechanical valve replacement, and stroke prevention in AF indications [58], one study included treatment of venous thromboembolism (VTE) and stroke prevention in AF indications [56], and one study did not specify the indication [50].
Study participant characteristics
The included studies selected their patients based on the presence of AF (n = 13), AF plus incident-or prior-stroke and/or TIA (n = 7), AF/thromboembolic disease/mechanical valve replacement (n = 2), AF plus an additional risk factor for stroke (n = 1), received treatment from a cardiac provider (n = 1), had sustained hip fracture secondary to high-energy fall (n = 1), admitted to a geriatric unit and were receiving OAC (n = 1), were aged 75 years and older with a history of cardiovascular disease (n = 1) (Table 1).
Age was reported as mean with standard deviation, median with range or interquartile range (IQR) and by proportions for specified age groups. Mean age ranged from 70.9±9.5 years to 87.1±5.3 years [18, 63]. Median age ranged from 73 (IQR: 64–81) to 85 years [57, 62]. Three studies stratified by age groups and included 21% of participants aged between 60–69 years [24], 9.4% aged less than 65 years [66], and 16% between 65–75 years [23]. The proportion of females ranged from 45% to 75%. The proportion of participants within each study with dementia or CI ranged from 1% to 75%.
The presence of dementia or CI was variably defined across studies. Dementia was reported for 14 studies, cognitive impairment/disorders/dysfunction was reported for 10 studies, and three studies considered both terms as distinct clinical classifications. Eleven studies identified the presence of dementia from information available in administrative data: International Classification of Diseases and Health Related Problems (ICD) codes for dementia [60, 70], Quality and Outcome Read Codes for dementia [19, 62], dementia diagnosis within the Minimum Data Set [57] or comorbid information/problem lists from hospital electronic medical records [54, 59], electronic nursing home database [57], or stroke registry [17]. Nine studies identified people with dementia or cognitive impairment via medical diagnoses found in medical charts and histories, where some studies specified a formal dementia or geriatric assessment and others did not [20, 68]. Seven studies described dementia diagnosis ascertainment from validated methods such as the full or modified Mini-Mental State Examination (MMSE) or Short Portable Mental Status questionnaire [18, 72](Table 1).
Methodological quality of studies
Fifteen of 21 cross-sectional prevalence studies scored the maximum on quality assessment. Comparative prevalence of OAC use in people with and without dementia was not the main outcome of interest in all 21 studies included in this review. For this reason, we did not assess whether confounding factors were adequately addressed when investigating the difference in prevalence among people with and without dementia or CI. All studies for which prevalence results were obtained compared characteristics of people receiving OAC with those not receiving OAC, which was stratified by presence of dementia (sub-group analyses). Five of the 21 studies from which prevalence data were obtained did not indicate how OAC use was measured which precludes rigorous assessment of whether this was measured validly [50, 70]. For studies that compared safety and effectiveness outcomes of OAC use between dementia and non-dementia groups, three studies scored 10 out of a maximum of 11 points [18, 72] while three studies scored 7 or less points on quality assessment [23, 71]. These three studies were descriptive and did not deal with confounding factors. One study did not provide adequate information to measure OAC use [23]. Full quality assessment results are available in Supplementary Table 1.
Prevalence of oral anticoagulant use
The prevalence of OAC use for cardioembolic stroke prevention in AF was 29% (4221/14539) for people with dementia or CI and 47% (144254/306751) for people without dementia or CI when all study data were combined. Prevalence of OAC use for cardioembolic stroke prevention in AF in people with and without dementia or CI ranged from 8.3% to 64.0% and 7.0% and 75.6%, respectively (Table 2). Mean prevalence of OAC use for cardioembolic stroke prevention in AF for people with dementia was 32% compared with 48% for people without dementia (Fig. 2). For the time period 1998 to 2014, OAC prevalence for cardioembolic stroke prevention in AF increased for both dementia and non-dementia groups across all health care settings combined (Fig. 3).
Outcomes for oral anticoagulant use in persons with and without dementia (by year of publication)
apresented as mean (years)±standard deviation unless otherwise indicated; b112 patients in study sample, but 106 undergoing antithrombotic treatment. TTR. time in therapeutic range; INR, international normalized ratio; OR, odds ratio; HR, Hazard Ratio; CI, confidence interval; N/A, not applicable; AWEs, adverse warfarin-associated events; IRR, incident rate ratio; TT, treatment time; CNS, central nervous system.
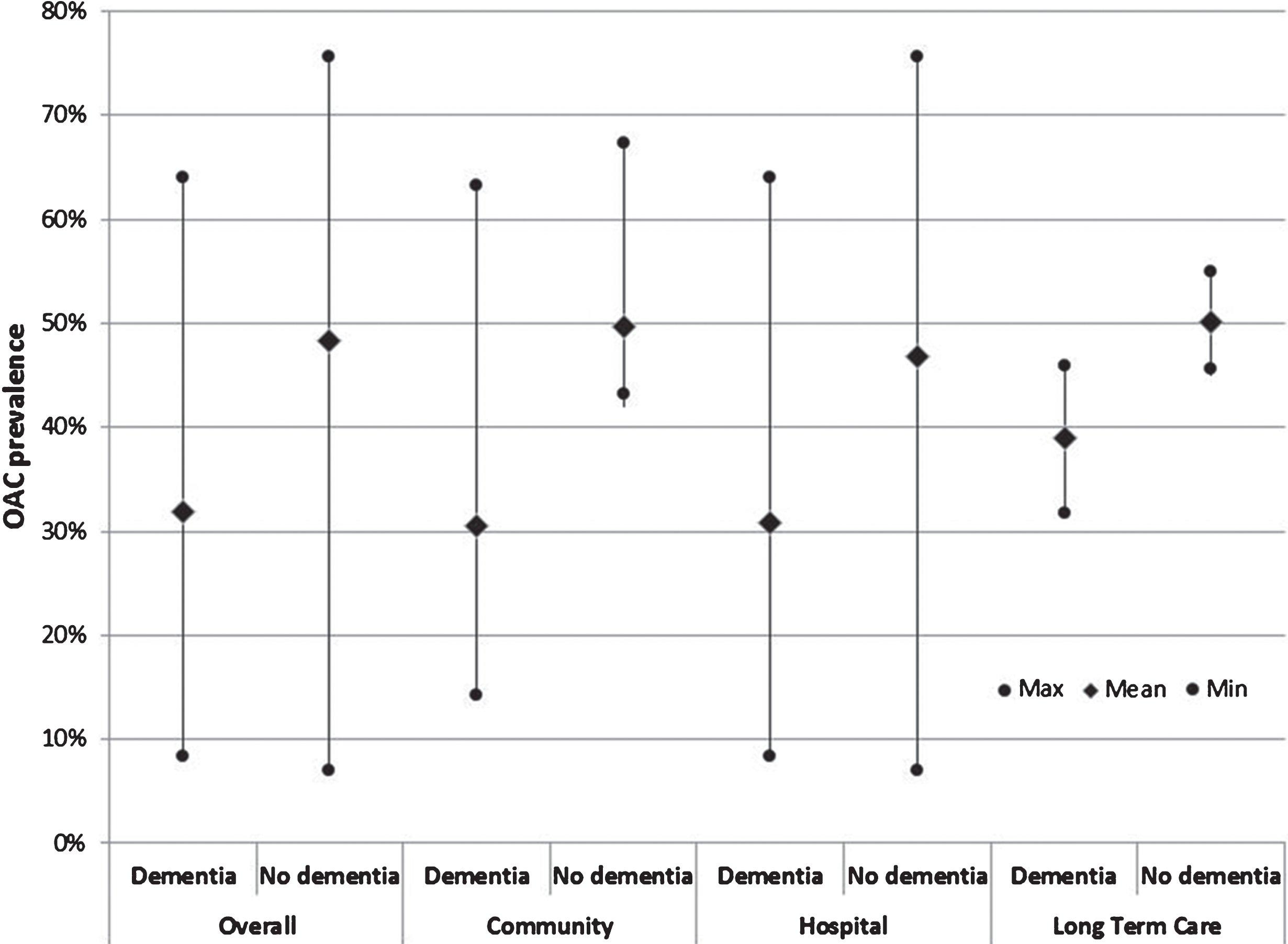
Mean prevalence of OAC use: overall, and stratified by community, hospital and long-term care healthcare settings for dementia/CI and non-dementia/CI groups. OAC, oral anticoagulation; CI, cognitive impairment.
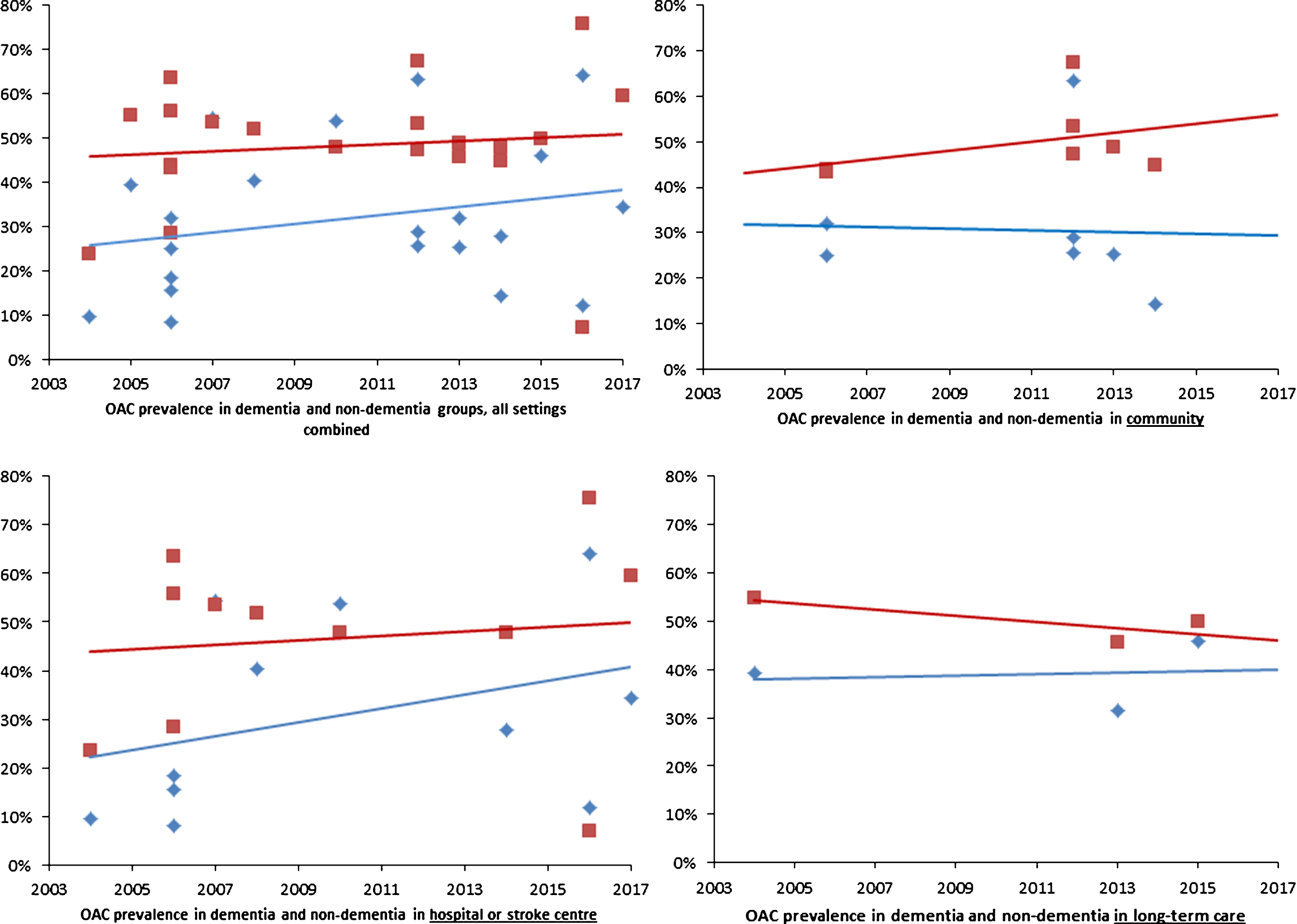
OAC prevalence by mid-year of study observation period: overall and stratified by community, hospital and long-term care healthcare settings for dementia and non-dementia groups, by mid-year of study observation period. Vertical-axis, prevalence of OAC (%); Horizontal-axis, publication year; Red square and trend line, non-dementia; Blue diamond and trend line, dementia/cognitive impairment; OAC, oral anticoagulation.
An overall meta-analysis for all healthcare settings revealed that people with dementia or CI had a significantly lower prevalence of OAC use for cardioembolic stroke prevention in AF compared to people without dementia or CI (OR 0.48, 95% CI = 0.40–0.58, p < 0.00001) (Fig. 4, 1.1.1). Significant statistical heterogeneity between studies was found (I2 = 93%). When stratified by healthcare setting, people with dementia or CI residing in the community had a significantly lower prevalence of OAC use (OR 0.40, 95% CI = 0.31–0.52, p < 0.00001) (Fig. 4, 1.1.2), followed by the people with dementia or CI receiving care in hospital (OR 0.49, 95% CI = 0.33–0.73, p < 0.00001) (Fig. 4, 1.1.3), then followed by residents in long-term care (OR 0.66, 95% CI = 0.45–0.95, p < 0.00006) (Fig. 4, 1.1.4) when compared to people without dementia or CI. Sensitivity analysis revealed no significant influence of any individual studies, study characteristics or dementia classification on the prevalence of OAC in people with and without dementia (Supplementary Material 3, Supplementary Figures 1–5 and 8–9). Additionally, to assess increasing prevalence of OAC over time, a sensitivity analysis was conducted that included studies published during or after 2010 only which showed a similar pooled odds ratio to the overall odds ratio (Supplementary Material 3, Supplementary Figure 2). However, sensitivity analysis that included studies with≥30% of the study sample with a prior history of stroke or TIA demonstrated a higher prevalence of OAC use for cardioembolic stroke prevention in AF compared to people without dementia or CI (OR 0.58, 95% CI = 0.43–0.79, p < 0.00001) (Supplementary Material 3, Supplementary Figure 6).
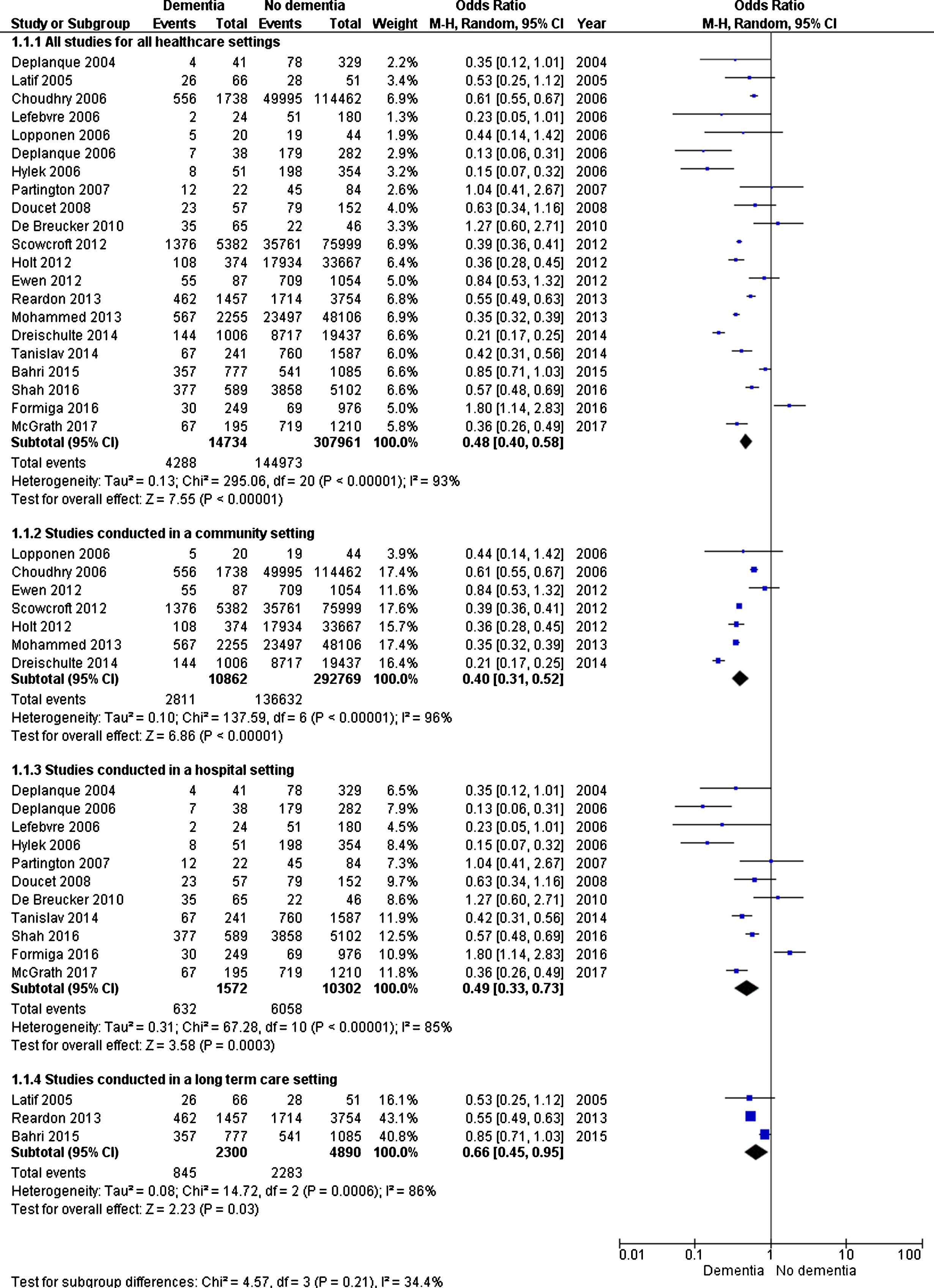
Forest plots of oral anticoagualtion use in people with and without dementia or cognitive impairment for 1.1.1) for all healthcare settings, and then subgroup analysis according to healthcare setting: 1.1.2) studies conducted in the community, 1.1.3) studies conducted in hospitals, and 1.1.4) studies conducted in long-term care.
Safety and effectiveness outcomes of oral anticoagulant use
Safety and effectiveness outcomes of oral anticoagulant use for cardioembolic stroke prevention in AF for people with and without dementia or CI are summarized in Table 3. Differences in effectiveness and safety were reported for dementia/CI and non-dementia/CI groups. It was not possible to conduct a meta-analysis on the safety and effectiveness of OACs. Data on the safety and effectiveness of OACs from each study were reported separately.
Outcomes for oral anticoagulant use in persons with and without dementia (by year of publication)
apresented as mean (years)±standard deviation unless otherwise indicated. b112 patients in study sample, but 106 undergoing antithrombotic treatment. TTR, time in therapeutic range; INR, international normalized ratio; OR, odds ratio; HR, Hazard Ratio; CI, confidence interval; N/A, not applicable; AWEs, adverse warfarin-associated events; IRR, incident rate ratio; TT, treatment time; CNS, central nervous system.
Effectiveness outcomes
One study reported that the composite outcome of stroke, non-central nervous system (CNS) embolism, myocardial infarction (MI), vascular death, and all-cause death was significantly lower for people without dementia than for people with dementia (HR 0.46, 95% CI, 0.27–0.78, p = 0.002). When controlled for TTR, there was no increased risk for the composite outcome in the dementia group (adjusted HR 0.72, 95% CI, 0.45–1.14, p = 0.155) [18]. Results for studies of smaller samples suggested that rates of thrombosis [56], stroke, and mortality [23] were not different for dementia and non-dementia groups (Table 3).
Safety outcomes: Anticoagulation control
Four studies reported varied results regarding anticoagulation control. One study found that people with CI residing in the community had poorer anticoagulation control than people without CI. People with CI (MMSE score < 24) demonstrated lower mean percentage of TTR (mean±standard deviation (SD) 38±26) compared to people without cognitive impairment (MMSE score > 27), (mean (SD) 61±27), p < 0.0001) [71]. Results of another study demonstrated that long-term warfarin users with CI monitored within a pharmacist-managed anticoagulation clinic also spent reduced TTR compared with warfarin users without CI, but the result was not statistically significant (TTR % mean (SD) 61±16 (MMSE≤26), 65±20 (MMSE > 26), p = 0.36 [56]. Further descriptive results in another study indicated patients monitored in an anticoagulation clinic with an MMSE score less than 23 spent 68% of TTR compared with 76% for those with an MMSE 23 and above [72]. In addition, no differences for percentage of days with subtherapeutic, therapeutic and supratherapeutic INR values were found for people with and without dementia in long-term care [58].
Safety outcomes: Adverse events
Total bleeding (minor and major) was found to be significantly lower for people without dementia than for those with dementia (HR) 0.56, 95% CI, 0.37–0.85) [18]. Although, in two studies, no significant differences were found for rates of minor and major bleeding and hemorrhage between dementia and non-dementia groups [23, 56]. Adverse warfarin events (AWEs) (injuries from warfarin) were significantly higher for residents in long-term care with dementia (adjusted incidence rate ratio (IRR) 1.48, 95% CI, 1.20–1.82). Risk of potential or preventable AWEs which constituted an INR value greater than 4.5 was also higher (adjusted IRR 1.36, 95% CI, 1.06–1.76) [58] (Table 3).
DISCUSSION
To our knowledge, this is the first systematic review to investigate the prevalence and outcomes of OAC use for cardioembolic stroke prevention in AF in people with and without dementia or CI. There are three major findings from the review. First, people with dementia had 52% lower odds of receiving OAC for embolic stroke prevention associated with AF than people without dementia. Mean OAC prevalence for people with dementia was 32% compared with 48% for people without dementia. Over the time period 1998 to 2012, OAC prevalence increased for both groups for all healthcare settings combined. Second, six studies compared safety and effectiveness outcomes of OAC use among people with and without dementia, with all studies investigating diverse outcomes. This heterogeneity precludes a meta-analysis of outcomes data to accurately determine whether people with or without dementia have different outcomes of OAC treatment. Third, there is a paucity of data on the prevalence or outcomes of DOAC use in people with dementia. No DOAC safety or effectiveness studies identified by our search strategy have included representative samples of persons with dementia or presented sub-analyses for people with dementia.
People with dementia were less likely to receive OAC than people without dementia. Possible reasons for OAC underuse include: frailty, falls risk, active or prior bleeding, fear of bleeding complications, comorbidities, poor adherence, difficulties with self-monitoring, poor anticoagulation control and polypharmacy [10, 74]. Results from the European Heart Rhythm Association EP Wire survey found that 40% of respondents considered dementia as a key reason not to prescribe OAC. The only more important reason cited was prior or active bleeding or increased bleeding risk [74]. Yet it remains unclear to what extent dementia is associated with lower use of OAC independent of other factors that may contraindicate the prescription of OAC [75, 76]. Ultimately, people with dementia are more likely to experience substantial comorbidity, frailty, and polypharmacy [75]. In a sample of people with AF and dementia at high stroke risk but without increased bleeding risks or absolute contraindications to OAC, it was found that 22% of people received inadequate OAC and 39.5% received no OAC [76]. Further, at the time of dementia diagnosis, 26% of people with AF received warfarin, 37% antiplatelet therapy and 37% did not receive either antiplatelet or OAC [21]. While in people receiving warfarin therapy who were subsequently diagnosed with dementia, 16% remained on warfarin after dementia diagnosis compared with 96.7% of people who were not diagnosed with dementia [77]. Reluctance to prescribe OAC or an inclination to cease OAC in people with dementia could demonstrate that physicians perceive dementia as a limiting factor for OAC, possibly due to perceived increased bleeding risk or lack of adherence [74–76]. Moreover, high thromboembolic risk is often undervalued in ageing individuals with comorbid illness [78] and clinicians may be uncertain whether older, frail people, such as people with dementia could benefit from stroke reduction and whether this counterbalances the risk of bleeding [77, 78]. Our review demonstrates OAC under use in people with dementia and AF and possible higher bleeding risks. However, the risk-benefit of treatment for people with dementia may still provide net clinical benefit. Recent analysis of data from the Swedish Dementia Registry demonstrates lower risk of ischemic stroke and mortality, with only a small increase in any-cause hemorrhage in people with AF and dementia treated with warfarin [21]. Collectively, results may demonstrate that people with dementia and AF should not routinely be excluded from OAC treatment despite a slightly higher bleeding risk.
Over the time period of 1998 to 2012, increasing OAC prevalence was observed for both dementia and non-dementia groups. When stratified by healthcare setting, OAC prevalence for people with dementia in a hospital setting demonstrated the greatest increase. Medical practitioner characteristics and healthcare setting (hospital, community, long term care) have been found to influence OAC prescribing. It has been demonstrated that cardiologists have increased guideline adherence, whereas general practitioners (GPs) were less adherent [79]. Specialist therapeutic recommendations from neurology [70] facilitates the prescription of OAC, and follow-up by cardiologists and younger GPs were strong predictors of VKA treatment [65]. Patients treated at primary stroke centers and large academic hospitals were more likely to receive thromboprophylaxis than patients treated at smaller or general hospitals [34]. Residing in long term care is a negative predictor of being discharged from hospital with OAC [34, 66]. It is not possible to quantify the influence of practitioner characteristics and healthcare setting on our results, however future studies could confirm the effect of these factors on OAC use, particularly for people with dementia and since the introduction of the DOACs.
The results of this study reflect a low prevalence of OAC use for cardioembolic stroke prevention in AF in people with (48%) and without dementia or CI (32%). These results suggest possible under treatment in high risk populations for stroke. These results suggest limited compliance with current stroke prevention guidelines, especially among people with dementia. Alternatively, data included in this was averaged over an extended time period (2000–2017), which could mask the possible magnitude of changing rates of anticoagulation prevalence rates. Further, only one study included in this review provided data on DOAC use in dementia and non-dementia groups. Recent Australian and Norwegian studies have suggested that the overall prevalence of OAC use has increased since the availability of DOACs, particularly for octogenarians [41, 42].
Insufficient studies were identified in this present review to provide enough comparative information or to conduct a meta-analysis for outcomes of OAC use in persons with and without dementia. Two studies demonstrated that people with dementia have poorer anticoagulation control during treatment with VKA and spend more time below therapeutic range than people without dementia [56, 71]. Results that demonstrate a relationship between CI and low TTR should not be directly interpreted as cause and effect, as other reasons could influence low TTR, although, it is clinically intuitive. Safe administration of thrombo-prophylaxis is heavily reliant on self-care. Poor self-care has been identified as a major contributor to hospital readmission and poor health outcomes in patients with heart failure [80]. This could also be expected for AF. People with dementia or CI could have difficulty in acquiring knowledge of chronic disease and medications. A thorough understanding of chronic illness and intact executive function are crucial for managing chronic disease [81, 82]. Limited executive functioning influences the ability to recognize symptoms and make decisions [83], which may result in poor in-range INRs and harm for people with dementia receiving OAC.
The composite outcome of stroke, non-CNS embolism, vascular death, MI, and mortality was found to be significantly higher for people with dementia than those without, but when controlled for TTR, there was no increased risk [18]. This suggests that improving TTR for people with dementia could reduce embolic events. Further, two studies found that thrombosis [56], stroke and mortality [23] were not different for dementia and non-dementia groups, however these studies were limited by small numbers. Conflicting results were found for rates of bleeding events between dementia and non-dementia groups. One study demonstrated increased risk of total bleeding in people with dementia [18] and non-significant differences were found in a further two studies [23, 56].
Poor anticoagulation control is a known deterrent for prescribing OAC [75, 84]. Poor anticoagulation control is closely correlated with embolic stroke, hemorrhage and mortality [85–87]. Given potential difficulties in achieving good anticoagulation control in persons with dementia receiving VKA, this may explain why proportionally less people with cognitive impairment receive anticoagulation than do people without cognitive impairment. DOACs circumvent some limitations of warfarin, such as the need for routine monitoring, and have more predictable pharmacokinetics [40], and are simpler to use than VKA which may improve adherence [88], hence in people with cognitive impairment DOACs could alternatively be considered [89]. Indeed, the European Society of Cardiology guidelines recommend switching those with poor INR control to DOACs [22], but as yet there is little evidence to support this recommendation. DOACs directly inhibit thrombin (dabigatran) and factor Xa (apixaban, rivaroxaban and edoxaban) [90]. DOACs have a rapid onset of action, shorter half-lives, and do not affect factor VII. These mechanisms could decrease bleeding risk; particularly limiting traumatic intracranial bleeding related to falls [91], which is critical when considering OAC for people with dementia. Dementia, per se, can impair medication adherence [92], but comorbidity burden [93] and polypharmacy [94] are known to reduce medication adherence, of which there is increased occurrence in persons with AF and dementia [94]. These areas require thorough investigation to understand the risks and benefits of DOACs in people with dementia.
Limitations
Our study has several limitations. First, the primary data sources have limitations in that comparisons are derived from sub-group analyses of observational studies. These studies did not examine anticoagulation in relation to cognitive status as the main objective. Crude ORs were therefore calculated and no adjustments have been made for variables confounding the prevalence of OAC in dementia/CI and non-dementia/CI groups. Further, information about cognitive status may be limited. For example, dementia and CI were defined in different ways in various studies, and the severity of dementia was not consistently reported. The effect of the use of data obtained from sub-groups of large studies and the heterogeneity of dementia definitions on our findings is unknown. Our meta-analyses showed substantialheterogeneity between studies demonstrated by high I2 values and caution should be used when interpreting findings. Participants of the studies included in this review that were documented to have had CI may have been more likely to have marked CI for it to have been documented. Hence, the observed results may not be generalizable to all people with CI, and this could underestimate the use of OAC in persons with dementia and CI. In addition, we did not assess how the diagnosis or detection of AF occurred for each study. Variability in AF detection rates could influence prescribing of OACs, which could impact the generalizability of the findings of this review to the general population. Further, given the heterogeneity of approaches taken and various safety and effectiveness outcomes reported in the outcomes studies, it was not possible to average or meta-analyze safety and effectiveness outcomes data. The methodological quality of included studies that determined prevalence of OAC use was generally sound. Five prevalence studies did not score maximum points of quality assessment as inclusion criteria were not clearly defined, exposure and outcomes measurements were unclear, and objective, standard criteria for measurement of diagnoses and conditions were not used. Three studies evaluating outcomes of OAC use for people with and without dementia did not provide adequate information to measure exposure (OAC use) and two studies were descriptive and therefore no adjustment for confounding factors was made, which limits the quality. Further, studies were conducted in the UK, the rest of Europe, and North America which may limit the generalizability of results to other countries and healthcare systems.
Conclusion
People with AF who also have dementia are less likely to receive OAC for stroke prevention than people without dementia. There is a dearth of information regarding the outcomes of OAC use for stroke prevention in AF in people with dementia and CI. Given the increasing use of the DOACs, in particular within older age groups, the declining use of warfarin, and the limited generalizability of study findings from pivotal DOAC trials and various observational studies to people with dementia, there is an urgent need for more information. Studies of the safety of OAC specifically in people with AF and dementia of various types, investigating the OAC type, dose, and adherence are urgently needed to guide treatment.
Footnotes
ACKNOWLEDGMENTS
This study was supported by a research grant from the Dementia Australia Research Foundation. LF is supported by a Research Training Scheme PhD Scholarship from the Australian Government: Department of Education and Training. JI is supported by the National Health and Medical Research Council’s Early Career Fellowship. JSB is supported by a National Health and Medical Research Council Dementia Leadership Fellowship.