
Abstract
The association between cerebrovascular disease pathology (measured by white matter hyperintensities, WMH) and brain atrophy in early Alzheimer’s disease (AD) remain to be elucidated. Thus, we investigated how WMH influence neurodegeneration and cognition in prodromal and clinical AD. We examined 51 healthy controls, 35 subjects with mild cognitive impairment (MCI), and 30 AD patients. We tested how total and regional WMH is related to specific grey matter volume (GMV) reductions in MCI and AD compared to controls. Stepwise regression analysis was further performed to investigate the association of GMV and regional WMH volume with global cognition. We found that total WMH volume was highest in AD but showed the strongest association with lower GMV in MCI. Frontal and parietal WMH had the most extensive influence on GMV loss in MCI. Additionally, parietal lobe WMH volume (but not hippocampal atrophy) was significantly associated with global cognition in MCI while smaller hippocampal volume (but not WMH volume) was associated with lower global cognition in AD. Thus, although WMH volume was highest in AD subjects, it had a more pervasive influence on brain structure and cognitive impairment in MCI. Our study thus highlights the importance of early detection of cerebrovascular disease, as its intervention at the MCI stage might potentially slow down neurodegeneration.
INTRODUCTION
Alzheimer’s disease (AD) is a progressive neurodegenerative disease associated with the accumulation of neurofibrillary tangles and neuritic plaques in the brain, resulting in cumulative neuronal damage [1]. Neurobiological changes follow certain atrophy patterns, occurring first in trans-entorhinal regions, entorhinal cortex, and hippocampus, before spreading out into the amygdala and basolateral temporal lobe, and eventually into neocortical regions [2]. Studies show that small-vessel cerebrovascular disease (CeVD) and the prevalence of its markers [3–5], particularly white matter hyperintensities (WMH), indicate that CeVD is an important risk factor for the clinical expression of AD [6, 7]. Indeed, increased WMH burden has been associated with medial temporal lobe atrophy and cognitive impairment in AD [8–10]. Specifically, AD subjects show associations between WMH and global reductions in grey matter volume (GMV) together with frontal and parietal-lobe specific structural alterations [11]. However, the exact pathophysiological process of how WMH and AD neuropathology interact to accelerate degeneration in AD remains to be elucidated. Therefore, it is of interest to study the effect of WMH on atrophy patterns and cognition in AD.
Previous studies have demonstrated that WMH plays a role in grey matter (GM) structural changes and cognitive decline even in the prodromal stage of AD, known as mild cognitive impairment (MCI) [12–18]. MCI is characterized by cognitive impairment but without functional impairment that interferes with daily life [19–22]. Cross-sectional studies illustrate associations between high WMH and decline in perceptual speed and executive function in healthy controls and MCI [13, 23]. Moreover, high WMH volume has been associated with greater risk of progression to MCI [22]. However, the associations between regional WMH distribution and cognition have been mixed. For instance, while some showed higher temporal lesion load associated with global cognition in healthy and patient groups [12], others found higher frontal and temporal WMH as being related to worse cognition in middle-aged healthy adults [24]. Some studies have also highlighted the influence of frontal WMH on executive function in the healthy elderly but temporal WMH influence on memory in AD [25]. Nonetheless, their relationship across different phases of disease requires further study [26].
Previous studies indicate that larger total WMH volume is associated with smaller total GMV [20, 27] and baseline WMH is likely to predict the rate of global GMV decline in healthy elderly [28] and MCI patients [29]. Moreover, it has been suggested that in comparison to region-of-interest based approaches, whole-brain voxel-wise analysis provides greater sensitivity to focal alterations in brain anatomy [30]. Indeed, the association between regional WMH volume as well as other cerebrovascular markers such as lacunes and regional GMV has been a subject of recent investigation [30–32]. While some studies show cross-sectional and longitudinal associations between cerebrovascular disease markers and GM loss in temporal, frontal, and parietal cortices [14, 33], others show no such associations between WMH and cortical thinning [31]. However, previous studies have not simultaneously examined the influence of lobe-wise WMH on whole-brain voxel-wise GMV and their contribution to cognition in healthy controls, MCI, and AD.
In light of these uncertainties, we investigated differences in whole-brain GMV and effect of total and regional WMH on voxel-wise GMV in AD, MCI, and age-matched healthy controls. Based on previous findings regarding the influence of WMH on GMV decline and disease progression, we hypothesized that regional WMH volumes will be mainly associated with GMV loss in frontal, temporal, and parietal lobes in AD and MCI patients. Furthermore, based on mixed findings regarding the influence of lobe-wise WMH on global and domain-specific cognition across the disease spectrum, we evaluated the differential contribution of regional WMH and region-specific GMV loss to cognitive impairment in AD and MCI.
METHODS
Participants
Between April 2013 and April 2016, 165 participants were recruited from tertiary neurology centers in Singapore [34, 35]. Inclusion criteria included diagnosis of MCI based on the NIA-AA criteria [36] or AD based on the NIA-AA criteria [37]. Subjects with MCI were required to have cognitive symptoms, deficits on neuropsychological evaluation, a clinical dementia rating (CDR) score of 0.5, and to not meet criteria for dementia. AD subjects were required to have a CDR of 1. Healthy control subjects were required to have a Mini-Mental State Examination (MMSE) score of 27 or above and a CDR of 0. Exclusion criteria included: 1) a history of alcohol or drug abuse; 2) a current or known history of major depression; 3) comorbid neurodegenerative disease such as Parkinson’s disease; 4) CeVD such as cerebral amyloid angiopathy and prior stroke; 5) neuropsychiatric conditions such as psychosis; 6) presence of contraindications to MRI. Of the 165 participants, 49 of them did not have a FLAIR image. As such, in this study, we only included participants with both T1-weighted and FLAIR images (n = 116). Subjects’ demographics and cognitive characteristics are summarized in Table 1. A total of 116 subjects were included in the study, i.e., healthy controls (n = 51), MCI (n = 35), and AD (n = 30). Subjects were well matched in their demographics, such as age, gender, ethnicity, education, and handedness. This study was approved by the SingHealth institutional ethics review board and written informed consent was obtained for all participants.
Demographics and clinical characteristics of patients and control subjects
AHC > MCI, BHC > AD, CMCI > AD, p < 0.05. Values represent mean (SD). Superscript letters indicate whether group mean was significantly different healthy controls and MCI (A), between healthy controls and AD (B) and between MCI and AD (C), based on post-hoc comparisons (p < 0.05) following one-way ANOVA. Chi-square tests were carried out on gender, handedness, and ethnicity covariates as well as on the three cardiovascular risk factors namely diabetes mellitus, hypertension, and hyperlipidemia. HC, healthy controls; MCI, mild cognitive impairment; AD, Alzheimer’s disease; C, Chinese; M, Malay; I, Indian; O, Other; R. Right; L; Left; WMH, white matter hyperintensities; CDR, Clinical Dementia Rating scale; MMSE, Mini-Mental State Examination. *p < 0.05.
Neuropsychological assessments
All patients underwent clinical, neuropsychological, and MRI assessments. Clinical evaluations were also conducted, including comprehensive physical examination by neurologists and medical history from the patient and reliable informant [37]. The neuropsychological battery was performed by trained psychologists who evaluated global cognition as well as specific cognitive domains, namely episodic memory, executive function, attention, visuospatial abilities, and language abilities. Global cognition was assessed using the MMSE [38] and Montreal Cognitive Assessment [39]. Episodic memory was assessed using 10-word delayed recall [40] and WAIS-IV delayed visual reproduction [41]; executive function was assessed using color trails 2 [42] and frontal assessment battery [43]; attention/working memory was assessed using coding [44] and digit span forward tests [42]; language was assessed using verbal fluency and the 30-word Boston naming test [45]; and visuospatial was assessed using the Alzheimer’s Disease Assessment Scale–Cognitive (ADAS-Cog) constructional praxis test [40] and block design test [42]. Performance on the individual tasks was transformed into z-scores based on normative scores [46–51]. A composite summary index for each cognitive domain was then derived from the corresponding averages of the tests.
Image acquisition
MRI scans were performed at Duke-NUS Medical School, Singapore on a 3T Tim Trio System (Siemens, Erlangen, Germany) (n = 54) or a 3T Prisma Fit System (Siemens, Erlangen, Germany) (n = 62) after scanner upgrade. We obtained high-resolution T1-weighted MPRAGE (Magnetization-Prepared Rapid Gradient Echo) sequences (192 continuous sagittal slices, TR/TE/TI = 2300/2.28/ 900 ms, flip angle = 9°, FOV = 256×240 mm2, matrix = 256×240, isotropic voxel size = 1.0× 1.0×1.0 mm3, bandwidth = 240 Hz/pixel) and FLAIR (Fluid Attenuated Inversion Recovery) sequences (192 continuous sagittal slices, TR/TE/ TI = 5000/387.0/1800 ms, flip angle = 15°, FOV = 256×256 mm2, matrix = 256×256, isotropic voxel size = 1.0×1.0×1.0 mm3) on both scanners using the same parameters. Scan images were reviewed at acquisition and subjects with motion artifacts and gross pathological findings were excluded.
Following procedures reported by Weir and Zuo [52, 53], we quantified the test-retest reliability for MPRAGE on Tim Trio and Prisma Fit in an independent cohort of 23 young healthy controls (11 females, 28.7±6.0 years old, 94.5±24.0 days between scans), and achieved a voxel-correspondent intra-class correlation of 0.96±0.04 for GM, 0.97±0.04 for white matter (WM), and 0.88±0.10 for cerebrospinal fluid (CSF).
White matter hyperintensity derivation
From the FLAIR images, WMH was quantified using an in-house automatic procedure. First, SPM8 (http://www.fil.ion.ucl.ac.uk/spm/) was used to segment GM, WM, and CSF of the T1-weighted images. Combining GM and WM images, we obtained subject-specific brain masks which were used to remove non-brain regions from the FLAIR images. Finally, WMH segmentation and quantification were performed, which involved: 1) modal pixel intensity determined by FLAIR image and 2) threshold-based segmentation using a threshold of 1.45 times the modal pixel intensity. Regional WMH volume for the frontal, parietal, temporal, and occipital lobes were also calculated [54]. Manual visual inspection was performed following the quantification of WMH volume. The total and regional WMH volumes were log transformed to ensure normality.
Volume-based morphometry
We applied the voxel-based morphometry protocol using the VBM8 toolbox (http://dbm.neuro.uni-jena.de/vbm8/) in Statistical Parametric Mapping (SPM12) (http://www.fil.ion.ucl.ac.uk/spm/). This SPM voxel-based morphometry analysis [55] was used to derive subject-level GM, WM, and CSF masks using SPM tissue probability maps from T1-weighted structural data, similar to our previous approach [56], including 1) segmentation of individual T1-weighted images into GM, WM, and CSF using an adaptive Maximum A Posterior (MAP) technique that does not require a priori tissue probabilities [57]; 2) creating a study-specific template using nonlinear DARTEL registration [58]; 3) normalization of each GM/WM segmented map to the customized template in MNI space; 4) modulation by multiplying voxel values by only the nonlinear components of the Jacobian determinants derived from the spatial normalization step, to account for individual brain sizes; 5) smoothing the normalized GM and WM maps with an 8 mm isotropic Gaussian kernel.
Group differences in GMV: To examine group differences, we built a voxel-wise Analysis of Covariates (ANCOVA) general linear model with GMV as the dependent variable, group membership, and total and lobe-wise WMH as the independent variables-of-interest and scanner type, education and ethnicity as covariates. In a secondary analysis, we further controlled for age, gender, and handedness covariates in addition to ethnicity, education, and scanner covariates. The GM regions which showed significant group differences were examined using a threshold of uncorrected p < 0.001 and a minimum cluster size of 100 voxels [30, 32]. Significant clusters in the GM were anatomically identified using the Automated Anatomical Labelling atlas labels.
Associations between GMV and WMH: We also assessed the differential effects of regional WMH on GMV across groups. For this analysis, we set up contrasts to assess which regions showed associations between GMV and total WMH and lobe-wise WMH in AD, MCI, and control groups separately. Scanner type, education, and ethnicity were included as nuisance covariates. The GM regions that showed significant association with total/regional WMH were reported using a threshold of uncorrected p < 0.001 and a minimum cluster size of 100 voxels.
Statistical analyses
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 24.0 (SPSS, Inc; Chicago, IL, USA). Normality for continuous variables was examined using Skewness-Kurtosis and visual inspection of histogram. One-way analysis of variance (ANOVA) was used to examine the differences between groups and chi-square was used to assess differences between categorical variables. Significance was set at a two-tailed probability value of p < 0.05.
To investigate the associations between GMV, regional WMH, and cognition, we performed stepwise multiple linear regression analysis. The independent variables comprised GMV from regions that showed significant group differences in AD compared to controls, total or regional WMH volume while cognitive scores were the main dependent variable. The tested cognitive measures included global cognition (MMSE, Montreal cognitive assessment) and five domain-specific cognition scores (episodic memory, executive function, attention, language, and visuospatial function). The multiple regression analysis was controlled for age, gender, education, handedness, ethnicity, and scanner type. Multiple comparisons correction was carried out across these seven models with a multiple comparisons corrected p-value of p < 0.0071.
RESULTS
AD subjects show less widespread reductions in temporal GMV after controlling for WMH
Total WMH volume was highest in AD subjects compared to both MCI (p = 0.030) and controls (p = 0.003). Before controlling for total WMH, AD subjects showed significantly reduced GMV compared to healthy controls and MCI in frontal, temporal, and parietal regions: right middle frontal gyrus, right superior temporal gyrus, bilateral middle temporal gyrus, bilateral hippocampus and amygdala, left parahippocampus, and right precuneus (Table 2). After controlling for WMH, AD subjects showed less widespread GM atrophy; temporal regions including the left hippocampus, left amygdala, and right superior and middle temporal gyrus showed reductions in GMV (Table 2 and Fig. 1). MCI subjects did not show any difference in GMV compared to controls.
Regions showing group differences in grey matter volume before (a) and after (b) controlling for total white matter hyperintensity volume
Grey matter regions showing atrophy in AD compared to healthy controls and MCI, before and after controlling for total WMH volume. Columns labelled “age, gender, handedness” represent the grey matter volume reduction results after further controlling for age, gender, and handedness covariates. WMH, white matter hyperintensity; HC, healthy controls; MCI, mild cognitive impairment; AD, Alzheimer’s disease.

Group differences in grey matter volume after controlling for total white matter hyperintensity volume. AD subjects showed reduced grey matter volume (purple) in the bilateral hippocampus, middle temporal and superior temporal cortices following correction for total WMH volume. Clusters in blue represent areas of grey matter atrophy in AD subjects prior to controlling for WMH volume. Results are shown at the uncorrected p < 0.001 height threshold with an extent threshold of 100 voxels. Results are displayed on representative sections of the MNI template brain. In coronal and axial slices, the left side of the image corresponds to the left side of the brain. R Mid Temp, right middle temporal cortex; lHIP, left hippocampus.
Total WMH volume has the greatest negative impact on frontal and temporal grey matter in MCI
Total WMH volume had the largest negative influence on GMV in MCI subjects, specifically in temporal and frontal regions (p < 0.001; minimum cluster size = 100 voxels; Fig. 2). We found an overlap between regions atrophied in AD and those showing association between total WMH and reduced GMV in MCI (Supplementary Figure 1).

Impact of total white matter hyperintensity volume on grey matter volume in AD, MCI and healthy controls. Total WMH volume showed an association with grey matter volume in MCI (green) and healthy controls (blue) after controlling for age, gender, handedness, ethnicity, education and scanner covariates. MCI subjects showed the most widespread decreases in grey matter volume across the frontal and temporal lobes while controls showed reduced grey matter volume mainly in frontal and middle temporal regions. Subjects with AD did not show any reduced grey matter volume associated with total WMH. Results are displayed on representative sections of the MNI template brain. The left side of the image corresponds to the left side of the brain. WMH, white matter hyperintensity; AD, Alzheimer’s disease; MCI, mild cognitive impairment; HC, healthy controls.
Frontal and parietal WMH have the largest negative impact on voxel-wise GMV in MCI
Frontal and parietal WMH had the largest negative impact on GMV in MCI (Supplementary Figure 2). Specifically, frontal WMH showed associations with frontal and temporal GMV reductions: bilateral middle frontal gyrus, left precentral gyrus, left superior, middle and inferior temporal gyri, bilateral superior medial frontal gyrus, bilateral parahippocampus, bilateral hippocampus, left insula, and right middle and inferior orbitofrontal gyri (Table 3). After further controlling for age, gender, and handedness, frontal WMH showed associations with frontal and temporal GMV reductions: bilateral middle frontal gyrus, left superior, middle and inferior temporal gyri, bilateral superior medial frontal gyrus, left parahippocampus, left hippocampus (Table 3A, Fig. 3). Furthermore, parietal WMH was associated with frontal and temporal GMV reductions: bilateral superior medial frontal gyrus, bilateral medial and right superior orbitofrontal gyri, right middle frontal gyrus, left precentral gyrus, left inferior and superior temporal gyri, left hippocampus, and left amygdala (Table 3). After further controlling for age, gender, and handedness, parietal WMH was associated with mainly frontal GMV reductions: bilateral superior medial frontal gyrus, right medial orbitofrontal gyri, left precentral and postcentral gyri (Table 3B and Fig. 4).
Negative association between lobe-wise (frontal – A; parietal – B; occipital – C; temporal – D) white matter hyperintensity and gray matter volume
Grey matter regions showing negative association with lobe-wise WMH volume. Columns labelled “age, gender, handedness” represent areas showing such negative associations after further controlling for age, gender, and handedness covariates. WMH, white matter hyperintensity; GMV, gray matter volume; HC, healthy controls; MCI, mild cognitive impairment; AD, Alzheimer’s disease.
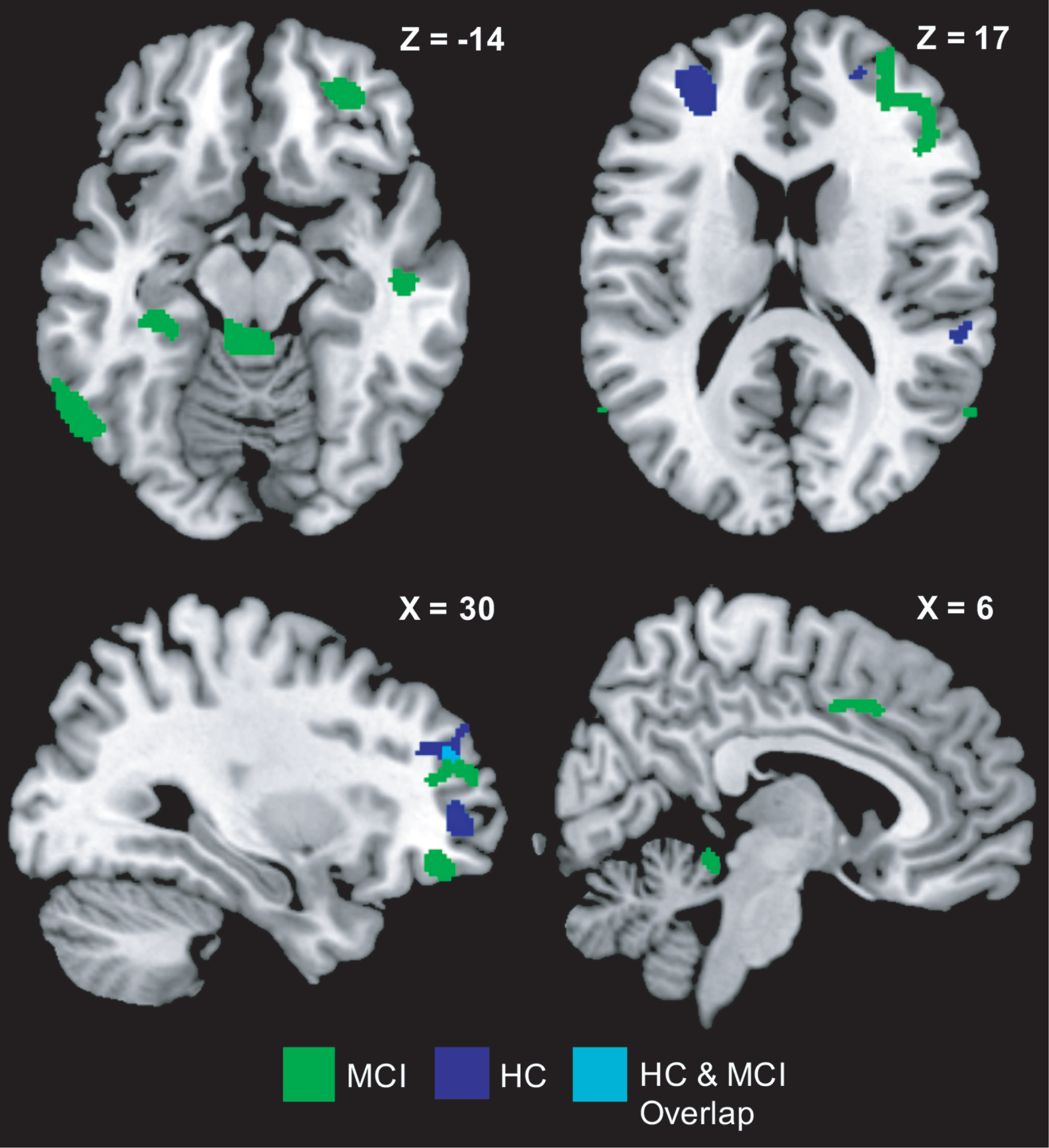
Impact of frontal lobe white matter hyperintensity volume on grey matter volume in AD, MCI, and healthy controls. Greater frontal WMH related to lower grey matter volume in MCI (green) and healthy controls (blue) after controlling for age, gender, handedness, ethnicity, education, and scanner covariates. MCI subjects showed the most widespread WMH-associated decreases in grey matter volume of the bilateral frontal and temporal lobes while controls also showed WMH-related grey matter volume reductions in the bilateral frontal and right temporal regions. Subjects with AD did not show any reduced grey matter volume associated with total WMH. Results are displayed on representative sections of the MNI template brain. In the axial slices, the left side of the image corresponds to the left side of the brain. WMH, white matter hyperintensity; AD, Alzheimer’s disease; MCI, mild cognitive impairment; HC, healthy controls.
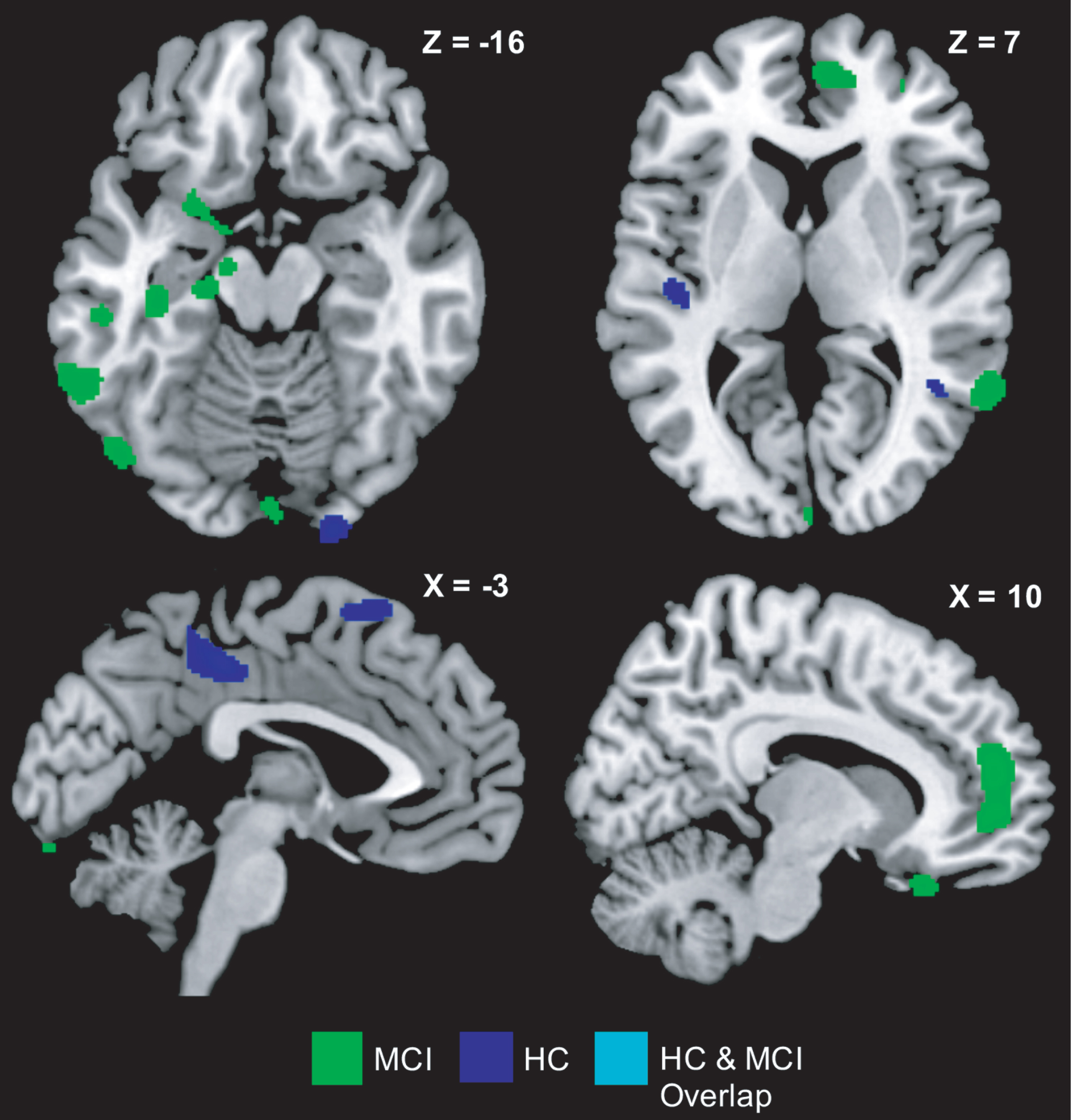
Impact of parietal lobe white matter hyperintensity volume on grey matter volume in AD, MCI and healthy controls. Parietal WMH volume showed an association with grey matter volume in MCI (green) and healthy controls (blue) after controlling for age, gender, handedness, ethnicity, education, and scanner covariates. MCI subjects showed changes in grey matter volume across the bilateral frontal, left temporal regions while controls showed reduced grey matter volume mainly in left precuneus and left middle cingulum regions. Subjects with AD did not show any reduced grey matter volume associated with total WMH. Results are displayed on representative sections of the MNI template brain. In the axial slices, the left side of the image corresponds to the left side of the brain. WMH, white matter hyperintensity; AD, Alzheimer’s disease; MCI, mild cognitive impairment; HC, healthy controls.
In healthy controls, frontal and parietal regional WMH was associated with reductions in frontal, temporal, and parietal GMV. On the one hand, frontal WMH was associated with GMV reductions in bilateral middle and right superior frontal gyri, right superior and middle orbitofrontal gyri, right superior temporal gyrus, and right supramarginal gryus before and after controlling for age, gender, and handedness (Table 3A, Fig. 3). On the other hand, parietal WMH was associated with left supplementary motor area and left superior frontal gyrus atrophy (Table 3B). After further controlling for age, gender, and handedness parietal lobe WMH was associated with GMV reduction in left precuneus and left middle cingulum regions in healthy controls (Table 3B, Fig. 4).
In AD subjects, frontal and parietal regional WMH were associated with right middle and inferior orbitofrontal gyrus GMV reductions but only prior to additionally controlling for age, gender and handedness covariates (Table 3A, B).
Occipital and temporal WMH show smaller influence on voxel-wise GMV in healthy controls and MCI compared to frontal and parietal WMH
Although occipital and temporal WMH showed a negative influence on GMV, the effect of temporal WMH was not as widespread as that of frontal and parietal regional WMH.
Occipital WMH was associated with GMV reductions in right superior and middle temporal gyri, right supramarginal gyrus, right medial orbitofrontal gyrus, and right superior frontal gyrus in healthy controls and remained largely the same after additionally controlling for age, gender and handedness in the model; and bilateral superior medial frontal and orbitofrontal gyri, bilateral middle and inferior triangular frontal gyri, left inferior temporal gyrus, left parahippocampus and hippocampus in MCI (Table 3C). After further controlling for age, gender, and handedness, occipital WMH negatively influenced GMV in bilateral superior medial frontal and orbitofrontal gyri, right middle frontal and inferior triangular frontal gyri, left parahippocampus, and hippocampus in MCI (Table 3C).
Temporal WMH had the largest negative impact on right inferior temporal GMV in healthy controls; and right medial orbitofrontal gyrus, right medial superior frontal gyrus, and right middle and superior frontal gyri in MCI (Table 3D). These results remained after further controlling for age, gender and handedness covariates. There was no impact of occipital and temporal regional WMH on GM structure in AD.
Parietal WMH and hippocampal volume predict global cognition
Of all the features including GMV, regional WMH, and cognition that were included in the step-wise regression model, only parietal lobe WMH was selected as a significant predictor of MMSE scores in MCI (p = 0.025, R2 = 0.145) (Fig. 5A) whereas hippocampal GMV significantly predicted MMSE scores in AD (p = 0.003, R2 = 0.213) (Fig. 5B). There was no association between lobar WMH and global cognition in AD.

AD and MCI subjects showed distinct associations with global cognition. In MCI subjects only, higher parietal lobe WMH was associated with reduced MMSE scores while in AD subjects only, lower hippocampal grey matter volume was associated with decline in MMSE scores. MMSE, Mini-Mental State Examination; WMH, white matter hyperintensity; GMV, grey matter volume; R, right; AD, Alzheimer’s disease; MCI, mild cognitive impairment.
On the other hand, we found no association between lobar WMH or GMV and domain-specific cognition in MCI. In contrast, AD subjects showed positive associations between episodic memory and hippocampal GMV (p = 0.029, B = 0.449) as well as executive function and precuneus GMV (p = 0.020, B = 0.464). There were no associations between domain-specific cognition and lobe-wise WMH volume in AD.
DISCUSSION
A whole brain voxel-wise approach was used to assess the influence of regional WMH volume on GM structure in prodromal and clinical AD. We observed that AD patients exhibited less extensive GM atrophy after controlling for total WMH volume. Importantly, greater regional, i.e., frontal and parietal WMH volumes were associated with the largest negative and most extensive effect on GMV in MCI subjects, compared to AD and healthy controls. Additionally, parietal lobe WMH was associated with lower MMSE scores only in MCI subjects while decreased hippocampal volume was associated with lower MMSE scores only in AD subjects. Our findings thus lend support to the proposition that AD and CeVD-related alterations begin in prodromal stages of disease and are likely to be important co-morbid conditions that influence cognitive decline.
The influence of cerebrovascular disease on neurodegeneration
Previous studies indicate that WMH volume accounts for 23% of the variance of cortical GM atrophy [59] and has the greatest contribution to AD [60]. Similarly, we found that total WMH volume was highest and associated with reduced GMV in AD. Additionally, corroborating with our findings, negative associations between WMH and GMV have been previously observed in the healthy elderly [20]. More importantly, WMH may be associated pathologically to AD since total WMH volume was associated with reduced GMV in the hippocampus, amygdala, and temporal regions in AD in our study. Eminently, neuropathological evidence does show diffuse and focal WM lesions, including WMH, in AD [61]. Although the direction of this association between WMH and cortical degeneration is under conjecture, our findings showed less extensive atrophy when total WMH was controlled for. It is likely that WMH, a marker of CeVD pathology, has additive effects with AD pathology resulting in greater GMV loss. Indeed, concurrent AD and CeVD pathology in prodromal stages has been shown to indicate accelerated disease progression [62–65]. Additionally, WM disruption within areas of WMH may interrupt axonal projections to cortical regions resulting in cortical neuronal loss by retrograde degeneration [59]. Thus, when GMV is corrected for WMH, the amount of GMV is lower because both GMV and WMH are on the same pathological continuum. Therefore, the presence of WMH may result in more pronounced detrimental effects of underlying AD pathology.
We also observed that regions showing atrophy in AD overlapped with regions where reduced GMV associated with total WMH in MCI and healthy controls including the bilateral hippocampus and right middle temporal cortex (Supplementary Figure 1). This offers some insights regarding the early influence of CeVD such that structures that are affected by WMH in prodromal disease stages could provide information on regions that later show the greatest atrophy in AD or regarding further progression to AD [15, 31]. Our findings highlight the importance of distinguishing subjects with high and low WMH load in order to better ascertain extent and pattern of atrophy in AD.
Region-specific WMH influence GMV in prodromal AD
Previous studies have shown that the majority of WMH occur in the frontal lobe and the parietal lobe, similar to the deposition pattern observed in our study [66]. While some studies show the largest effect of WMH on GM atrophy in AD subjects [10, 59], others show that vascular pathology alongside AD pathology is associated with greater hippocampal atrophy in MCI [14, 67]. Such mixed results could be due to hypothesis-driven region-of-interest approaches where all voxels in a region-of-interest are averaged, possibly causing essential signals, especially at early disease stages, to also be averaged out [68]. Here, using a whole-brain voxel-wise approach, we observed that WMH-related effects on atrophy were more profound in MCI and revealed a novel finding that frontal and parietal WMH had the largest negative influence on GMV compared to temporal and occipital WMH. Whole-brain voxel-wise analysis is more sensitive to alterations in GM regions specific to the different disease course [69]. For instance, in our study, both frontal and parietal lobe WMH volume influenced hippocampal, frontal, and temporal GMV in MCI. Similarly, recent studies exhibit associations between high WMH burden, especially in frontal and temporal lobes, and more severe atrophy in AD-related regions. This may be explained as the influence of both vascular pathology and disruptions in WM pathways that link such distant regions in the brain [33, 70]. One postmortem study has also shown that greater axonal and myelin loss were found in WMH in both AD and healthy controls [66]. In addition, previous studies have shown that parietal lobe WMH is associated with more severe disease progression and predictive of MCI conversion to AD over time [3, 71]. On the other hand, studies also point towards the involvement of neurodegenerative factors such as cortical atrophy as well as tau and amyloid-β deposition in the accumulation of WMH via Wallerian degeneration of anatomically connected WM bundles [72–75]. In this regard, postmortem studies do indicate that parietal lobe WMH in AD are associated with demyelination and axonal loss rather than ischemic damage in aged controls [74]. However, due to the lack of amyloid and tau imaging in our current study, no directionality can be presently inferred regarding the association between cortical atrophy and WMH accumulation. Furthermore, although we did not observe significant differences in GMV between MCI and controls, unlike previous studies [76, 77], we have established patterns of GMV reductions (similar to atrophy patterns in AD) as an effect of region-specific WMH, thus indicating that WMH-related derogatory effects on structure appear to be evident early in disease.
Relationship between WMH volume and cognition
We observed that parietal WMH volume was associated with global cognition as measured by MMSE in MCI subjects only. However, such a relationship between WMH and domain-specific cognition was not observed. Such mixed associations between WMH and cognition have also been observed previously in the healthy elderly and MCI [13, 27]. Indeed, studies do indicate that the presence of WMH can itself cause disruptions in fibers connecting spatially distant cortical areas, in turn leading to greater cognitive impairment in concurrent AD and CeVD pathology [78, 79]. Furthermore, such WMH-cognition associations were missing in AD patients. In contrast, consistent with previous findings, hippocampal volume was related to global cognition in AD [80, 81]. This suggests that region-specific WMH volume may contribute to cognitive impairment in MCI rather than in the dementia stage, where atrophy might play a greater role.
Strengths and limitations
The strengths of this study include comprehensive assessments of structural brain measures and neuropsychological assessments and voxel-wise GMV analysis that allows detection of subtle changes in brain volume. Additionally, we assessed the influence of regional WMH on both brain structure and cognition to help provide greater insights into the influence of CeVD on the brain at the healthy control, MCI, and AD stages. However, our study was limited by the cross-sectional study design which prevented us from investigating the effect of WMH on the progression of atrophy patterns. Given the moderate sample size, our voxel-wise GMV findings did not survive corrections for multiple comparisons though stringent height and cluster-level thresholding were performed to minimize false positives. Moreover, we did not have information regarding the amyloid status of our subjects, thus we were unable to assess the influence of such AD risk factors on the relationship between WMH and brain structure. In addition, the MCI group had a mixture of amnestic and non-amnestic MCI subjects; such heterogeneity might confound the relationship between WMH, GMV and cognition. Thus, future work will involve understanding the interaction between AD risk factors, WMH and GMV and age-dependent associations with cognition in prodromal and clinical AD [82].
CONCLUSIONS
In conclusion, we used voxel-wise brain analysis to study the effect of total and regional WMH volumes on GMV in healthy controls, MCI, and AD subjects. We demonstrated that total WMH volume had the largest negative effect on GMV in MCI. Interestingly, the regional distribution of WMH, specifically in the frontal and parietal lobes, also had the largest influence on GMV in MCI. We demonstrated that parietal WMH volume was associated with global cognitive deficits in MCI only. Taken together, the total volume and location of WMHs are important determinants of their clinical relevance [83, 84]. Hence, early detection of WMH and timely intervention could potentially attenuate regional cortical atrophy and cognitive impairment at the MCI stage. Management and modification of risk factors for CeVD are thus likely to be important therapeutic goals in AD.